

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Critically ill patients who require mechanical ventilation (MV) have shown improved survival over time due to interventions such as lung protective ventilation1 and advances in supportive care.2 Patients requiring MV have shown an estimated in-hospital mortality rates of 32% in the US3 and 31.4% in France.4
Higher hospital case volume has been associated with lower mortality high-risk surgical procedures56 and for critically ill patients.4789 The impact of case volume seemed more prominent in critically ill patients with the high severity of illness10 and in patients with gastrointestinal and respiratory diagnoses.8 While earlier studies reported that the higher case volume is associated with improved outcome in critically ill patients,78 more recent and large-scale studies have been unable to reproduce the effect.911 Moreover, the impact of critically ill patient case volume on long-term mortality has not been evaluated.
The objective of our study was to assess the impact of case volume on in-hospital and long-term mortality in critically ill patients who required MV for 48 hours or more. We hypothesized that higher institutional case volume may be associated with lower in-hospital and long-term mortality.
METHODS
Data source and study population
The National Health Insurance Service (NHIS) database contains all claims data for the population covered under the National Health Insurance (NHI) program and the Medical Aid program in Korea. The NHIS provides its database to researchers after de-identification of personal information to aid generation of real-world evidence.12
Adult patients (age ≥ 18) who received MV for 48 hours or more between 2008 and 2016 in the intensive care unit (ICU) were identified and extracted from the NHIS database by searching NHI codes AJ100, AJ110, AJ120, AJ130, AJ140, or AJ150 during hospitalization. Underlying comorbidities such as hypertension, diabetes mellitus, coronary artery disease, and chronic kidney disease (CKD), and cardiovascular disease were extracted from the database using International Classification of Diseases (ICD)-10 codes. The Elixhauser comorbidity index, derived from 30 disease entities using ICD-10 codes13 and shown to correlate with hospital mortality,14 was used as a covariable to adjust for severity of illness. The Elixhauser comorbidity system has been shown to be slightly superior to the previously used Charlson comorbidity system at adjusting for comorbidity.15
In-hospital mortality, ICU length of stay, and hospital length of stay were also extracted. Because death certificates are automatically reported to the NHI, long term (1, 3, 5 year) mortality was detected when healthcare coverage by the NHI was terminated due to death.
Definition of case volume
The case volume was defined as the average annual number of adult patients (age ≥ 18) who received MV for 48 hours or more. Case volume was categorized as follows; low case volume (< 300 cases/year), medium case volume (300–500 cases/year), and high case volume (> 500 cases/year).
Statistical analysis
Patient characteristics were compared according to case volume using the one-way analysis of variance or Kruskal-Wallis test for continuous variables and χ2 test or Fisher's exact test for categorical variables, respectively. In-hospital mortality according to case volume was assessed using logistic regression model after adjusting age, gender, comorbidities, and Elixhauser comorbidity index. The goodness-of fit for the logistic regression model was assessed using Hosmer-Lemeshow test. The Kaplan-Meier survival curve was derived according to case volume and the log-rank test was performed to compare the survival curve. The goodness-of fit for the Cox proportional hazard model was assessed using the likelihood ratio test and the proportional hazard assumption was explored using the log-minus-log plot. Clinical outcomes were compared according to case volume using the one-way analysis of variance.
All analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). Results were considered statistically significant when P values were less than 0.05.
RESULTS
A total of 158,712 patients received MV for 48 hours or more in 55 centers from January 2008 to December 2016 in Korea. Patient and center characteristics are presented in Table 1 with 38% (61,024) of patients admitted to high-volume centers, while 37.2% (58,997) and 24.4% (38,691) of patients were admitted to medium-volume and low-volume centers, respectively (Table1). About 72% of patients were admitted to hospitals in urban areas.
Table 1
Patient and center characteristics

Numbers reported as No. (%), median (IQR), and mean (SD).
IQR = interquartile range, SD = standard deviation, ICU = intensive care unit, LOS = length of stay.
![]()
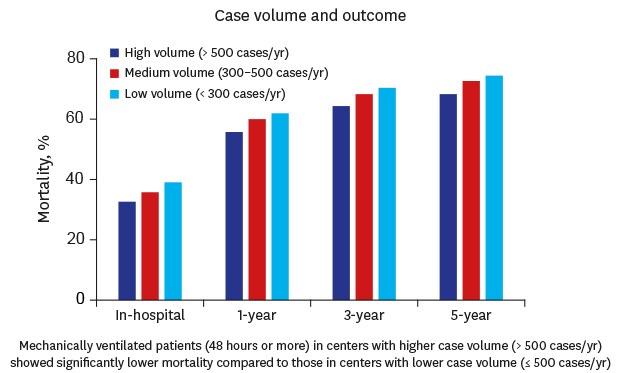
The overall in-hospital mortality rate was 35.4% (56,133/158,712). In-hospital mortality rates in high-, medium-, and low-volume centers were 32.6%, 35.8%, and 39.2%, respectively. The relationship between the average annual volume and in-hospital mortality rate is shown in Fig. 1.
 | Fig. 1Relation between the average annual volume and in-hospital mortality after mechanical ventilation for 48 hours or more.ICU = intensive care unit.
|
After adjusting for age, gender, comorbidities, and Elixhauser comorbidity index, medium-volume centers (adjusted odds ratio [OR], 1.13; 95% confidence interval [CI], 1.10–1.15; P < 0.01) and low-volume centers (adjusted OR, 1.33; 95% CI, 1.30–1.37; P < 0.01) showed significantly higher in-hospital mortality compared to high-volume centers (Table 2).
Table 2
Univariable and multivariable logistic analyses for in-hospital mortality

![]()
Low-volume centers were associated with higher 1-year and 3-year mortality compared with high-volume centers (Table 3 and Fig. 2). In low-volume and medium volume centers, older age, men, patients with CKD or cerebrovascular disease, and higher Elixhauser comorbidity index were identified as significant risk factors of long-term mortality (Table 3).
Table 3
Multivariable logistic analyses for 1-, 3-, 5-year mortality

![]()
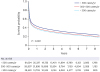 | Fig. 2Kaplan-Meier survival curve after mechanical ventilation for 48 hours or more according to the center volume.
|
Long-term survival for up to 8 years was also significantly higher in high-volume centers compared to or low-volume or medium-volume centers (P < 0.01) (Supplementary Fig. 1).
DISCUSSION
Higher case volume of patients receiving MV for 48 hours or more was associated with significantly lower in-hospital mortality and lower long term mortality for up to 8 years.
Typically, 20%–40% of ICU patients require MV16 and mechanically ventilated patients are at greater risk of death with disproportionately higher utilization of health care resources.1718 Studies have reported that hospitals with higher ICU patient volume tend to show lower adjusted mortality rates compared to hospitals with less ICU patients, although less so in the surgical population.7919 As significant resources and experienced medical personnel are required to provide quality critical care to ICU patients and also trauma patients, regionalization of critical care20 or trauma care21 have been proposed. The positive relationship between case volume and patient outcome, as also seen in our study, may provide additional basis for regionalized approach in critical care for patients requiring prolonged MV.
In our analysis, mechanically ventilated patients treated in centers with more than 500 cases per year showed better survival compared to patients managed in institutions with lower annual case volumes, even after adjusting for confounders. These results provide evidence for a relationship between volume and outcome in mechanically ventilated patients. Similar relationships between case volume and outcome have been reported in previous studies. Plausible explanations for the relationship include higher nurse-to-patient ratio and greater number of experienced staff as experience is likely to be gained more quickly in centers with higher case volume. Higher probability of multidisciplinary ICU teams comprised of various specialties and implementation of patient care protocols proven to increase survival such as lung protective low tidal volume ventilation and protocols for light sedation may also have played a role.2223
On the contrary, a study that analyzed the Australian and New Zealand adult ICU database was not able to demonstrate the previously reported relationship between higher hospital volume results and reduced in-hospital mortality.9 The study included all mechanically ventilated ICU patients regardless of the duration of MV, therefore patients requiring brief MV who were at lower risk of death were included. Another difference compared to our study and previous studies lies in that critical care in the two countries is state of the art with almost uniformly closed ICUs24 staffed with highly trained critical care nurses and intensivists. Considering that these factors may have attenuated the volume-outcome relationship, the case volume may play a role only in healthcare systems that include hospitals with relatively less resources and training.2526 Another study that used administrative data to evaluate the effect of case volume on death within 30 days in patients who were mechanically ventilated for more than 2 days also failed to show an association.27 Besides the lack of power to compare between the lowest case volume group and the other groups,28 more than 80% of the patients in the lowest group and 32% of patients in the second lowest group were transferred to larger hospitals. Therefore, a direct comparison between groups were inappropriate. Other studies have suggested that there may be a threshold beyond which mortality benefit is lost with increased case volume.2930 In addition, diagnosis also seems to be a factor as risk-adjusted mortality was decreased in patients within the same diagnostic category as hospital volume increased.31
The overall in-hospital mortality in patients who were mechanically ventilated for 48 hours or more was 35.4% in our study, which was comparable with previous studies.432 Patients who received prolonged MV and ICU care most likely require hospital follow-up due to cognitive, psychological, and physical impairment.3334 However, few studies have evaluated the association between case volume and long-term outcome in patients requiring prolonged MV. Only one study investigated long term mortality in mechanically ventilated patients and demonstrated that higher case volume were independently associated with lower 5-year mortality compared hospitals with lower case volume,34 which was consistent with our study. Our study also showed that higher case volume was associated with superior long-term mortality of up to 5 years.
Old age (≥ 70-year-old) and CKD were significantly associated with short and long-term mortality in addition to higher case volume in our study. Old age is a consistently reported predictor of in-hospital mortality in patients receiving MV.1735 CKD is a known risk factor of mortality in the general population36 as well as patients with heart failure37 or myocardial infarction.38 In accordance with our study, a recent study demonstrated that preexisting CKD had profound impact on 30 day- and 1-year mortality in critically ill patients requiring MV.39
The NHI program of Korea is a universal healthcare coverage system. It is provided by the NHIS, which is the single payer of the NHI program. The NHIS provides healthcare insurance to 97% of the population in Korea and the Medical Aid program supports the remaining 3% of the population with the lowest income.40 Whenever healthcare service is provided, the healthcare provider files for reimbursement to the NHIS and this claim is recorded in the NHIS database. The breadth and completeness of the NHIS database used in our study is one of the strengths of our study. In addition, only concrete outcomes such as mortality and length of stay were used as end points.
ICUs in Korea have features that are in stark contrast to ICUs in most developed countries. The vast majority of ICUs in Korea are operated as open units without dedicated intensivists due to the poor reimbursement scheme and late development of intensivists as a subspecialty. Also, respiratory therapists are yet to be acknowledged as a profession and bedside nurses are responsible for the respiratory hygiene of patients.
There are several limitations to consider when interpreting the results of our study. First, due to the administrative nature of the NHIS database used in our study, clinically relevant variables are lacking. Risk adjustment is a critical issue in studies using administrative data that were constructed without consideration for research. As performed in our study, adjusting for comorbidities using indices derived from comorbidities and evaluating concrete outcomes such as in-hospital and long-term mortality may considered to be most optimal when analyzing administrative data. Second, due to the relatively long study period, outcomes may in patients receiving MV for 48 hours or more have been affected by medical advances during the study period. However, considering the long history of lung protective ventilation and that advances in medicine were universally accessible, we believe that the impact of a relatively long study period is likely to be uniform and minimal. Third, admission diagnoses or the nature of the ICU admission (medical vs. surgical) could not be discriminated. However, patients who received MV for less than 48 hours were considered to have low severity of illness and were excluded. According to a comprehensive report on ICUs by the Korean Society of Critical Care Medicine, only 10% of ICU patients were admitted for postoperative management. Therefore, the study population may be mostly severely ill medical patients.
Despite these limitations, our study has some important implications. Our study is the first nationwide population-based study to investigate the relationship between case-volume and in-hospital and long-term mortality in patients who were mechanically ventilated for 48 hours or more. In addition, selection bias was minimized by using the NHIS database, which includes all patients receiving MV for 48 hours or more in Korea.
In conclusion, mechanically ventilated patients (48 hours or more) in centers with higher case volume (> 500 cases/year) showed significantly lower in-hospital and 1-year mortality compared to those in centers with lower case volume (≤ 500 cases/year). Long-term survival was also superior in high-volume centers.
 XML Download
XML Download