

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anastomotic leakage has always been an important complication in colorectal surgery. Especially for rectal cancer, surgery has a higher leakage rate and more complicated morbidity. Rectovaginal fistula (RVF) is a type of anastomotic leakage, but the incidence is low and few studies have been reported [1234]. Furthermore, although various procedures and treatments for RVF have been proposed, optimal strategies are still controversial [5678]. Redo coloanal anastomosis (RCA) is one procedure for RVF and is a valuable surgical option that avoids a permanent stoma in nearly 80% of patients with failed colorectal or coloanal anastomosis [910]. But, RCA not only is a difficult operation but also lacks the results of treatment on RVF.
Thus, our purpose was to find out the difference of leakage, according to RVF presence or absence, to know the risk factor of RVF, and to identify the optimal strategy of treatment for RVF by evaluating the success rate of each treatment.
METHODS
Patients
Between April 1997 and June 2013, 950 patients who underwent low anterior resection with colorectal anastomosis or coloanal anastomosis for rectal cancer were identified from the prospective database of the Colorectal Department at Kyungpook National University Medical School. All patients were female and retrospectively analyzed. We excluded patients diagnosed with inflammatory bowel disease or with familial adenomatous polyposis or who were diagnosed with or underwent abdominoperineal resection surgery. This study was approved by the Institutional Review Board of Kyungpook National University Medical Center. All patients gave their informed consent in writing prior to surgery during the study period (KNUCH-16-05).
Definition
The diagnosis of RVF was defined as the presence of clinical symptoms with communication between the vagina and the anastomotic area by clinical examinations (digital rectal palpation, endoscopy, or radiological investigations). We defined the onset of symptom as the date when the symptom was first confirmed in the out-patient department. When vaginal fecal discharge presented, we defined as the symptom in RVF, and anal pain with fever presented, we define as the symptom in nRVF.
We defined success as the absence of any vaginal discharge of feces, or mucous during at least 3 months after the last procedure with the absence of stoma. When 2 treatments were successfully used at the same time, we considered each treatment successful. The major procedure defined as a surgery case need to general anesthesia. We defined a major procedure as a surgery case that needed general anesthesia. Conservative treatment included applying drainage to the pelvic cavity, covering the anastomosis with fibrin glue, or installing a rectal tube.
Methods
We divided patients who underwent low anterior resection with leakage for rectal cancer into 2 groups. One group was the patients who had anastomosis leakage with RVF (RVF, n = 18). The other group was the patients who had anastomotic leakage without RVF (nRVF, n = 29). We compared the 2 groups according to the patients' demographics and perioperative outcomes. And to know the risk factor of RVF, we compare the RVF group with the no-leakage group. We performed 4 types of procedures to treat RVF, and analyzed the success rates of each procedure.
Surgical procedures
All enrolled patients received low anterior resection with curative resection for rectal cancer. The 4 types of procedures we performed for RVF were primary repair, diverting stoma, RCA, and a conservative procedure. In general, we considered primary repair as the first step of treatment for the RVF, unless we had other serious complications, and we considered primary repair again or creating stoma when the first step had failed. Despite this strategy, RCA was finally performed in cases of repeated failures.
Statistical analysis
The Pearson chi-square test was used for the univariate analysis of categorical variables and the Mann Whitney U-test was used for continuous variables. For comparing more than 2 groups, the Pearson chi-square test or the Kruskal-Wallis test was used, and summarized data were presented as median values with a range. The stepwise logistic regression model used for multivariate analysis with variables considered clinically significant. A P <0.05 was taken as being statistically significant. We performed statistical analysis using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA).
RESULTS
Comparison of clinical result
From 1997 to 2013, 950 consecutive women received lower anterior resection for rectal cancer in our institution. Of the enrolled study patients, 47 patients underwent anastomotic leakage. The incidence rate of anastomotic leakage was 4.9% and leakage with RVF was 1.9% which is lower than that of nRVF (3.0%) (Fig. 1).
In the total of study patients, anastomotic leakage occurred statistically significantly at a low primary tumor location and low anastomosis level (6.6 cm, P = 0.006; 3.6 cm, P = 0.005). Further in a multivariate analysis study of the risk factors for RVF, below 5 cm of anastomosis was significantly associated with RVF (P = 0.008) (Table 1).
However, when comparing the 2 groups, what showed a significant difference was not primary tumor location and low anastomosis, but perioperative radiotherapy and delayed onset time (27.8% vs. 3.4%, P < 0.015; 181.3 ± 176.4 days vs. 23.2 ± 53.6 days, P < 0.001). There were no influences with primary tumor depth and primary tumor direction for RVF. Five patients had advanced T4 tumor at leakage groups. Three of them underwent RVF and 2 underwent nRVF (16.7% vs. 6.9%, P = 0.291). The patients who had tumor direction for the vaginal aspect were 13 patients in the leakage groups. Among them, 7 patients underwent RVF and 6 underwent nRVF, which was not statistically significant (38.9% vs. 20.7%, P = 0.273). When we analyzed all patients according to the other factors, there were no significant differences with age, body mass index, American Society of Anesthesiologists physical status classification, CEA level, or previous history of hysterectomy (Table 2).
Comparison of treatment
Comparing the RVF group and nRVF group, the RVF group received more procedures than did the nRVF group. However, the success rate of the RVF group was lower than that of the nRVF group (83.3% vs. 100%, P = 0.025) (Table 2).
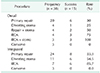
After a median follow-up of 38 months (range, 2–123 months), 45 procedures were performed in 18 patients with RVF and 42 procedures in 29 patients with nRVF. The most commonly performed procedure in the RVF group was primary repair, which showed a lower success rate than in the nRVF group (33.3% vs. 57.1%). Surprisingly, the results of the conservative procedure differed according to the pattern of leakage. The RVF group did not show success, but the nRVF group had a 75% success rate. Analyzing the results of these, the procedure of RCA had a satisfactory result in the RVF group and a higher success rate than the other procedures had (n = 6 [85.7%]) (Table 3).
In analysis of the duration taken from primary surgery to the treatment operation, there were no different durations according to the treatment procedure (P = 0.507). The mean time taken for all 18 patients was 252 days. Among them, 8 cases were primary repair (303 days), 4 cases were stoma (300 days), 3 cases were repair with stoma (51 days), 2 cases were RCA with stoma (308 days), and 1 case was RCA (140 days).
As the treatment detail of RVF in Table 4, 7 patients received only 1 procedure at treatment during the follow-up period. Among them, 2 patients treated with stoma and remained failed result, because they did not want any further treatment when RVF recurred 2 months later. On the other hand, there was 1 patient who received 5 procedures and who was able to obtain a successful result after the fifth procedure (RCA) despite repeated recurrences after the 4 repairs. There were 15 patients who had success; 7 of them received combination therapy. The most successful combination was RCA combined with stoma (Table 4).
DISCUSSION
RVF is thought to be an infrequent complication of low anterior resection (LAR) for rectal cancer. Despite numerous publications dealing with RVF, only a few studies have focused on RVF after LAR for rectal cancer [12311]. Only one study did a comparative analysis of RVF and nRVF in patients with rectal cancer, but there were no results of the treatment [4]. Therefore, we studied 47 patients who underwent postoperative anastomotic leakage and the differences and treatment outcomes according to RVF. During a median follow-up of 38 months, 18 of the patients had RVF, and a total of 35 procedures was performed, with a 42.8% (15 of 35) overall success rate. There were just 4 types of procedure for RVF. Each procedure analysis showed that the success rate ranged from 33.3% after primary repair to 85.7% after RCA. Because RCA had the highest success rate, it would be the last treatment for unresolved RVF patients.
The true incidence of RVF following LAR for rectal cancer is not well known. Previous studies have reported various ratios of RVF from 0.9% to 9.9% [1234]. However, this incidence can differ greatly depending on the definition of the RVF and the observation period. In this study, we defined RVF as a case with symptoms confirmed on postoperative follow-up abdominal CT. RVF was identified at 1.9% during the median follow-up observation period of 38 months, which is not different from the results of other studies.
The double stapling technique (DST) reconstruction after a previous hysterectomy was a classic cause of RVF after LAR [31213]. In this study, the RVF rate was 1.8% (15 of 831) in patients with DST and 2.5% (3 of 119) in patients with hand-sewn anastomosis. The incidence of RVF did not differ significantly between DST and hand-sewn anastomosis (P = 0.636). Of the total patients, 36 underwent perioperative hysterectomy or a combined hysterectomy (3.8%, 36 of 950). Only one of these 36 patients underwent RVF, and there was no significant difference from hysterectomy. (2.7%, 1 of 36; P = 0.686). Our data showed that DST and hysterectomy is not a risk factor for RVF.
Neoadjuvant radiotherapy has been suggested as a risk factor of leakage, and is accepted as such by many colorectal surgeons. It is also considered in RVF [4]. Nevertheless, our results showed that perioperative radiotherapy was associated with leakage but not with RVF. Five of the 133 patients who received radiation therapy developed RVF, which is similar to another 817 patients who did not receive radiation therapy (3.8% vs. 1.6%, P = 0.089). In comparison of leaked groups, the RVF group was statistically more related to perioperative radiotherapy than was nRVF (27.8% vs. 3.4%, P = 0.015). This result suggests that RVF is strongly associated with neoadjuvant radiotherapy in patients with leakage.
The overall success rate of RVF varies from 43% to 100% [131415]. Sonoda et al. [14] reported successful repairs in 43.2% of 37 patients who underwent the endorectal advancement flap to treat RVF of varying etiologies. Pinto et al. [15] reported a 56.3% success rate with similar procedures. But, Rahman et al. [16] reported a 100% success rate for 39 patients who underwent transvaginal purse-string repair. In this study, we performed 4 procedures and these showed an overall success rate of 83.3%. The success rate of primary repairs was 33.3% at median follow-up of 38 months. However, Corte et al. [17] reported a 91% success rate with delayed RCA. Similarly, our study showed an 85.7% success rate with RCA. And, our other study showed that RCA operation is feasible and do not make serious complications. Twelve patients who received redo surgery for postoperative RVF or rectourethral fistula had 1 severe complication to make re-creation stoma and there were no deaths [10]. This suggests that RCA is one of the successful options to treat RVF. Nevertheless, RCA should be indicated for patients who have relatively good condition suitable general anesthesia. Because, RCA is an operation with high difficulty and high morbidity rate (26%–41%) [9,18]. In our study, the patients who suffer from RVF were good condition suitable general anesthesia because, except in some cases, the timing of RVF development showed later onset than other leakage. It means RVF is more likely to be a stable condition than other leakage. Therefore, when treating RVF, the primary repair should be considered first, and RCA should be performed in patients who area in good condition to withstand major surgery. Because the success rate of primary repair was worthy to select for the first consideration of treatment of RVF.
Many surgeons prefer to propose a temporary stoma after several failed local surgical attempts or in association with a major abdominal procedure [17]. A temporary diverting stoma could prevent the danger of leaking as not letting stool go through. However, initially making a defunctional stoma in a low anterior resection to prevent leakage seems to be not very effective protection for developing fistula. Haksal et al. [19] reported that anastomosis fistula was one reason for failure of stoma closure (8.3%). Song et al. [20] reported that anastomosis leakage was an independent risk factor for stoma re-creation after closure of defunctioning stoma in patient rectal cancer. Also, fistula was involved in leakage. Our study showed that making defunctioning stoma was not significantly associated with the prevention of RVF (P = 0.207, Table 1). In this study, there were a total of 27 diverting stoma for treating RVF and nRVF; the success rate for RVF was lower than that for nRVF (6 of 11 [54,5%] vs. 14 of 16 [87.5%]), which suggests that diverting stoma is not very effective in treating RVF.
In one interesting study, Lamazza et el. [21] used a self-expanding metal stent for 10 patients with RVF. Among them, 7 patients had success and the other 3 patients had to receive surgery. However, our study did not consider this procedure, because a metal stent procedure has a high recurrence rate and possibility of residual incontinence after the fistula has healed [2223]. Moreover, the median tumor level of our study patients was too low to try stent insertion.
There are possible limitations associated with our study. First, it was retrospective, with a limited number of cases. However, RVF after rectal cancer surgery has a very low incidence. Moreover, it is difficult to collect cases at just one institution. Thus, further prospective multi-institutional studies of a larger population are needed to find optimal strategies for RVF. Second, this study did not follow the classic step-up approach for surgical management of RVF. However, we showed that simple strategies could successfully treat RVF. Moreover, simple strategies had higher success rates than did the step-up approach.
After LAR for rectal cancer, RVF developed more frequently in patients who had lower level of primary tumor location. Among the patients who underwent leakages, receipt of perioperative radiotherapy was significantly high in the RVF group than that of the nRVF group. This study suggests that the primary repair of RVF was worthy to select for first consideration to treatment and, RCA might be considered another successful treatment strategy for RVF.




 XML Download
XML Download