

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Femoral neck fractures with valgus impaction are considered relatively stable and can be treated with internal fixation using multiple screws123). However, fixation failure due to the excessive sliding of screws, nonunion of the fracture site, and subsequent femoral head osteonecrosis have been reported in many studies456). Furthermore, excessive impaction at the fracture site and subsequent femoral shortening in patients who achieve bone union can lead to deterioration in hip function due to abductor insufficiency and significant leg length discrepancy78). With continued aging of the population, poor outcomes of hip fracture surgery have become a social issue in terms of higher mortality and an increase in medical expenses. For this reason, the ability to predict poor outcomes after internal fixation for femoral neck fracture with valgus impaction is very important.
Many reports in the literature have shown that preoperative deformities of femoral neck fractures with valgus impaction are associated with nonunion or subsequent femoral head osteonecrosis459). Nevertheless, many orthopedic surgeons still perform internal fixation using multiple screws in femoral neck fractures with valgus impaction regardless of the degree of preoperative deformity. This is due to the lack of a widely accepted cut-off value of preoperative deformity for the prediction of reoperation, and the fact that there is still the possibility of achieving bone union in a highly deformed femoral neck fracture with valgus impaction. In addition, there is no obvious consensus concerning the use of primary hip arthroplasty in femoral neck fractures with valgus impaction.
We analyzed surgical outcomes at two institutions after internal fixation using multiple screws in femoral neck fracture with valgus impaction to determine independent outcomes predictors and their cut-off values for nonunion and reoperation. We hypothesized that preoperative deformity was associated with nonunion and reoperation and significant preoperative deformity could lead to a poor surgical outcome, even in patients who achieved bone union.
Go to : 
MATERIALS AND METHODS
Institutional review board approval was obtained (Pusan National University Hospital-1903-008-076). This retrospective, multicenter study analyzed consecutively collected data from databases in two tertiary university hospitals. Between January 2006 and December 2016, 130 femoral neck fractures with valgus impaction treated with internal fixation using multiple screws were identified. A valgus impacted femoral neck fracture was defined when the proximal fragment showed closed apposition and impaction at the medial and lateral side of the fracture site on the anteroposterior (AP) radiograph and the angle of the medial group of trabeculae at the fracture site showed a valgus configuration10). We excluded patients who were followed for fewer than six months (n=16), underwent intraoperative reduction (n=4), were diagnosed with an insufficiency fracture or pathologic fracture (n=1), or had incomplete medical records (n=5).
The surgery was performed on a plain operating table that places the patient in the supine lithotomy position on the unaffected side under fluoroscopic control. A fracture table was not used in order to avoid traction force into the fracture site. We used partially threaded 6.5 mm cannulated screws in an inverted triangle configuration11). The placement of the portal for the inferior screw was made just superior to the lowest level of the lesser trochanter in order to prevent additional stress on the subtrochanteric area. After internal fixation using multiple screws, postoperative rehabilitation, including sitting, continuous passive motion of the hip and knee joints, and wheelchair ambulation were started on the first postoperative day. Standing and partial weight-bearing ambulation with walking aids were allowed two days after surgery.
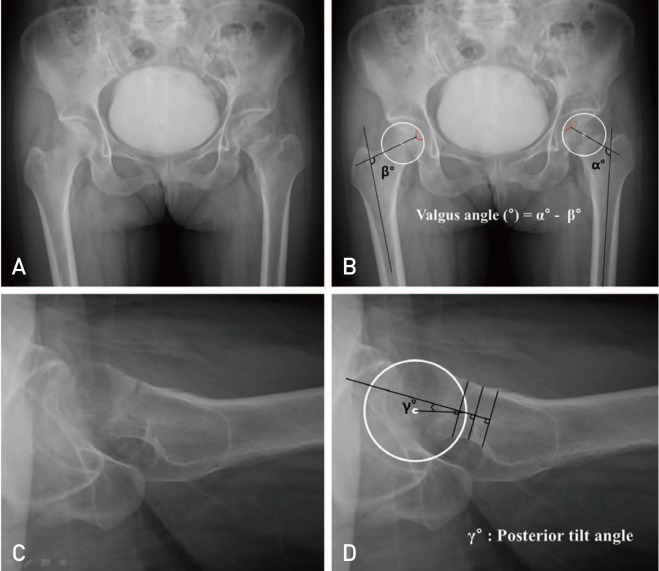
Preoperative characteristics were compared between the groups with and without nonunion and between the groups who had a reoperation or not. Preoperative characteristics included sex, age, pre-injury mobility score, time from injury to operation, American Society of Anesthesiologists class, and body mass index1213). For the radiologic evaluation of preoperative deformity, the valgus angle and the posterior tilt angle were measured. To measure the valgus angle, the femoral head center and the deepest point of the fovea centralis, which is a conspicuous and consistent anatomic landmark on the femoral head, were chosen. We measured the angle formed by the line connecting the deepest point of the fovea centralis and the center of the femoral head and the longitudinal axis of the femoral shaft on the unaffected side (β). In the same way, the angle of the affected side was measured (α). The valgus angle was defined as the difference between these two angles (α–β). The posterior tilt angle was assessed using Palm's method4), measured as the angle between the mid-column line and the radius column line, which is drawn from the center of the caput circle to the crossing of the caput circle and the mid-column line (Fig. 1). AP radiographs of the pelvis were obtained with the patient in the supine position with both femurs internally rotated at 15°. The size of both lesser trochanters was matched to make a valid comparison of measured values.
For the clinical evaluation, we assessed the Harris hip score (HHS) and Palmer and Parker's mobility score at the one-year follow-up. For the radiologic evaluation, we assessed the incidence of nonunion and femoral head osteonecrosis with subsequent segmental collapse, and radiologic measurements, including articulo-trochanteric distance (ATD) index, and the sliding distance of the screws at the one-year follow-up, as reported by Yoon et al.14). Nonunion was defined when there was: 1) greater than 10 mm displacement, 2) progression to varus angulation, 3) greater than 5% change between the axis of the screws, 4) greater than 20 mm posterior translation, 5) femoral head perforation, or 6) no evidence of bone healing with significant hip pain after six months151617). Femoral head osteonecrosis with subsequent segmental collapse was diagnosed in patients who complained of pain and had simple radiographs showing cystic changes and focal bone radiolucency with more than 2 mm of femoral head collapse. When nonunion or femoral head osteonecrosis with subsequent collapse was confirmed, hip arthroplasty was performed.
Pearson's chi-square test or Fisher's exact test for categorical variables and the independent Student's t-test or Mann-Whitney U-test for continuous variables were used to compare preoperative characteristics and surgical outcomes of each group. A multiple logistic regression model was used to determine independent predictors of nonunion and reoperation. Variables showing statistical significance on univariate analysis were included in the multivariate logistic regression analysis, and the forward stepwise method was used to select variables that were eventually included in the model. When the independent predictors were identified as continuous variables, a receiver operating characteristics (ROC) analysis was performed to determine the cut-off value. Values are presented using the area under curve (AUC), P-values, 95% confidence intervals (CI), sensitivity, and 1-specificity. The SPSS software package (ver. 22.0; IBM Corp., Armonk, NY, USA) was used for all statistical analyses. Statistical significance was set at P<0.05.
Go to :
RESULTS
Twenty-six patients were excluded after screening, and 104 patients who met the criteria were enrolled in the present study, including 75 female and 29 male. The mean age was 67.1 years (range, 26–85 years) and the mean follow-up period was 16.3 months (range, 12-36 months). Nonunion was identified in 11 of the 104 patients (10.6%). Femoral head osteonecrosis with subsequent segmental collapse was identified in nine of the 93 patients with bone union (9.7%). The average times to diagnosis of nonunion and femoral head osteonecrosis were 4.2 months (range, 1–6 months) and 13.9 months (range, 6–39 months), respectively. Six patients underwent total hip arthroplasty and five underwent bipolar hemiarthroplasty for the treatment of nonunion. Total hip arthroplasty was performed in all patients with femoral head osteonecrosis.
Comparisons of preoperative characteristics between the groups with and without nonunion, and between the groups who underwent reoperations or not are presented in Table 1 and Table 2. The mean age and posterior tilt angle were 66.0 years and 8.0° in the union group and 76.6 years and 15.8° in the nonunion group, respectively. There were significant differences in age and posterior tilt angle between these two groups. The age and posterior tilt angle between these two groups. The age and posterior tilt angle between these two groups. The age and posterior tilt angle were 65.6 years and 7.6° in the no reoperation group and 73.7 years and 14.0° in the reoperation group, respectively. Significant differences in age and posterior tilt angle were also identified between these two groups.
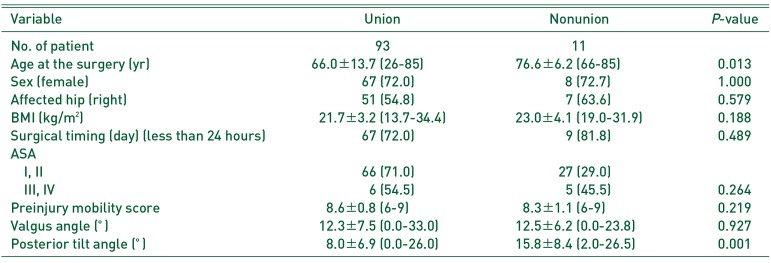
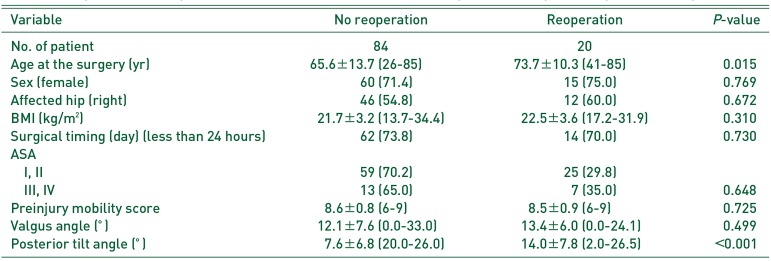
Table 1
Comparison of Preoperative Characteristics between the Union Group and Nonunion Group
![]()
Table 2
Comparison of Preoperative Characteristics between the No Reoperation Group and Reoperation Group
![]()
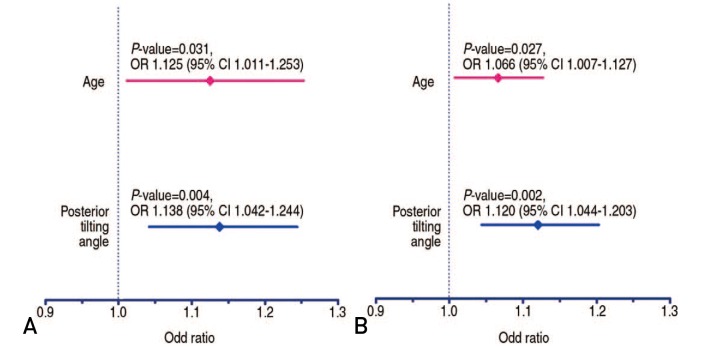
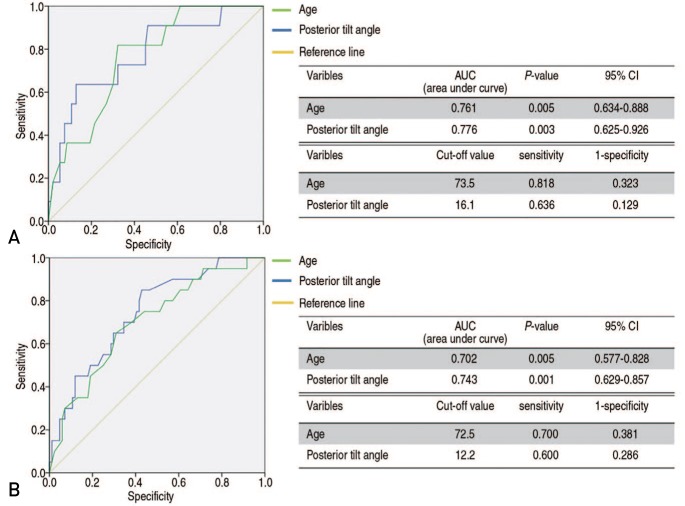
Multiple logistic regression analysis revealed that independent predictors of nonunion were age (P=0.031, adjusted odds ratio [OR]=1.125, 95% CI=1.011–1.253) and posterior tilt angle (P=0.004, adjusted OR=1.138, 95% CI=1.042–1.244). Age and posterior tilt angle were also identified as independent predictors of reoperation (P=0.027, adjusted OR=1.066, 95% CI=1.007–1.127; P=0.002, adjusted OR=1.120, 95% CI=1.044–1.203, respectively) (Fig. 2). ROC analysis revealed that the cut-off values for age and posterior tilt angle for nonunion were 73.5 years (sensitivity=0.818, 1-specificity=0.323, AUC=0.761, P=0.005, 95% CI=0.634–0.888) and 16.1° (sensitivity=0.636, 1-specificity=0.129, AUC=0.776, P=0.003, 95% CI=0.625–0.926), respectively. The cut-off values for age and posterior tilt angle for reoperation were 72.5 years (sensitivity=0.700, 1-specificity=0.381, AUC=0.702, P=0.005, 95% CI=0.577–0.828) and 12.2° (sensitivity=0.600, 1-specificity=0.286, AUC=0.743, P=0.001, 95% CI=0.629–0.857), respectively (Fig. 3).
When we classified 84 patients who did not undergo reoperation into two groups according to the cut-off value of posterior tilt angle for reoperation (13°), the mean ATD index, sliding distance of screws, HHS, and mobility score at one-year follow-up were 8.9, 4.3 mm, 90.4, and 8.3 in the group with less than 13° tilt, respectively, and 14.6, 6.9 mm, 82.5, and 7.6 in the group with greater than 13° tilt, respectively. There were significant differences in the mean ATD index, sliding distance of screws, HHS, and mobility score at the one-year follow-up between the two groups (Table 3).
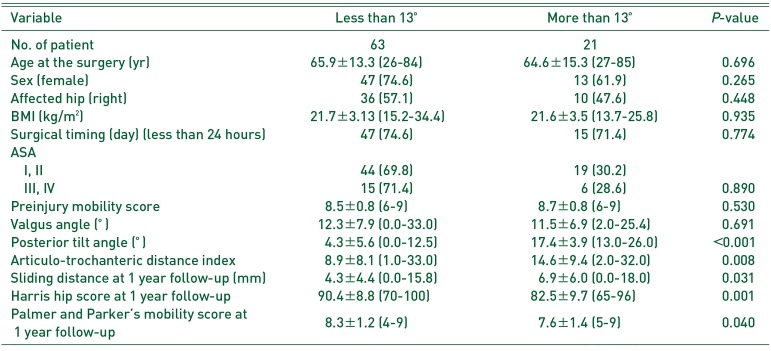
Table 3
Comparison of Preoperative Variable and Postoperative Surgical Outcomes between the Group Who Had Less than 13° of Posterior Tilt Angle and Who Had More than 13° of Posterior Tilt Angle
![]()
Go to :
DISCUSSION
This study reveals that older age and higher posterior tilt angle were independent predictors of nonunion and reoperation in femoral neck fractures with valgus impaction. Cut-off values of each predictor were 73.5 years and 16.1° for nonunion and 72.5 years and 12.2° for reoperation. In particular, patients who had a posterior tilt angle greater than 13°, which was demonstrated as a cut-off value for reoperation, had a significantly higher ATD index and sliding distance of screws, and poorer HHS and mobility score at the one-year follow-up among 84 patients who did not undergo reoperation.
Many previous studies on femoral neck fracture with valgus impaction reported that poor preoperative posterior tilt angle might be associated with nonunion or femoral head osteonecrosis145). Palm et al.4) reported that preoperative posterior tilt in undisplaced (Garden type 1 and 2) femoral neck fractures is thought to influence the rate of reoperation. They introduced a new radiologic measurement method for the posterior tilt of fracture and concluded that their new measurement for posterior tilt appears to be reliable and able to predict the need for reoperation in patients with Garden type 1 and 2 femoral neck fractures. The force acting on the femoral head in sagittal plane, especially with the hip flexed or when lifting, tends to deflect the fracture site posteriorly. We believe that this biomechanical characteristic explain the association between the high posterior tilt angle and high rate of fixation failure.
Nevertheless, many orthopedic surgeons still appear hesitant to perform primary hip arthroplasty in femoral neck fractures with valgus impaction. This is because there is no widely accepted radiologic cut-off value of preoperative deformity to predict poor outcomes and there is still the possibility of achieving bone union even in highly deformed femoral neck fracture with valgus impaction. However, our study demonstrates that patients with a posterior tilt angle greater than 13° showed poorer radiologic and clinical outcomes than those with an angle less than 13°, even though they could achieve bone union. Stockton et al.7) reported that 32% of patients with femoral neck fracture who were treated with cancellous screws experienced severe shortening of greater than 1 cm. Zlowodzki et al.18) reported that femoral neck shortening after femoral neck fracture fixation with multiple cancellous screws has a significant negative impact on physical functioning. We believe that the results of these previous studies have something in common with our investigation. Highly deformed femoral neck fractures can cause excessive shortening of the femoral neck, which can have a negative impact on the surgical outcomes, even when bony union is achieved. Based on these poor outcomes and high failure rates, we believe that it would be better to consider other surgical options, including hip arthroplasty, rather than in situ pinning in highly deformed valgus impacted femoral neck fractures.
It is difficult to conclude that arthroplasty is a better option in highly deformed femoral neck fractures with valgus impaction based on the results of the present study because this is not a comparative study of surgical outcomes between osteosynthesis and arthroplasty. However, many previous studies reported that hip arthroplasty could provide excellent outcomes in elderly patients with displaced femoral neck fractures19202122). Blomfeldt et al.23) reported that patients with femoral neck fractures who underwent arthroplasty did not experience any complications or reoperations between the 24 and 48 month follow-up visits. Furthermore, hip function was significantly better and the decline in health-related quality of life was less pronounced in contrast to that in the internal fixation group. Chammout et al.19) showed that the HHS after total hip arthroplasty in displaced femoral neck fracture reached 90 in the first four years. Although these studies did not investigate the same population as our study, clinical outcomes in the arthroplasty group seem to be better than that in the group with a posterior tilt angle of greater than 13° in the current investigation.
This study has the following limitations. First, this is a retrospective analysis. However, we evaluated 104 consecutive patients from a prospectively collected database treated with the same surgical protocol at two institutions. Second, there might be some measurement errors for the valgus angle, posterior tilt angle, ATD index, and sliding distance of screws. Although, two orthopedic surgeons who did not participate in the operations independently measured the radiologic values, and the averages of each value were used for the analyses to minimize these measurement errors, there might still be other measurement errors related to standardization of proximal femoral rotation on plain radiographs. Third, the follow-up period seems to be relatively short for the assessment of the incidence of femoral head osteonecrosis with subsequent collapse. However, there was no significant differences in the follow-up period between the groups with and without reoperation, and the average follow-up period of both groups was longer than the average time to diagnosis of femoral head osteonecrosis.
Go to :
CONCLUSION
The present study revealed that older age and higher posterior tilt angle were independent predictors of nonunion and reoperation in femoral neck fractures with valgus impaction. In addition, radiologic and clinical outcomes in patients with a posterior tilt angle of greater than 13° were significantly poorer that those of patients with a posterior tilt angle of less than 13°. Based on these results, we believe that primary hip arthroplasty should be considered in patients older than 73 years of age with a posterior tilt angle greater than 13°.
Go to :
 XML Download
XML Download