

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Osteoporosis is regarded as one of the most common diseased entity in modern society. The disease affects more than 33% of female over 50 years old and may result in osteoporotic fractures that may significantly downgrade life quality. And the impact of osteoporosis is most pronounced in elderly women who have the highest risk of fracture [123].
The diagnosis is often made by measuring bone mineral density (BMD) using dual energy x-ray absorptiometry (DXA) with the T score less than −2.5 utilized as a cut-off point for diagnosis of osteoporosis [4567]. Number of treatment modalities have been suggested to prevent and to treat osteoporosis. Currently, the most commonly used treatment is using various anti-resorptive (osteoclast) medications including bisphosphonate, selective estrogen receptor modulators (SERMs), and denosumab. While there are number of advantages and disadvantages of each anti-resorptive medication, SERMs is the most commonly used initiative medication for postmenopausal osteoporosis.
Recently, nutritional supplements have been suggested to be an important adjuvant therapy to maintain bone metabolism. This includes calcium and vitamin D which plays a significant role in bone remodeling [8]. However, while there are number reports on the role of vitamin D on BMD, there are only handful of reports when this is prescribed in combination with SERMs specifically.
Thus in this study, we aim to evaluate the effect of using supplementary vitamin D to the female osteoporosis patients who are treated with SERMs.
Go to : 
MATERIALS AND METHODS
Cohort selection
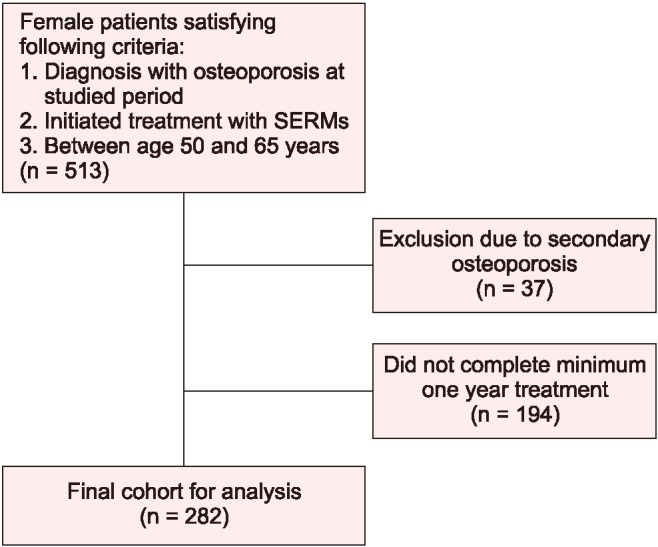
Retrospective chart review was performed on patients who were diagnosed with osteoporosis and initiated osteoporosis medications between January 2015 and December 2016. The inclusion criteria of the study are the patient 1) between the age of 50 and 65 years, 2) of the female gender, 3) had undergone menopause, 4) used SERMs as their primary osteoporosis medication, and 5) this who have taken the medication continuously for a minimum of 1 year. The exclusion criteria were the patients who had underlying diseases or medication that may potentially develop secondary osteoporosis.
Due to the recent high awareness of the importance of vitamin D supplements on osteoporosis, the prescription of vitamin D was routinely done by the senior author starting from January 2016. Therefore, the patients who were prescribed with SERMs between January 2015 and December 2015 did not receive vitamin D while the all of the patients who were prescribed after January 2016 received vitamin D supplements. Two-hundred eighty-two patients fulfilled our inclusion and exclusion criteria and this cohort constitute the bases of our study. Of these patients, 151 were treated with SERMs only while 131 were treated with SERMs and vitamin D supplements (Fig. 1).
Study protocol
In order to compare the epidemiologic characteristics of the two groups, the following factors were recorded; age, height, weight and the time since the menopause occurred.
In all patients, BMD was measured using DXA scan and this was done prior to the medication and was repeated at 1 year following the index prescription. The measurements at the total spine and total hip were recorded for comparison. Our initial protocol was to exclude the part of the spine that involves compression fracture. However, none of the patients had compression fracture when initial BMD was taken. Of the patients who developed spinal compression fracture during the follow-up, the affected vertebra was excluded when BMD was measured. The patients were also checked with the occurrence of osteoporotic fractures of any site including, around the hip, wrist, and ankle.
For the prescription of SERMs, raloxifene (Evista®;
Eli Lilly, Indianapolis, IN, USA) was prescribed in all patients. The prescribed SERMs is a daily medication which is taken orally. The patients were asked to take the medication following breakfast each day. For vitamin D supplements, daily oral pill of 1,000 IU (D-MAC®; Dalim BioTech, Seoul, Korea) was used. This was again, asked to take at the time of the SERMs administration. In addition to the prescription of the SERMs and vitamin D supplements, all patients had a prescription of daily calcium. Three-month prescription was given to the patient and was re-prescribed at each 3-month visit to the outpatient office. The patients were asked of any complication that may be related to SERMs, vitamin D and calcium and supplementary medication was given when necessary. The patients who had discontinued taking the medication were considered as the patient who did not take medication for minimal of 1 year and thus excluded from the study.
Statistical analysis
Statistical analysis was performed using SPSS ver. 18 software (IBM Corp., Armonk, NY, USA) and acquired data are expressed as mean ± standard deviation. For the simple comparison of the two groups, Student t test was used. For the comparison of the change in BMD between the two groups, paired t test was utilized. The P value less than 0.05 was considered to be statistically significant.
Go to :
RESULTS
The mean age of the patients was 58.9 ± 4.1 years with mean body mass index of 23.1 ± 4.1 kg/cm2. The time from the menopause was mean of 6.3 ± 4.0 years. The epidemiologic data of each group are described in Table 1.
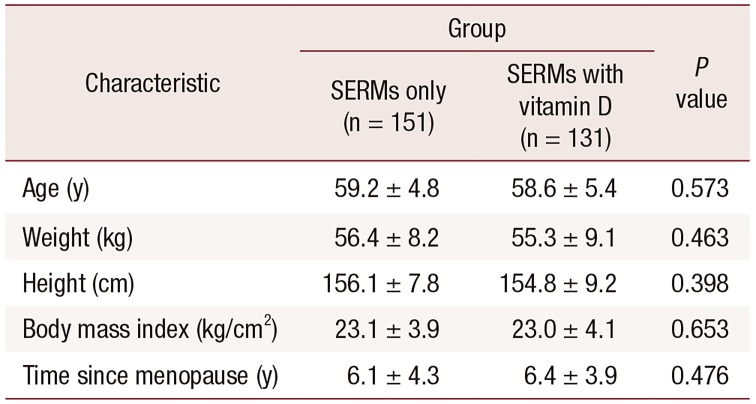
Table 1
Epidemiologic characteristics of patient cohort
![]()
Initially, the mean BMD of the patient cohort as measured by g/cm2 was 0.812 ± 0.231 in spine and 0.641 ± 0.154 in hip. There was no significant difference of the initial BMD when SERMs only group was compared with SERMs with vitamin D group (P = 0.387 in spine, P = 0.739 in hip). The patient of 68.2% had improved BMD at one year follow up (66.8% in SERMs group and 71.2% in SERMs with vitamin D group). The BMD of the SERMs only group improved by 3% in spine and 1% in hip while that of the SERMs with vitamin D group improved by 6% and 1%, respectively. When two groups were compared, significance improvement in spine (P = 0.045) was noticed with additional vitamin D yet no significance or trend was found in hip (P = 0.157). The BMD of the two groups are described in Table 2.
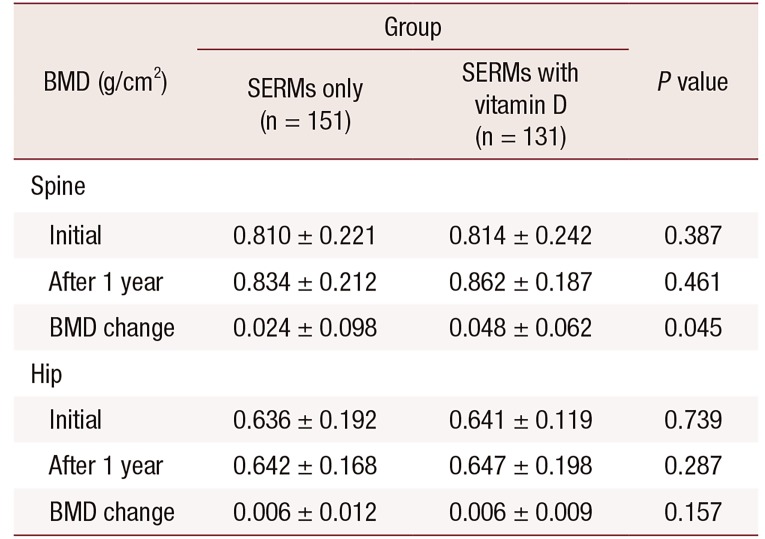
Table 2
Bone mineral density (BMD) of patient cohort
![]()
Regarding osteoporotic fracture, three patients developed distal radius fracture (1 in SERMs only group and 2 in SERMs with vitamin D group) as a resultant of slip down. One patient in the SERMs group developed single level vertebral fracture at the 4th lumbar spine. The summary of the occurred fractures and their treatments are summarized in Table 3. There was no significant difference on osteoporotic fracture occurrence between two groups (P = 0.8931).

Table 3
Summary of osteoporotic fractures occurred during the follow up
![]()
Go to :
DISCUSSION
The result of the current study shows that there is a potential tendency that vitamin D may further improve BMD in the spine if it is used in combination with SERMs. However, we were unable to notice any alteration in osteoporotic fracture risk with the use of vitamin D.
Vitamin D is produced in the skin, which has main role in bone and mineral metabolism [9]. Nowadays, vitamin D deficiency is correlated with cardiovascular disease by vitamin D receptor signaling [10]. Vitamin D is important for the treatment of osteoporosis as deficient vitamin D may result in defective bone mineralization which may eventually lead to low BMD [1112]. The primary function of vitamin D is regulation of calcium absorption in the intestine and stimulating bone resorption to maintain serum calcium concentration. Therefore, theoretically sufficient vitamin D may maximize the effect of the anti-resorptive therapy and consequently lower the fracture risk [1314]. The vitamin D can be derived from diet, sunlight and through other supplements. However, a recent study utilizing Korea National Health and Nutrition Examination Surveys (KHANES) reported that 76.7% of the overall Korean female population is vitamin D deficient which was defined as serum 25(OH)D level below 50 nmol/L [15].
Numbers of studies have tried to validate the effect of vitamin D on BMD. A study from Tuppurainen et al. [16] reported a significant increase in BMD of the femoral neck after 5 years. A study by Dawson-Hughes et al. [1718] also showed consistent result reporting a significant increase of BMD in non-vitamin D deficient patients. Similarly, a study by Islam et al. [19] reported significant improvement of BMD in total hip and femoral neck with Bangladeshi women with baseline 25(OH)D of 36 nmol/L [19]. In contrary, there are also numerous reports that vitamin D does not have any positive effect on the BMD. A meta-analysis on this subject was recently published by Reid et al. [20]. The authors investigated 23 randomized controlled studies which included 4,082 patients with a mean age of 59 years. The study revealed conflicting results; 6 studies reporting significant benefit, 2 reporting significant detriment and 11 reporting no significance. This meta-analysis concluded that the benefit of using vitamin D to improve BMD is questionable.
Raloxifene at the standard dosage of 60 mg daily prevents postmenopausal bone loss in women without osteoporosis and is used also to treat established postmenopausal osteoporosis [212223]. The effect of combining SERMs with vitamin D is a subject of debate. To our knowledge, there is no clinical study that looked specifically on this topic and only one animal study was done with male mice. The study from Sato et al. [24] treated osteoporotic male mice with SERMs and vitamin D analogue and found this therapy could block bone loss. Regarding the effect of raloxifene alone, there is handful of studies reporting its influence in osteoporosis [2526272829]. The studies consistently reported that use of raloxifene can increase BMD both of the spine and of the hip but the improvement in the spine is more prominent. This is somewhat similar to our study as our study also showed an increase of BMD both in the spine and in the hip but the amount increased was greater in the spine. Also, the studies consistently reported that raloxifene can prevent fracture of the spine but not the hip. In our study, we found only 1 spine fracture in the SERMs group and no occurrence of around the hip fracture. We think this discordance may be due to the relatively younger age of our patient cohort and also relatively short follow up period.
We acknowledge that there are number of limitations to the current study. Firstly, the number of patient cohort in our study is relatively small. As there are limited reports on the effect of vitamin D in combination with SERMs, we were unable to perform the sample size estimation prior to the study. Therefore, we think with the increase of patient cohort number, the effect of vitamin D on BMD will become more clearly visualized. Secondly, our follow up period may be too short. In the current study, we are reporting clinical result of one year follow up and this may be too short as the effect of such mediation can be effective for prolonged period. However, as the effect of SERMs is most powerful in the first two year after the administration, this study may at least provide baseline information on the effect of vitamin D on BMD. Also, as the compliance of osteoporosis medication is reported to be discouraging, adding additional year in follow up period may require substantial working force. Lastly, important data missing in the current study is patients' vitamin D level when the osteoporosis medication was first initiated. It is likely that the patient who had vitamin deficiency may benefit further from using supplementary vitamin D. Unfortunately, we were unable to verify this and this remains as an important limitation of the current study.
Nevertheless, to our knowledge, this is the first study that looked at the effect of vitamin D when used in combination with SERMs on BMD. According to our study, postmenopausal osteoporosis patient may further increase BMD of the spine if vitamin D is used in combination with SERMs. However, we also propose further study with a larger study population and extended study period to strengthen our result.
Go to :
 XML Download
XML Download