

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The incidence rate of thyroid cancer has been growing rapidly in Korea since the 1980s, with the highest incidence in 2010 according to the National Cancer Registration and Statistics [12]. The 5-year survival rate of thyroid cancer patients after thyroidectomy is 99.9%, which has led to increased interest in the quality of life of thyroid cancer survivors [23]. Patients diagnosed with thyroid cancer who undergo thyroidectomy often experience fatigue and persistent weight gain despite efforts to lose weight [4]. Although most evidence supports weight gain after thyroidectomy, weight loss has also been reported [56].
Obesity is considered by many surgeons as a challenge associated with perioperative complications that may worsen the outcome [7]. Overweight and obesity, indicated by high body mass index (BMI), are possible risk factors for thyroid cancer [7]. As per the National Health and Nutrition Examination Survey of the United States aggregated in 2009–2010, the predominance of heftiness was 35.5% and 35.8% among grown-up people individually, a noteworthy increment contrasted and 12% among men and 17% among ladies in 1976–1980. [678]. Whether or not the degree of obesity increases after thyroidectomy is unclear [7]. Given the controversy in the literature surrounding the impact of obesity on surgical outcomes, we aimed to investigate the relationship between thyroidectomy and obesity, and between the extent of thyroidectomy and obesity in thyroid cancer patients.
METHODS
The present study was approved by the Institutional Review Board (approval number: KUH1020065) of the Konkuk University Medical Center. Written informed consent was obtained from all participants. In June 2014, a total of 234 patients who had been diagnosed with thyroid cancer and had undergone surgery at the university medical center between June 2009 and December 2013 were surveyed for their postoperative obesity, fatigue, and physical activity. Their height, body weight, BMI), blood pressure, and basic blood test including thyroid-stimulating hormone (TSH) level before and after surgery were compared and analyzed. Four patients who had also been diagnosed with other cancers, such as colon cancer, breast cancer, or prostate cancer; 2 patients who had undergone total thyroidectomy (TT) after initial thyroid lobectomy due to relapse; and 1 subject who was lost during follow-up were excluded. A total of 227 patients were included in the analysis, of which 103 patients had undergone subtotal thyroidectomy and 124 had undergone TT.
We defined patients as obese (BMI ≥ 25.0 kg/m2), as proposed by the World Health Organization Western Pacific Region, the International Association for the Study of Obesity, and the International Obesity Task Force. Metabolic Equivalent of Task values (METs) were used to classify physical inactivity. METs are multiples of the resting metabolic rates and were calculated using the Korean version of the International Physical Activity Questionnaire, short form (version 1.0, Seoul, Korea). Physical inactivity was defined as less than 600 MET-min/wk. The data were analyzed using Student t-test, chi-square test, analysis of covariance, and logistic regression. Data are presented as means ± standard deviations.
RESULTS
Patients' characteristics
The mean age of all patients was 46.0 ± 11.0 years (range, 18–77 years). There were 188 women (82.8%) and 39 men (17.2%). The mean follow-up duration was 23.9 ± 16.7 months (range, 3.0–69.0 months). At the time of surgery, 38.8% of the patients were obese. Postthyroidectomy obesity was observed in 90 of the 227 patients (39.6%; Table 1).
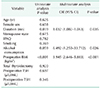
Comparison between lobectomy and TT
The TT group was older than the lobectomy group and had no difference between men and women. Menopause in women was more frequent in the TT group than in lobectomy group (P < 0.05). The prevalence of postthyroidectomy tended to be higher tendency in the TT group than in the lobectomy group (P = 0.062). The follow-up period of the TT group (28.3 ± 17.0 months) was longer than that of the lobectomy group (18.4 ± 14.6 months). The postoperative TSH level was 1.82 ± 1.86 µIU/mL in the lobectomy group and 0.35 ± 1.34 µIU/mL in the TT group, and the weight increase after surgery was 0.45 ± 0.38 kg and 0.17 ± 0.36 kg, respectively, with no significant difference between the 2 groups (P = 0.608). The BMI increased by 0.09 ± 0.41 kg/m2 in the lobectomy group and by 0.04 ± 0.14 kg/m2 in the TT group, with no significant difference between the groups (P = 0.417) (Table 1).
Predictors of postthyroidectomy obesity
In the univariate analysis, the predictors of postthyroidectomy obesity were older age (P = 0.001), female sex (P = 0.001), alcohol drinking (P = 0.029), and higher preoperative BMI (P < 0.001) (Table 2).
In the multivariate analysis, preoperative BMI (P < 0.001), heavy alcohol consumption (P = 0.026), and follow-up duration (P < 0.035) were independent predictors of postthyroidectomy obesity (Table 2).
DISCUSSION
The increasing rate of obesity in Korea, as well as in Western countries, is a growing public health problem [8]. According to the data from the 2015 Korea National Health and Nutrition Examination Survey for Korean adults aged 19 years or older, the prevalence of obesity (BMI ≥ 25 kg/m2) is about 40% for men and 26% for women, i.e., one-third of Korean adults are obese [89]. In this retrospective cohort study, we evaluated the relationship between thyroidectomy and obesity. Patients who undergo thyroidectomy are frequently concerned about weight gain after the initial treatment, but there are few data about weight changes in thyroid cancer patients undergoing thyroidectomy and the results are controversial [9]. In our present study, 38.8% (88 of 227) patients were obese at the time of surgery and 39.6% (90 of 227) showed postthyroidectomy obesity during follow-up.
Previous research reported inconsistent associations between different degrees of obesity as a postoperative outcome [9]. Our study focused on the relationship between thyroidectomy in thyroid cancer patients and obesity, and considered the extent of thyroid resection as a contributing factor to postoperative obesity. Several studies have investigated whether or not thyroid cancer patients gain weight after thyroidectomy. Kitahara et al. [1] compared 120 thyroid cancer patients who showed normal thyroid functions after TT with 120 patients who showed normal thyroid functions after treatment for hypothyroidism. Jonklaas and Nsouli-Maktabi [5] found that the TT group showed a much higher weight gain for a year. Thyroid cancer survivors who had developed iatrogenic hyperthyroidism after TT did not lose weight because of hyperthyroidism and had aging-related increases in body mass [10]. However, another study that compared 102 thyroid cancer patients who had normal thyroid function after TT with 92 thyroid nodule patients who had normal thyroid function reported no significant difference in the weight change and BMI between the 2 groups [46].
Obesity is generally believed to be a risk factor for the development of postoperative complications [6]. Although being obese is believed to be associated with medical hazards, recent literature shows no convincing data to support this assumption [11]. In our study, patients who were already overweight or had high BMI at the time of surgery had a higher risk of obesity after thyroidectomy. The preoperative BMI was significantly associated with postoperative BMI (Pearson correlation, r = 0.923, P < 0.001), and 39.6% of the participants showed postoperative obesity (odds ratio, 3.945; P < 0.001).
Previous exposures of the neck area to radiation, excessive iodine intake, chronic autoimmune thyroiditis, and obesity are some of the known risk factors of the increased incidence of thyroid cancer [1712]. It is well-known that higher BMI leads to higher the risks for various cancers, such as colon cancer, pancreatic cancer, and breast cancer, or endometrial cancer in menopausal women [1314]. There are reports that adipocyte proliferation and the action of adipocytokines in obese people cause insulin resistance and inflammation, which interacts with thyroid with and affects the occurrence of thyroid cancer [1516].
Patients with differentiated thyroid epithelial cancer experienced significant weight gain compared to their baseline weight after TT with ongoing TSH suppression [17]. Obesity is not only related to thyroid cancers, but is also closely related to the actual function of the thyroid. It is widely known that hyperthyroidism may cause weight loss and that hypothyroidism may cause weight gain; accordingly, hyperthyroidism treatment may lead to weight gain and hypothyroidism treatment to weight loss [18]. Many population studies have reported a positive correlation between blood TSH levels and the BMI of obese people [1718]. In our study, the mean TSH level was 1.92 ± 1.20 µIU/mL (range, 0.01–10.48 µIU/mL). At the time of the survey, the mean weight was 62.6 ± 12.1 kg (range, 41.9–115.1 kg); the mean BMI was 24.1 ± 3.6 kg/m2 (range, 16.0–37.4 kg/m2); the mean TSH level was 1.02 ± 1.76 µIU/mL (range, 0.01–10.48 µIU/mL). We provided thyroid hormone replacement therapy with levothyroxine after thyroidectomy and suppressed the TSH level according to the American Thyroid Association Guideline Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer 2009, which explains why the TSH level was higher in the thyroid lobectomy group than in the TT group. Although the weight gain was higher in the thyroid lobectomy group than in the TT group, the differences in weight change and BMI change between the 2 groups were not statistically significant (P = 0.284 and P = 0.417, respectively) even when iatrogenic hyperthyroidism with thyroid hormone replacement therapy after TT was compared with thyroid lobectomy.
A few studies on the impact of thyroid function on lipid metabolism are available. Bel Lassen et al. [19] proposed that endogenous subclinical hyperthyroidism after thyroidectomy may directly affect lipid profiles after thyroidectomy. Jung et al. [20] suggested that changes in thyroid function after thyroidectomy can be associated with changes in the concentration and functions of lipid profiles.
Recreational alcohol intake is common across the globe and health and social problems resulting from alcohol consumption are becoming a concern [2122]. The relationship between alcohol intake and body weight has been extensively studied over the past years [2122]. Our results show the risk of obesity after surgery in the alcohol consumption group was 6.492 times that of the group that did not consume alcohol.
Patients who underwent TT surgery tended to be older and had a longer follow-up period than patients who underwent lobectomy (P < 0.001). We perform thyroid lobectomy when patients have a low risk of papillary thyroid cancer according to the American Thyroid Association guidelines. Recently, thyroid lobectomy has been performed more frequently than in the past because surgeons and patients tend to prefer it to TT if there are no oncological problems [23]. This resulted in a difference of about 1 year in the follow-up duration between 2 groups. Although we adjusted for the time factor, it could be a limitation of our study. The small sample size was another limiting factor in this study, and larger-scale studies and randomized prospective studies would be needed in the future. Limitations of the study also include the retrospective nature of the data, so our study should be viewed as descriptive and hypothesis generating and not establishing causality. Another limitation was our inability to ascertain the difference in weight measurement error between various scales, because weights were measured during routine clinical care by multiple providers.
In conclusion, the extent of thyroidectomy does not significantly affect postthyroidectomy obesity. Preoperative obesity and heavy alcohol consumption are risk factors for postthyroidectomy obesity. Future well-designed larger studies and life style management for obesity control are needed.

 XML Download
XML Download