

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Osteoporosis is a skeletal disorder characterized by a decrease in bone mineral density. With the growing elderly population, morbidity and mortality rates associated with osteoporotic fractures are also increasing [1]. According to a study that analyzed the results of 2008 to 2011 Korea National Health and Nutrition Examination Survey (KNHANES) [2], the prevalence of osteoporosis among Korean women aged 50 years or older was high: 30.1% in the lumbar spine and 23.1% in the femoral neck. Therefore, early detection is important for reducing the fracture-related mortality rate among people with a risk of osteoporosis.
Bone mass is determined by the peak bone mass and extent of subsequent bone loss. Peak bone mass is not only affected by genetic factors, but also by nutritional status, physical activities, and hormonal changes [3]. Childbirth and breast feeding usually take place around the age of 30 to 39 years when the peak bone mass is achieved; thus, investigating the effects of parity and duration of breast feeding on the risk of osteoporosis among postmenopausal women is very important for the prevention of osteoporosis [4].
Childbirth and breast feeding affect calcium metabolism in women, which in turn, affects bone density [5]. While some studies have reported reduction in femoral bone density due to childbirth [367], other studies reported that parity may have a protective effect on the bones in multiparous women [89]. In addition, some authors claim that the number of childbirths does not have a significant effect on bone density in postmenopausal women since bone loss due to childbirth is recovered after delivery [101112]. Although some studies have reported that estrogen levels in mothers decrease during the breast feeding period and that the reduction is caused by calcium loss through breast milk [131415], other studies indicate that the duration of breast feeding and postmenopausal bone density are unrelated since bone loss stops once breast feeding is stopped and bones are restored to their original state [31617].
As shown, reduction in bone mass may be caused by calcium loss and hormonal change during pregnancy and breast feeding, but a consensus has not been reached on the long-term effects of such changes on the bone density of postmenopausal women. The reason for such conflicting findings between studies may be attributed to differences in ethnicity, age, menopausal status, parity, and/or duration of breast feeding of women in these studies, and the study designs. In particular, the average number of childbirths or duration of breast feeding among women in Korea differs from that in other Asian or Western countries. Therefore, results from studies outside Korea may not be directly applicable.
A recently published meta-analysis [18] showed that an increase in parity reduced the risk of hip fracture among postmenopausal women. However, another meta-analysis on the effects of parity on the bone density of pre-menopausal and post-menopausal women [19] reported that parity did not affect bone density in the lumbar spine and femoral neck, although primiparous or multiparous women showed significantly higher total femoral bone density than nulliparous women, indicating that the effect of parity on bone density may differ depending on the site of measurement.
Thus, even meta-analyses have failed to reach a consensus on the relationship between parity or duration of breast feeding and bone density. Particularly, since such correlations may appear differently depending on the ethnicity and menopausal status of the subjects and the site of bone density measurement, the present study included studies that investigated the relationship between parity or duration of breast feeding and bone density in the lumbar spine or femoral neck in postmenopausal Korean women alone. A meta-analysis was also performed to derive integrative results regarding these studies.
Go to : 
MATERIALS AND METHODS
Search strategy and study selection
The following terms were used to search Korean databases (RISS, KISS, KMbase, and KoreaMed) and non- Korean databases (PubMed, EMBASE, the Cochrane Library, and CINAHL) up to December 26, 2018. The search terms were “parity”, “bone mineral density”, “BMD”, “osteoporosis”, “bone mass”, “birth”, “labor”, “delivery”, “pregnancy”, “breast feeding”, “feeding”, and “lactation”.
Study quality assessment
The quality of individual studies was assessed using the modified form of the New Castle-Ottawa quality assessment scale (NOS) [20]. This scale consists of three major categories: selection, comparability, and outcome. Using this assessment tool, items with high quality of evidence were marked with an asterisk (*) and scores were assigned according to the total number of asterisks. The maximum possible score for each study was 8 points.
Inclusion and exclusion criteria
Studies that compared the relationship between parity or duration of breast feeding and bone density among postmenopausal Korean women were considered to have satisfied the inclusion criteria but only studies that measured bone density in the lumbar spine or femoral neck using dual energy X-ray absorptiometry were included. Only articles published in English or Korean were included. Among studies that used the same data, articles that presented statistics appropriate for meta-analysis were selected first, after which, articles with the largest sample sizes were selected. Moreover, studies that did not apply the World Health Organization (WHO) criteria for osteoporosis (T-score < −2.5 standard deviation [SD]) were excluded.
Data extraction
Three researchers independently assessed the suitability of the selected studies and extracted the data. The extracted data included the name(s) of the author(s), sample size, age of subjects, outcomes (parity and duration of breast feeding: mean, SD, odds ratio, and 95% confidence interval [CI]), and quality of study scores.
Statistical methods
Data analysis was performed using Comprehensive Meta-Analysis (CMA) version 2.2 (Biostat, Englewood, NJ, USA). The outcome variable in the present study was osteoporosis status. Meta-analysis was performed with fixed and random effects, where analysis was performed with random effects in cases with high heterogeneity. Heterogeneity was assessed using Higgins I2 and χ2, where, if I2 was ≥ 50% and χ2 was < 0.10, the case was determined to show heterogeneity.
Publication bias was assessed using a funnel plot and Egger's test, while sub-analyses were performed according to the characteristics of the subjects and studies (quality of study).
Go to :
RESULTS
Search for studies
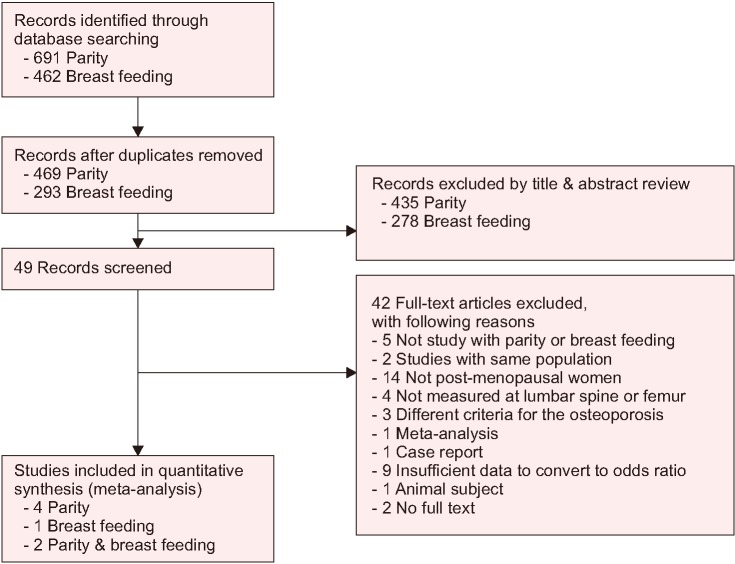
Based on the literature search, a total of 1,153 studies (691 studies on parity and 462 studies on breast feeding) were found. After excluding duplicate studies, 762 articles were extracted. An additional 713 articles (435 on parity and 278 on breast feeding) were excluded based on a review of the title and abstract, after which, the full text of 49 articles were reviewed. Ultimately, a total of 7 articles (4 on parity, 1 on breast feeding, and 2 on both parity and breast feeding) [21222324252627] were considered suitable for the present study, and a meta-analysis was performed on the studies (Fig. 1).
Study characteristics
The characteristics of the 7 studies included in the final analysis are shown in Tables 1 and 2. The total sample size was 3,813 patients, including 1,052 patients in the osteoporosis group and 2,761 patients in the non-osteoporosis group (including osteopenia and healthy patients). The mean ages of the osteoporosis and non-osteoporosis groups were 62.49 and 61.98 years, respectively. In 6 out of the 7 articles, the relationship between parity and risk of osteoporosis was analyzed: 3 studies [212223] presented parity as ranges of values while 3 studies [242526] used mean parity values. Moreover, 3 studies analyzed the relationship between duration of breast feeding and risk of osteoporosis: 2 studies [2127] presented duration as ranges of values and 1 study [24] used mean values.
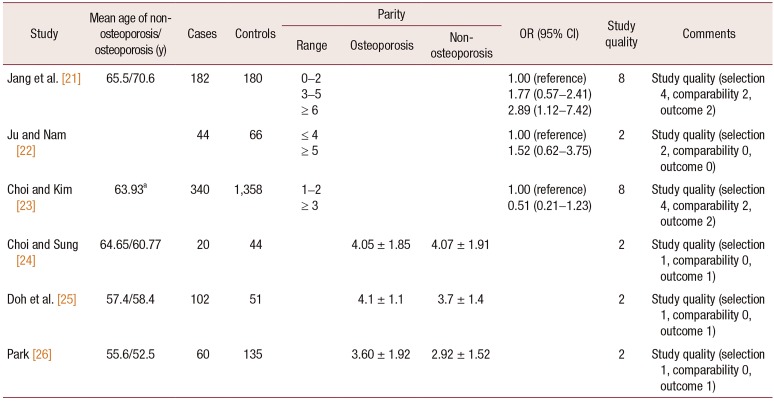
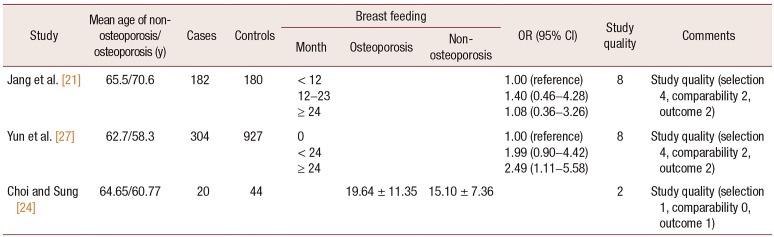
Table 1
Characteristics of included studies: parity and osteoporosis risk
| Study | Mean age of nonosteoporosis/osteoporosis (y) | Cases | Controls | Parity | OR (95% CI) | Study quality | Comments | ||
|---|---|---|---|---|---|---|---|---|---|
| Range | Osteoporosis | Nonosteoporosis | |||||||
| Jang et al. [21] | 65.5/70.6 | 182 | 180 | 0–2 | 1.00 (reference) | 8 | Study quality (selection 4, comparability 2, outcome 2) | ||
| 3–5 | 1.77 (0.57–2.41) | ||||||||
| ≥ 6 | 2.89 (1.12–7.42) | ||||||||
| Ju and Nam [22] | 44 | 66 | ≤ 4 | 1.00 (reference) | 2 | Study quality (selection 2, comparability 0, outcome 0) | |||
| ≥ 5 | 1.52 (0.62–3.75) | ||||||||
| Choi and Kim [23] | 63.93a | 340 | 1,358 | 1–2 | 1.00 (reference) | 8 | Study quality (selection 4, comparability 2, outcome 2) | ||
| ≥ 3 | 0.51 (0.21–1.23) | ||||||||
| Choi and Sung [24] | 64.65/60.77 | 20 | 44 | 4.05 ± 1.85 | 4.07 ± 1.91 | 2 | Study quality (selection 1, comparability 0, outcome 1) | ||
| Doh et al. [25] | 57.4/58.4 | 102 | 51 | 4.1 ± 1.1 | 3.7 ± 1.4 | 2 | Study quality (selection 1, comparability 0, outcome 1) | ||
| Park [26] | 55.6/52.5 | 60 | 135 | 3.60 ± 1.92 | 2.92 ± 1.52 | 2 | Study quality (selection 1, comparability 0, outcome 1) | ||
![]()
Table 2
Characteristics of included studies: breast feeding duration and osteoporosis risk
| Study | Mean age of nonosteoporosis/osteoporosis (y) | Cases | Controls | Breast feeding | OR (95% CI) | Study quality | Comments | ||
|---|---|---|---|---|---|---|---|---|---|
| Month | Osteoporosis | Nonosteoporosis | |||||||
| Jang et al. [21] | 65.5/70.6 | 182 | 180 | < 12 | 1.00 (reference) | 8 | Study quality (selection 4, comparability 2, outcome 2) | ||
| 12–23 | 1.40 (0.46–4.28) | ||||||||
| ≥ 24 | 1.08 (0.36–3.26) | ||||||||
| Yun et al. [27] | 62.7/58.3 | 304 | 927 | 0 | 1.00 (reference) | 8 | Study quality (selection 4, comparability 2, outcome 2) | ||
| < 24 | 1.99 (0.90–4.42) | ||||||||
| ≥ 24 | 2.49 (1.11–5.58) | ||||||||
| Choi and Sung [24] | 64.65/60.77 | 20 | 44 | 19.64 ± 11.35 | 15.10 ± 7.36 | 2 | Study quality (selection 1, comparability 0, outcome 1) | ||
![]()
The quality scores of the included studies ranged between 2 and 8 points. Among the studies on parity, 4 out of 6 studies showed a low quality with a score of 2 points, whereas, the other 2 studies showed a very high score of 8 points. Among the studies on duration of breast feeding, 2 out of 3 studies showed a very high score of 8 points, whereas, the remaining 1 study showed a low score of 2 points.
Estimation of the effect size of parity on the risk of osteoporosis
Among the 7 studies included in the meta-analysis, 6 studies analyzed the risk of osteoporosis according to parity, of which, 3 studies presented parity as mean values and the remaining 3 studies presented parity as ranges of values. The range of values varied between studies, including ranges of 0–2, 3–5, ≥ 6, ≤ 4, ≥ 5, 1–2, and ≥ 3. In 6 studies that analyzed the effect of parity on osteoporosis in postmenopausal Korean women, the effect size was derived by a fixed-effect model since heterogeneity was not high [χ2 = 8.193, degree of freedom (df) = 5, P = 0.146; I2 = 38.97%]. In these studies, the effect size of parity on the risk of osteoporosis was 1.43 (95% CI = 1.09–1.88), which was statistically significant (Z = 2.583, P = 0.010) (Fig. 2). The funnel plot did not show any publication bias, which was supported by Egger test results.
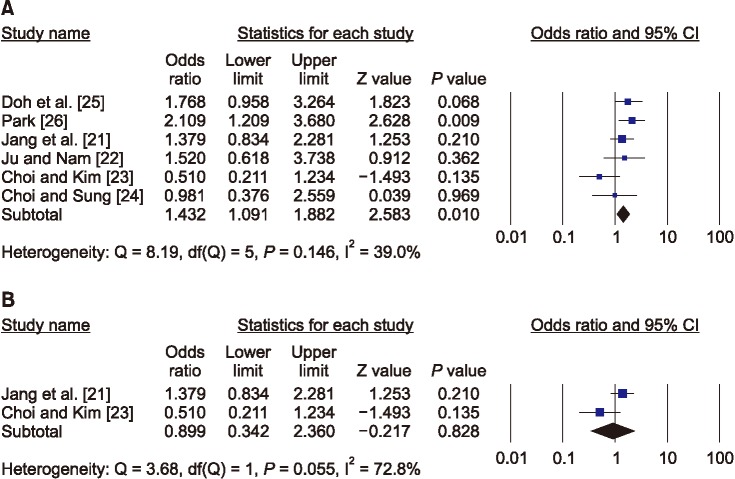
However, as shown in Figure 2, the weight value of one of the six studies that examined the effects of parity on the risk of osteoporosis was significantly higher than that of the other studies. Therefore, as a result of the sensitivity test for two high quality studies, the effect of parity on the risk of osteoporosis was not significant.
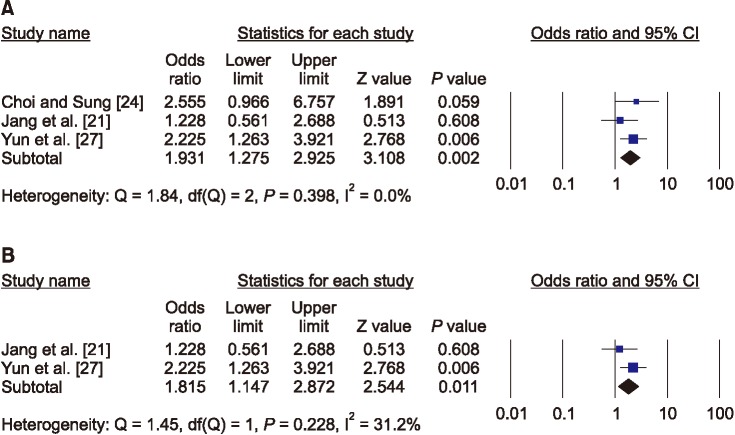
Estimation of the effect size of breast feeding duration on the risk of osteoporosis
Among the 7 studies included in the meta-analysis, 3 studies analyzed the risk of osteoporosis according to duration of breast feeding, of which, 1 study presented the duration of breast feeding as mean values and the other 2 studies presented it as ranges of values (< 12, 12–23, and ≥ 24 months or none, < 24, and ≥ 24 months). All 3 studies that analyzed the effect of breast feeding duration on osteoporosis in postmenopausal Korean women were homogeneous (χ2 = 1.843, df = 2, P = 0.398; I2 = 0%); thus, the effect size was derived by a fixed-effect model. In these studies, the effect size of breast feeding duration on the risk of osteoporosis was 1.93 (95% CI = 1.28–2.93), which was statistically significant (Z = 3.108, P = 0.002) (Fig. 3). The funnel plot did not show any publication bias, which was supported by Egger test results.
Go to :
DISCUSSION
Although some systematic review studies [18192028293031] have investigated the relationship between parity or duration of breast feeding and the risk of osteoporosis, no consensus has been reached. The present study is important as it is the first meta-analysis to investigate the relationship between parity or duration of breast feeding and the risk of osteoporosis in postmenopausal Korean women alone.
Although our meta-analysis was limited by the fact that the studies we analyzed used different ranges of parity, the results showed that postmenopausal women with higher parity had a higher risk of osteoporosis compared to those with lower parity. Generally, the loss of calcium required for fetal growth and development during pregnancy causes a 3% reduction in bone density in the mother [32] and estrogen deficiency during the period of postpartum amenorrhea. Therefore, it is suspected that multiple childbirths may result in reduction in bone mass due to conception and delivery before bone mass has sufficiently recovered from the previous childbirth.
However, a meta-analysis on the effect of parity on bone density [19], conducted outside Korea, reported that parity did not have a significant effect on the femoral neck and lumbar spine, but primiparous or multiparous women showed significantly higher total femoral bone density compared to nulliparous women, which is contrary to the findings of the present study. However, the study population of all the studies included in that meta-analysis, except for one study, consisted of Caucasians, and included both premenopausal and postmenopausal women. Moreover, parity status was analyzed without categorization. Therefore, it would be difficult to make a direct comparison between the above study and the present study, which analyzed only postmenopausal Korean women. Bone mass may decrease due to increased calcium demand during pregnancy, and calcium absorption by the intestines increases due to increased estrogen concentration during the latter part of pregnancy. Increase in bone density may be caused by increased load on the bones due to increased body weight during pregnancy and increased physical activities during childrearing.
However, only a few studies in Korea have systematically investigated the effect of parity on the risk of osteoporosis, and they used different ranges of parity. Therefore, the threshold of parity with respect to the risk of osteoporosis could not be analyzed. Moreover, among the 7 studies included in the meta-analysis, only 2 showed a high-quality score. Sensitivity tests conducted with only these two studies of high quality showed that parity had not affected the risk of osteoporosis in the femur or lumbar vertebrae. Therefore, it is difficult to reach a definite conclusion on the impact of parity on the risk of osteoporosis in postmenopausal Korean women.
Meanwhile, WHO recommends exclusive breast feeding for the first 6 months after childbirth, and continuing breast feeding for 2 years or more [33]. However, there have been conflicting results on the effect of breast feeding duration on the risk of osteoporosis to date.
In the present study, postmenopausal women with longer durations of breast feeding showed a higher risk of osteoporosis in the lumbar spine or femur. Although the mechanism for regulating calcium metabolism during breast feeding is not well known, it has been reported to be mediated by a reduction in parathyroid hormone-related peptide and estrogen concentrations [34]. Because an average of 300–400 mg of calcium is lost daily to breast milk during breast feeding, the bone mass of mothers may decrease when the duration breast feeding is prolonged, despite the actions of regulating mechanisms that increase calcium retention in the kidneys and calcium reabsorption by the intestines [34]. In a study that analyzed data from 2010–2011 KNHANES [35], prolonged breast feeding lasting ≥ 37 months, increased the risk of osteoporosis in the lumbar spine of postmenopausal women, which supports the findings of the present study. However, a meta-analysis on the effect of breast feeding on the health of women reported that the duration of breast feeding did not have a significant effect on bone density [30]. In particular, the findings of the present study contradicts another study, which reported that a 4%–7% bone loss occurs in the lumbar spine and femur during breast feeding but that bone density returns to the previous state within 1 year from discontinuing breast feeding [36]. One study reported that breast feeding for only 6 months resulted in a reduction in bone density, which stopped after 6 months and returned to previous levels after another 6 months, whereas bone density did not return to original levels when breast feeding lasted ≥ 12 months [36]. In view of that study, identifying the threshold duration of breast feeding with respect to the risk of osteoporosis seems important. Therefore, it is necessary to longitudinally study changes in bone density according to the duration of breast feeding through cohort or prospective studies.
One of the strengths of the present meta-analysis is that homogeneity was assured since it integrated only results from studies that measured bone density by the same method in the same area among postmenopausal women alone. Even among menopausal women in the same population, bone density may be affected by the area measured, age of the subjects, and measurement method.
There were some limitations to this study. First, the cross-sectional studies included in the meta-analysis did not control for factors that can affect calcium metabolism during breast feeding, such as nutritional status, activity level, and change in body weight, and thus, their effects cannot be disregarded. Moreover, because only 3 studies were included in the meta-analysis, the threshold duration of breast feeding with respect to the risk of osteoporosis could not be analyzed. Furthermore, the joint effect of parity and duration of breast feeding could not be analyzed. Moreover, the small number of studies with different scale such as mean value, ranges included in the meta-analysis and low-quality studies may also have limited the generalization of the results.
However, it may be considered that women with longer duration of breast feeding are exposed to a greater risk of osteoporosis. Therefore, countermeasures for the prevention of hip fracture are needed for women with prolonged breast feeding.
In conclusion, the findings in the present meta-analysis showed that longer duration of breast feeding increased the risk of osteoporosis in the lumbar spine or femoral neck. On the other hand, the impact of parity on the risk of osteoporosis needs to be explored in future studies with high quality research designs.
Go to :
 XML Download
XML Download