

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Holmium laser enucleation of the prostate (HoLEP) was first introduced approximately 20 years ago by Fraundorfer and Gilling [1]. Since then, growing evidence has demonstrated that HoLEP offers a more favorable outcome than traditional transurethral resection of prostate (TUR-P) for men with lower urinary tract symptoms (LUTS) and benign prostatic hyperplasia (BPH), in terms of postoperative catheterization time, duration of hospital stay, and intraoperative bleeding [23]. HoLEP shares the same surgical principles as open prostatectomy [4]. Therefore, HoLEP can be performed safely in patients with severe enlargement of the prostate [567]. The short- and long-term efficacy of HoLEP has already been proven in numerous studies [89101112]. Currently, HoLEP has become an important alternative treatment modality to TUR-P or open prostatectomy in men with moderate-to-severe LUTS and BPH [13].
Nevertheless, there are still a significant number of issues that need to be overcome. Among them, the learning curve associated with technical aspects of the surgery is the major negative factor that hinders widespread use of this procedure to date [1415]. There has always been a concern that residual adenoma tissue may remain with an unexperienced hand since multiple surgical planes are formed, especially in an enucleating larger prostate. Furthermore, urinary incontinence after HoLEP is also a significant concern since both transient and permanent urinary incontinence have been reported to occur after the HoLEP procedure [161718]. Several modifications have been introduced to overcome the above issues.
Literature from the early 1990s to the present was reviewed regarding holmium laser resection of the prostate (HoLRP) [19], the original three-lobe HoLEP technique, its modifications, and en bloc enucleation methods with the intention to identify the advantages and disadvantages of each surgical method. It is important to note that it was difficult to understand the full details of the surgical procedures since the actual surgery is performed with the movement of instruments and hands in three-dimensional space (Table 1).
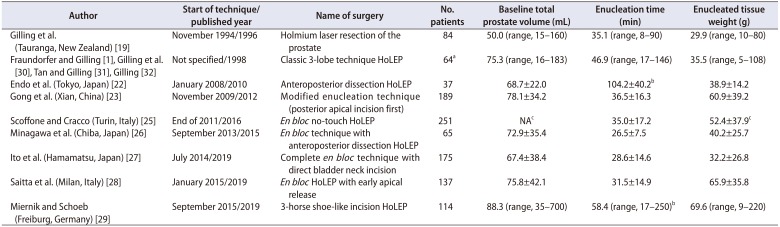
Table 1
Modified methods of the original three-lobe technique and en bloc enucleation methods
| Author | Start of technique/published year | Name of surgery | No. patients | Baseline total prostate volume (mL) | Enucleation time (min) | Enucleated tissue weight (g) |
|---|---|---|---|---|---|---|
| Gilling et al. (Tauranga, New Zealand) [19] | November 1994/1996 | Holmium laser resection of the prostate | 84 | 50.0 (range, 15–160) | 35.1 (range, 8–90) | 29.9 (range, 10–80) |
| Fraundorfer and Gilling [1], Gilling et al. [30], Tan and Gilling [31], Gilling [32] | Not specified/1998 | Classic 3-lobe technique HoLEP | 64a | 75.3 (range, 16–183) | 46.9 (range, 17–146) | 35.5 (range, 5–108) |
| Endo et al. (Tokyo, Japan) [22] | January 2008/2010 | Anteroposterior dissection HoLEP | 37 | 68.7±22.0 | 104.2±40.2b | 38.9±14.2 |
| Gong et al. (Xian, China) [23] | November 2009/2012 | Modified enucleation technique (posterior apical incision first) | 189 | 78.1±34.2 | 36.5±16.3 | 60.9±39.2 |
| Scoffone and Cracco (Turin, Italy) [25] | End of 2011/2016 | En bloc no-touch HoLEP | 251 | NAc | 35.0±17.2 | 52.4±37.9c |
| Minagawa et al. (Chiba, Japan) [26] | September 2013/2015 | En bloc technique with anteroposterior dissection HoLEP | 65 | 72.9±35.4 | 26.5±7.5 | 40.2±25.7 |
| Ito et al. (Hamamatsu, Japan) [27] | July 2014/2019 | Complete en bloc technique with direct bladder neck incision | 175 | 67.4±38.4 | 28.6±14.6 | 32.2±26.8 |
| Saitta et al. (Milan, Italy) [28] | January 2015/2019 | En bloc HoLEP with early apical release | 137 | 75.8±42.1 | 31.5±14.9 | 65.9±35.8 |
| Miernik and Schoeb (Freiburg, Germany) [29] | September 2015/2019 | 3-horse shoe-like incision HoLEP | 114 | 88.3 (range, 35–700) | 58.4 (range, 17–250)b | 69.6 (range, 9–220) |
![]()
Go to : 
HISTORICAL CONSIDERATIONS
Historically, urologists in New Zealand have made significant contributions to BPH surgeries using a holmium laser. The first attempt to use a holmium laser for transurethral prostatectomy was made by Gilling et al. [20], who combined the use of a holmium laser with an Nd:YAG laser to perform a so-called combined endoscopic laser ablation of the prostate or CELAP; this procedure was used to reduce short-term sequelae caused by Nd:YAG laser prostatectomy.
With accumulating experience on using a holmium laser, it has become clear that it has sufficient hemostatic effect on prostatic tissue. In this regard, holmium laser ablation of the prostate (HoLAP) technique was developed [21]. However, ablation did not yield prostate tissue that was suitable for detecting cancer, and the hemostatic effect was not superior to that of other lasers; hence, HoLAP was not widely used. In 1996, Gilling et al. [19] developed a new surgical procedure, HoLRP, which involved excising the prostate with a holmium laser. HoLRP was later applied to BPH surgery, which became the precursor surgery of HoLEP.
Subsequently, a morcellator was introduced in urological practice by Fraundorfer and Gilling [1]. At this time, the most recent modification of the HoLRP technique had been completed as an enucleation of prostatic adenoma. Following the development of the morcellator, large prostatic fragments could be pulled out of the bladder. HoLRP was no longer extended, and soon it was replaced with HoLEP. This enucleation method has become a powerful method for treating enlarged prostates of any size. The originally developed HoLEP technique was the three-lobe technique, which requires three longitudinal incisions from the bladder neck to the distal part of the prostatic adenoma, followed by enucleation of the median lobe and subsequent enucleation of both lateral lobes.
Over the years, many modifications have been developed, and the original surgical technique has evolved considerably [222324]. The en bloc nucleation is a method of enucleating the three prostatic lobes from the prostatic capsule as a whole lump, and several en bloc enucleation methods have emerged worldwide since 2010 [2526272829]. The en bloc method was developed to maintain the prostatic capsule plane and the urethral sphincter while removing the prostate without leaving residual prostate tissue. In parallel, the original surgical technique is continually being refined and evolving.
Go to :
CLASSIC GILLING'S THREE-LOBE TECHNIQUE
Gilling's method is based on the enucleation of three lobes, where the median and both lateral lobes are enucleated independently in retrograde fashion by making three longitudinal incisions from the apex to the bladder neck. The original technique was reported in 1998 in 14 BPH patients and encompassed the first HoLEP procedure combined with the morcellator [1]. The authors later published their extensive experience in 64 patients; however, the technical aspects of the surgical procedure are not portrayed in detail in these papers, and these were described in detail later [303132]. Separately, Kuo et al. [33] and Kim et al. [24] described this three-lobe technique in detail in 2003 and 2013, respectively; the latest update of the latter will be mentioned at the end of this paper.
As described in the historical section, the most advanced modification of the HoLRP method [19] was enucleation, which later became HoLEP formally when it was combined with morcellation technology [1]. In this respect, it is necessary to briefly describe the HoLRP method. The HoLRP method begins by two separate bladder neck incisions with subsequent transverse incisions at the proximal verumontanum to remove the median lobe. The upward incisions start from the lower edges of each lateral lobe distal to the verumontanum, at a 5 o'clock position for the left lobe and a 7 o'clock position for the right lateral lobe. The downward incision for the left lateral lobe starts at the 1 o'clock position, and that for the right lateral lobe commences at the 11 o'clock position. Connecting incisions are made at the 5 o'clock position (left) and the 7 o'clock position (right). There was no description for the management of anterior commissure at the 12 o'clock position.
After the morcellator became available, this HoLRP surgical technique evolved into HoLEP. Similar to HoLRP, the bladder neck at the 5 o'clock position and 7 o'clock position is incised vertically to the verumontanum; a further deep incision is made until a surgical capsule is reached. If there is no discernable median lobe, only one longitudinal incision may be made at the 6 o'clock position. Once the two incisions are complete, they are connected just above the verumontanum to allow enucleation of the median lobe. As the tip of the laser moves side-to-side toward the bladder neck, the median lobe is dissected from the prostatic capsule. The median lobe is completely separated from the bladder neck before being placed into the bladder for later morcellation. Next, both lateral lobes are enucleated; the medial edges of both lateral lobes, formed by the previous step for removing the median lobe, are extended to the apex to more clearly define the apical anatomy. The enucleation of the left lateral lobe is proceeded by sweeping circumferentially until the 2 o'clock position is reached.
A longitudinal incision should be made at the 12 o'clock position of the bladder neck, extended in the distal direction; the incision should be deepened until the underlying capsular plane is reached. The space between the adenoma and the capsule is developed laterally and circumferentially with a sweeping motion. The enucleation from the upper and lower parts is connected to each other at the 2 o'clock position of the apex. Again, there is no specific mention of how the incision is made near the sphincter, especially at the 12 o'clock position of the apex. After further enucleating the left lateral lobe, it is placed into the bladder, and the right lateral lobe is enucleated similarly to the left lateral lobe.
Kuo et al. [33] described a few additional technical details. They explained that enucleation of the right lateral lobe should precede the left lobe. They also suggested that a lower power setting (2 J, 40 Hz) during apical dissection is needed to reduce thermal injury to the sphincter. They emphasized that the dissection should begin at a point slightly proximal to the apex to preserve the apical fat pad, so as to protect sphincteric integrity.
After the development of this three-lobe technique, HoLEP gained universal popularity and demonstrated excellent surgical efficacy. However, many surgeons have concerns about stress urinary incontinence after HoLEP, since the prevalence of stress urinary incontinence after HoLEP (4.9%–12.5%) [8161718] was reported as higher than after open prostatectomy (3%–9%) [3435] or conventional TUR-P (approximately 2%) [9] for BPH. Although most of the postoperative stress urinary incontinence is transient in HoLEP, some surgeons have tried to seek better techniques for preserving the sphincter, especially at the apical prostate. Furthermore, if the depth of the three longitudinal incisions of the original three-lobe technique does not coincide with each other, especially when the prostate is large, a residual adenoma may remain due to the formation of multiple surgical planes. Concerns over these issues have led many HoLEP surgeons to become interested in the development of new techniques.
Go to :
ANTEROPOSTERIOR DISSECTION BY THE TOKYO GROUP
In 2008, Endo et al. [22] started to compare the clinical outcomes in 37 patients who underwent anteroposterior dissection with those of 31 patients who underwent conventional Gilling's method. Although the surgical method that he developed was the same in principle as that of Gilling et al. [30], they modified this technique to further reduce the possibility of sphincter damage. The enucleation method on the middle lobe remained the same, but the method of enucleating the lateral lobes was modified.
This new procedure is performed similarly to the previous procedure in that the bottom edge of the lateral lobe was enucleated from the surgical capsule throughout the apex and the bladder neck. However, this procedure did not extend further upward, and instead stopped just after forming the edge. A longitudinal incision was made over the 12 o'clock direction from the bladder neck to the sphincter level. In detail, the urethral mucosa at the 12 o'clock point opposite the verumontanum was first vaporized to reach the surgical capsule, which was extended to the bladder neck in a retrograde fashion. The adenoma was then released from the surgical capsule in either side around the 12 o'clock position while pressing downward at the mid-portion of each lateral lobe.
Since a natural surgical plane exists between the capsule and the adenoma, the bladder neck is first dissected along this continuous plane. Subsequently, the dissection proceeds anteroposteriorly and downward while moving to the distal apex. The apical urethral mucosa between the 12 and 5 o'clock position is torn off naturally from the left prostatic capsule without compromising the urethral sphincter. The prostate surface mucosa of the remaining apex is completely isolated from the adenoma, and the remaining mucosal connection between the adenoma and the prostatic capsule is resected in a retrograde manner. The authors reported that the operation time was similar in patients with an average prostate volume of 68.7 to 77.8 mL, but the transient stress urinary incontinence rate was significantly improved by 2.7% compared to 25.2% with the conventional method.
One of the unique characteristics of this procedure is that it adopted the antegrade incision approach as outlined in Gilling's procedure, which extends the 12 o'clock incision from the bladder neck to the apex. On the contrary, this procedure creates a retrograde longitudinal incision from the 12 o'clock position of the apical point to the bladder neck to prevent potential sphincter damage.
Go to :
MODIFICATION OF THE ORIGINAL THREE-LOBE TECHNIQUE BY THE XIAN GROUP
Gong et al. [23] developed a surgical technique to better delineate the surgical capsule. He made an initial posteriorapical incision and expanded it to the anterior prostate, while maintaining the surgical plane. Specifically, enucleation starts by dissecting the left apical area after a small incision is made at left lateral side of the verumontanum. The apical incision is extended circumferentially to the 3 o'clock position in the left lateral lobe, and to the 9 o'clock position in right lateral lobe through a transverse incision at the proximal part of the verumontanum.
Enucleation is performed in the direction of the bladder neck by separating the lower part of the median lobe from the prostatic capsule. The left lateral lobe is separated from the median lobe by making a vertical incision at the 5 o'clock position of the prostatic adenoma. The apical dissection of the left lateral lobe is further extended along the surgical capsule from the 3 o'clock position toward the 11 o'clock position. The left lateral lobe is then separated from the anterior prostatic tissue. Careful dissection of the urethral mucosal strip at the 1 o'clock and 12 o'clock position is carried out at the verumontanum level. The left lateral lobe is then separated from the right lateral lobe by making an incision at the 12 o'clock position in a retrograde fashion.
Enucleation of the right lateral lobe is accomplished in the same manner as the left lateral lobe. As the right apical incision is circumferentially performed from the 9 o'clock position to the 11 o'clock position, the urethral mucosal strip between the 11 o'clock and 12 o'clock position is formed. The right lateral lobe is easily separated from the surgical capsule when the mucosal strip is dissected.
Complete separation of the anterior prostatic tissue from the capsule while also preserving the sphincter at the 12 o'clock position is one of the most significant concerns in Ho-LEP surgery. In this procedure, when separating the anterior prostatic tissue from the capsule, the authors attempted to maintain the continuity of the surgical plane at the left lateral lobe by carrying the enucleated plane over to the opposite 11 o'clock position. After the mucosa of the left lateral lobe was separated from the sphincter, the authors made an incision at the 12 o'clock position in a retrograde fashion to avoid the damage to the sphincter. Although the authors did not mention the exact starting point of the longitudinal incision connecting the apex and the bladder neck at the 12 o'clock position, the location was naturally determined during the exposure of the surgical plane around the 12 o'clock position.
Go to :
EN BLOC NO-TOUCH EUCLEATION BY THE TURIN GROUP
Since 2010, several en bloc methods have emerged; these methods differ depending on whether the longitudinal incision is applied to the prostatic adenoma [2526272829]. Furthermore, there are differences in the methods of apical mucosal incision, as well as the handling of anterior prostate tissue at the apical 12 o'clock position. The reason for attempting to remove the prostatic adenoma with en bloc is as follows: First, as mentioned previously, there is a concern that residual tissue may remain due to a potential mismatch among the surgical planes due to the conventional three longitudinal incisions. Second, there is a need to overcome problems with improper incision length and depth when making longitudinal incisions at the 12 o'clock position from the bladder neck to the apex. If the incision is extended too distally, there is a risk of sphincter damage, if the incision is too deep, there is a risk of bleeding due to capsular perforation, and if the incision is too shallow, residual tissue will remain. Depending on the en bloc surgical method, there is a difference in the techniques of apical mucosal incision and enucleating the anterior prostate at the 12 o'clock position of the apex.
Scoffone and Cracco [25] applied the en bloc no-touch technique in 270 patients. At the beginning of the operation, a small incision is made at the left lateral side of the verumontanum and the surgical plane is widened in a retrograde manner. The left lateral lobe is longitudinally and retrogradely incised from the apex to the bladder neck at the 5 o'clock position. The left lateral lobe is enucleated sideways and moves up to the 3 o'clock position from the 5 o'clock position. At the 3 o'clock position, enucleation proceeds further to the 12 o'clock position, then overpasses the anterior commissure from the 12 o'clock position to the 9 o'clock position of the right lateral lobe. By using this technique, the correct surgical plane should always be maintained.
After the return to the 5 o'clock position of the apex, the apex of the right lateral lobe is approached by making a transverse incision at the proximal verumontanum. The median lobe and the right lateral lobe are enucleated from the 5 o'clock position to the 9 o'clock position as a single lump. Enucleation of the prostatic adenoma ultimately results in a horseshoe-shaped adenoma.
Further enucleation leaves a residual fan-shaped anterior mucosal strip between the 10 and 2 o'clock positions. Since this area is very close to the sphincter it should be approached very carefully; in other words, the prostatic adenoma and mucosa should be well separated at this site. Oblique incisions from the 10 o'clock position and the 2 o'clock position on either side are made so that the two incisions can be convergent to the 12 o'clock position. Finally, a transverse incision is applied to the mucosal strip at the 12 o'clock position in order to separate the mucosal attachment connecting the adenoma and the capsule. The authors emphasized that the incision should be kept at least 1 cm away from the sphincter. They also pointed out that in order to prevent sphincter damage a slight stretch of the adenoma toward the bladder neck should be maintained by the tip of the endoscope while incising the mucosal attachment. Furthermore, a completely separated adenoma is pushed into the bladder for morcellation.
In very large prostatic adenomas that significantly undermine the bladder trigone, it may be challenging to push the prostatic adenoma into the bladder by en bloc. However, various techniques for avoiding damage to the sphincter are noteworthy.
Go to :
EN BLOC ENUCLEATION WITH ANTEROPOSTERIOR DISSECTION BY THE CHIBA GROUP
Minagawa et al. [26] enucleated the prostatic adenoma en bloc using a similar method to the anteroposterior dissection technique performed by Endo et al. [22]. First, an incision is made on both sides of the verumontanum to lift both lateral lobes from the apex. The incision is made at the 12 o'clock position matched to the verumontanum level, exposing the prostatic capsule. A subsequent longitudinal incision along the 12 o'clock direction is made to separate the left and right lateral lobes. The enucleation extends to the proximal direction and anteroposteriorly and downward from the bladder neck; this is followed by enucleation of the adenoma toward the apex of the prostate at the 6 o'clock position.
As the adenoma is enucleated from the urethral sphincter at the upper area, the urethral mucosa of the apex is naturally pushed aside to form a belt-shaped mucosal strip at the 3 o'clock position (left lateral lobe) and the 9 o'clock position (right lateral lobe). The prostate adenoma proximal to the mucosal strip is dissected from the prostatic capsule. The enucleated planes descend symmetrically on both sides, and meet each other at the proximal part of the verumontanum. As a result, the prostatic adenoma is completely enucleated by en bloc and is ready for being pushed into the bladder.
The authors asserted that this en bloc procedure maintains a continuous surgical plane between the prostatic adenoma and the capsule, leaving no residual prostatic adenoma. It is also important to note that the authors made significant efforts to develop the technique to preserve the sphincter.
Go to :
COMPLETE EN BLOC TECHNIQUE WITH DIRECT BLADDER NECK INCISION BY THE HAMAMATSU GROUP
Ito et al. (Hamamatsu, Japan) [27] developed an excellent en bloc technique by retrospectively analyzing the results of serial patients with three consecutive changes in HoLEP technique. They divided the patients into three groups according to the following technique: the three-lobe technique, conventional en bloc technique, and the complete en bloc technique with direct bladder neck incision. They found a significantly shorter enucleation time and a significantly lower total laser energy with the new technique.
The mucosa lateral to verumontanum is incised to identify the correct plane for the capsule at the apex of the right lobe. The adenoma is separated from the surgical capsule in a retrograde manner toward the bladder neck. The bladder lumen is then reached by an incision at the 10 o'clock position, and enucleation is performed antegrade toward the posterior side of the right and median lobes. Continuous separation of the median lobe is performed by making a sharp incision at the bladder neck in order to mobilize the adenoma. The left lobe is enucleated in an anterograde manner, and the en bloc enucleation of the entire adenoma is completed. A mucosal band of the urethral sphincter is naturally formed at the apical urethra. The apical mucosal band is cut in order to push the completely enucleated adenoma into the bladder lumen.
The surgical video describing this procedure shows a long tear over the area distal to the sphincter. In addition, there is no description of surgical tips to determine the boundary of the mucosa. Therefore, beginners may face some difficulty in finding the edge to cut the mucosal strip at the distal apex. Nevertheless, this surgical technique has an advantage in that the surgical plane can be maintained throughout the procedure.
Go to :
EN BLOC ENUCLEATION WITH EARLY APICAL RELEASE BY THE MILAN GROUP
Saitta et al. [28] set the starting point of enucleation at an anterior apex. The mucosal incision starts from the 11 o'clock position to the 1 o'clock position of the prostatic apex, located proximal to the sphincter edge. This initial incision is further extended to the 10 o'clock position and the 2 o'clock position as the incision becomes deeper until the prostatic capsule and adenoma are entirely separated.
Subsequently, small vertical incisions are made lateral to the verumontanum at the 5 o'clock and 7 o'clock positions. However, a transverse incision connecting the two adjacent incision lines in the proximal verumontanum, which is common in other procedures, is not performed at this step. The incisions at each side are extended to the 7 o'clock position (right lateral lobe) and the 5 o'clock position (left lateral lobe). The incision lines at the 7 o'clock and 5 o'clock positions is connected to the previous initial incision lines at the 11 o'clock and 1 o'clock positions, respectively; this results in complete mucosal incisions in the apical area.
Subsequently, the right lateral lobe is enucleated circumferentially from the 7 o'clock position to the 11 o'clock position, the left lateral lobe from the 5 o'clock position to the 1 o'clock position. The planes of the two enucleations meet at the 12 o'clock position. When the apex near the 12 o'clock direction is released, a transverse incision is made at the 6 o'clock position proximal to the verumontanum in order to completely free the whole apex from the capsule. After the sphincter area is liberated, the adenoma is progressively enucleated circumferentially toward the proximal bladder neck. The mucosal attachment between the adenoma and the bladder neck is cut, and the prostatic adenoma is pushed into the bladder. The authors argued that this method of early release of the sphincter from the prostatic capsule is a crucial step in sphincter preservation because it prevents sphincter stretching.
Go to :
THREE HORSESHOE-LIKE INCISION EN BLOC HoLEP BY THE FREIBURG GROUP
Miernik and Schoeb [29] devised a ‘three horseshoe-like incision HoLEP,’ en bloc HoLEP method using three horseshoe-shaped incisions. They performed this procedure in 114 patients and compared the results with those who underwent conventional HoLEP. Although they did not provide long-term follow-up data, they reported that the total operation time was significantly shortened in patients who underwent the new procedure.
First, an inverted U-shaped incision is made around the verumontanum and the median lobe is lifted for enucleation. Apical prostatic adenomas of both sides are enucleated until the mucosal strip is formed in both lateral lobes. Subsequently, another inverted U incision is performed from the 10 o'clock position to the 2 o'clock position in order to release the mucosal strip; now, the adenoma of both lateral lobes is fully mobilized at the apex site. Next, the channel is formed between the anterior commissure and the capsule, as enucleation proceeds to reach the bladder neck. Here, the third inverted incision is made to the bladder neck in order to partially detach the adenoma from the bladder neck; both lateral lobes are now circumferentially enucleated. After the median lobe is enucleated to the bladder neck, the remaining mucosa attached to the prostatic adenoma is incised between the 4 and 8 o'clock position. Unlike other en bloc methods, this technique does not apply longitudinal incisions.
This surgical technique provided a simplified procedure for HoLEP, and is likely to be standardized for beginners for training purposes; however, this technique has a number of issues. For example, in cases of very large prostates where the median lobe deeply undermines the bladder trigone, the whole adenoma is unlikely to be pushed into the bladder with this procedure. Moreover, the sphincter area, which is the most distal part at the 12 o'clock position, needs to be identified. It may be difficult for beginners to follow the technique for these reasons. Stress urinary incontinence is a multifactorial phenomenon, and it is thought that many factors such as age, neurological disease, prostate shape [36], prostate size, accompanying bladder function, have a role in this condition. Therefore, the method of en bloc enucleation may not be the most suitable for use in this context.
Go to :
EARLY INVERTED V-SHAPED APICAL MUCOSAL INCISION WITH ANTERIOR CONJOINING (SEOUL NATIONAL UNIVERSITY HOSPITAL'S MODIFICATION)
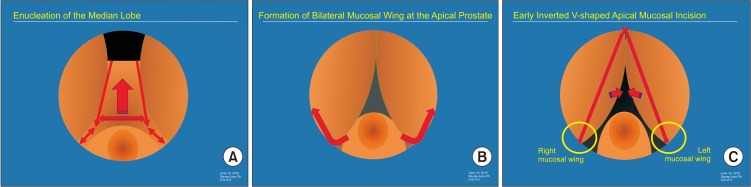
The detailed HoLEP surgical techniques used at Seoul National University Hospital were described in 2013 [6]. Although this technique is based on the three-lobe technique, it was modified to better preserve the sphincter around the prostate apex at the 12 o'clock position. The introduction of an early inverted V-shaped mucosal incision, and a technique for the dissection of the anterior prostate at the prostatic apex are the critical features of this modification (Fig. 1, Supplementary materials).
The location of the sphincter is confirmed with an endoscope prior to surgery in order to establish a whole surgical plan. Initially, a small longitudinal incision is made at both sides of the verumontanum in order to identify the prostatic capsule. The enucleation of the median lobe is initiated by a deep longitudinal incision in the 5 o'clock and 7 o'clock direction from the bladder neck to the previous incisions made around the verumontanum at each side. A subsequent transverse incision on the verumontanum to connect the two longitudinal incisions is made to further complete the enucleation of the medial lobe. After rotating the scope by 180 degrees, a small incision is made at the 12 o'clock position of the bladder neck (point 1), and the incision is widened downward on both sides. The first step for the enucleation of both lateral lobes is to leverage them upwards to uncover the prostatic surface of the apical region with a bottom-to-top motion, from the 7 o'clock to 9 o'clock position in the right side, and from the 5 o'clock to 3 o'clock position in the left side.
A mucosal web, once covering the lower edge of adenoma in each lateral lobe, become evident as the lateral lobe was lifted upwards. The authors have previously described the technique of the incision of this mucosal web as a ‘curtainopen incision’ [6]. It is very important to make this mucosal web in advance because it is very useful for later inverted V-shaped mucosal incisions. The most crucial point at this step before proceeding with the enucleation of the left lateral lobe is to incise the surface mucosa of both lateral lobes in advance; otherwise, the urethral mucosa is torn over the distal part of the urethral sphincter in a longitudinal direction as the enucleation proceeds upwards. The incision on the free mucosal web can be easily performed without direct contact with the sphincter. In this case, we have previously described that the apical mucosal incision should be directed on the prostatic adenoma side rather than the boundary of each lateral lobe [6]. Nowadays, an incision is performed at a more medial position in order to leave a greater urethral mucosal layer on the surface of the sphincter. To keep sufficient mucosal layer on the sphincter might be advantageous to prevent transient urinary incontinence immediately after surgery.
The starting point of the mucosal incision should be proximal to the sphincter at a midline 12 o'clock position (point 2). If the endoscope is slightly retracted, the outline of the sphincter is identified. The tip of the laser can be placed proximal to the sphincter; in this way, it is possible to safely make a further vertical connecting incision from point 1 and point 2 in the 12 o'clock direction. The exact location of the distal end of the 12 o'clock position for the longitudinal incision was not described in detail in our previous paper [6].
Previously, the authors described performing a conjoining mucosal incision at the 3 o'clock position (left lateral lobe) and the 9 o'clock position (right lateral lobe) [6]. However, now a slightly modified method is applied. Once the inverted V-shape mucosal incision is performed, the enucleation of the apex becomes easy. The left prostatic adenoma portion between the 12 o'clock and 2 o'clock positions should be approached from both sides (‘anterior conjoining’) in order to release the adenoma from the capsule without leaving any remnant adenomatous tissue, i.e., from the top to the bottom, and from the bottom to the top. The incision made on the mucosal strip should be a sufficient distance away from the sphincter. At the 1 o'clock or 2 o'clock position, the enucleation plane for the left lateral lobe is secured at the bladder neck, and further enucleation is performed laterally. The left lobe is then fully enucleated and pushed into the bladder.
To enucleate the right lateral lobe, the right prostatic adenoma is swept up circumferentially from the bottom upwards. Enucleation can proceed from the 7 o'clock position to the 10 o'clock position without difficulty, since the previous inverted V-shaped mucosal incision already separated the covering mucosal layer. At this point, a slight retraction of the endoscope reveals that the mucosal strip remains connected to the adenoma at the 11 o'clock position. A careful transverse incision on the proximal side of this mucosal strip aligns the incision with the mucosal margin of the opposite left side; then, the cross-over technique, to remove any remnant tissue in the left anterior lobe, can be accomplished. Bleeding arteries around the sphincter at the 10 o'clock, 12 o'clock position, and 2 o'clock position of the apex are frequently found, and care must be taken to maintain adequate hemostasis.
Go to :
CONCLUSIONS
Modifications of the original three-lobe technique have been developed to improve surgical outcomes, and several en bloc enucleation methods have also been introduced. However, compared to the original technique, more clinical evidence is needed to show the superiority of newer techniques over the original three-lobe technique in terms of efficacy and long-term side effects. So far, none of the newer techniques have been accepted as a standard technique for HoLEP. Standardization of a more simplified and effective HoLEP technique can significantly help beginners to overcome the learning curve more efficiently.
Go to :






 XML Download
XML Download