

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Out-of-hospital cardiac arrest (OHCA) remains a challenge worldwide.1 In North America, approximately 134 OHCA events occur per 100,000 adults annually and the survival rate is 3%–16%.2 To improve OHCA outcomes, many countries are applying various strategies to their emergency medical services (EMS).123 Previous reports of prehospital EMS interventions, including dispatch type, airway management, and the number of emergency medical technicians (EMTs) have been reported.4567891011 Among these, multi-dispatch response to an OHCA, using more than two EMS teams of the same or different tiers, have shown some positive effects.67111213 In Korea, to reduce response time and to increase the number of EMTs at an OHCA, a dual-dispatch system started in March 2015. We investigated the OHCA patient outcomes in Daegu Metropolitan City from March 1, 2015 to June 30, 2016, to identify the effectiveness of dual-dispatch system.
METHODS
The EMS system in Daegu metropolitan city
Daegu metropolitan city is located on the south-eastern side of the Korean peninsula, with an area of 883.56 km2 and a population of 2,487,829.14 Major hospital EMS are provided by one regional emergency medical center and four local emergency medical centers. Of 1,325 OHCA patients, approximately 90% were hospitalized at these five hospitals in 2016.15 For the prehospital EMS, the Daegu 119 call center operates 47 ambulances at 48 safety centers through the regional fire safety central office.16 Each prehospital EMS team comprises three EMTs, including one level-1 EMT (similar to EMT-intermediate level in U.S. EMS) as the highest-level ambulance crew, one level-2 EMT (similar to EMT-basic), and driver.317 Both scopes of practice are limited to the basic life support (BLS) level and provide manual chest compressions.18 For level-1 EMT, advanced airway and intravenous access could be attempted under direct medical direction. On March 1, 2015, the Daegu 119 started dual-dispatch, a protocol that uses two EMS teams at OHCA. In this protocol, 119 uses one EMS team generally, but if OHCA is recognized by the dispatch center, two EMS teams respond with available ambulances.
Study participants and data collection
On January 1, 2014, the Daegu Emergency Medical Cooperation Bureau began a citywide prospective population-based clinical registry for gathering information regarding OHCA patients from the prehospital phase to hospital discharge, connecting EMS and hospital data, based on the Utstein style (Daegu emergency medical services registry [DEMSRe]). This study used DEMSRe data from March 1, 2015 to June 30, 2016, during the dual-dispatch system operation period.
Of 1,476 OHCA patients, we excluded those aged < 18 years because the etiology of cardiac arrest between adults and pediatric patients is generally different. Second, patients for whom EMS resuscitations had not been attempted were excluded. Third, patients with OHCA witnessed by EMTs (the patient experienced arrest following the arrival of EMTs) were excluded, because Utstein style recommends that arrests witnessed by EMS personnel should be separated from the unwitnessed arrests or from the bystander witnessed arrests. Fourth, OHCA patients with a non-cardiac etiology were excluded. Fifth, we excluded patients for whom the in-hospital managements were not followed, because of the patient being pronounced dead on arrival (DOA) at hospital or “do not attempt to resuscitate (DNAR)” instructions. Sixth, we excluded patients with insufficient records. Lastly, patients who experienced arrest at a nursing home were excluded because pre-existing co-morbidities could interfere. After exclusions, 898 patients were included.
For prehospital data, we identified age, gender, place of cardiac arrest, witnessed or not, bystander cardiopulmonary resuscitation (CPR) provided, first recorded electrocardiography (ECG) rhythm, recognition of cardiac arrest by a dispatcher at a 119 call center, activation of dual-dispatch, and prehospital return of spontaneous circulation (ROSC) of OHCA patients, using 119 call center records. Additionally, we identified prehospital time-related variables, such as emergency call time, scene site arrival time, first defibrillation time in patients with a shockable rhythm, departure time, and hospital arrival time. Using hospital data, we identified underlying disease, implementation of targeted temperature management (TTM) or coronary angiography (CAG), survival or not, and the cerebral performance category (CPC) score in patients who survived.
DEMSRe Works collected prehospital data from quality managers in 119 call centers on alternate weeks, and collected hospital data from researchers in each of the hospitals. The DEMSRe Works data managers linked the two datasets, and calculated the response time (time from the emergency call to EMS arrival at the scene site), on-scene time (time from EMS arrival to departure for the hospital), transport time (time from EMS departure to arrival at the hospital), and first defibrillation interval (time from EMS arrival at the scene site to first defibrillation in patients with a shockable rhythm). The data were then analyzed for quality control.
Outcome measures
The primary outcome was survival discharge, with secondary outcomes including neurological recovery. Neurological recovery was classified as “good” or “poor,” based on the CPC score at the time of discharge from the final hospital. A CPC score of 1 or 2 was classified as “good”, and CPC scores between 3 and 5 were classified as “poor”. Data collection commenced following approval from the Institutional Review Board committee of each research institute in the five hospitals.
Statistical analysis
Patient characteristics, prehospital elements, and in-hospital processes were evaluated according to dispatch type. For continuous variables, the median and interquartile range (IQR) were calculated, and a Mann-Whitney U test was performed. For categorical variables, percentages were calculated, and a Pearson's χ2 test was performed.
To determine the effect of each dispatch type on OHCA outcomes according to on-scene time, associations were examined after classifying each dispatch type into two groups, according to each minute of on-scene time. As a result, the direction of the association between the two groups showed the greatest difference on the basis of 10 minutes.
To identify homogeneity between the two dispatch types within the two stratified groups, Breslow and Day`s tests were performed with OHCA outcomes according to the 10 minutes of on-scene time, and logistic regression analyses were performed with each element of the prehospital phase of OHCA as an independent variable in each group. Simultaneously, multiple logistic regression analysis was performed using possible confounding factors together as a covariate in each group, to determine the influence of dual-dispatch on OHCA outcomes in accordance with the stratified on-scene time.
All statistical analyses were performed using IBM SPSS version 21.0 (IBM Co., Armonk, NY, USA). A P-value of < 0.05 was considered statistically significant.
RESULTS
Overview
During the study period, 1,476 OHCA patients had been admitted to the study hospitals via Daegu 119 ambulances. Of these, 578 patients were excluded, comprising 44 patients aged < 18 years, 51 patients for whom EMS resuscitations had not been attempted, 82 patients whose OHCA was witnessed by EMTs, 256 patients of non-cardiac etiology, 93 patients who were DOA, DNAR, or who had insufficient records, and 52 patients who experienced arrest at a nursing home. Finally, 898 patients were included in the study population (Fig. 1).

Patient characteristics
Table 1 shows the OHCA patient characteristics. The median age was 69.0 years (IQR, 56.0–78.0 years), and 65.5% were men. The most frequent OHCA site was at home (74.1%). Witnessed cases comprised 56.5% (60.5% for the single-dispatch group [SDG] and 52.9% for the dual-dispatch group [DDG], P < 0.022), and bystander CPR was performed in 53.7% (40.0% for the SDG and 65.6% for the DDG, P < 0.001). A shockable initial ECG was present in 19.3% of patients (19.9% for the SDG and 18.8% for the DDG, P < 0.675). Dispatchers at emergency call centers recognized 57.8% of the OHCAs (36.6% for the SDG and 76.3% for the DDG, P < 0.001). Prehospital ROSC was 10.7% (12.0% for the SDG and 9.6% for the DDG, P = 0.250), survived discharge was 7.6% (8.9% for the SDG and 6.5% for the DDG, P = 0.176), and good neurological survival was 5.9% (6.7% for the SDG and 5.2% for the DDG, P = 0.345).
Table 1
Out of hospital cardiac arrest patient characteristics

Data are presented as median (interquartile range) or number (%).
CPR = cardiopulmonary resuscitation, ECG = electrocardiography, Dispatcher recognition = recognition of cardiac arrest by dispatcher at public emergency medical services call center, ROSC = return of spontaneous circulation, CPC = cerebral performance category.
Prehospital performance and hospital management
Table 2 presents prehospital EMS performance and hospital management, according to the two dispatch types. The median response time was 7.0 minutes (IQR, 5.0–9.0) for the SDG, and 6.0 minutes (IQR, 5.0–8.0) for the DDG (P = 0.008). The median on-scene time was 11.0 minutes (IQR, 8.0–15.0) for the SDG and 13.0 minutes (IQR, 10.0–16.8) for the DDG (P < 0.001). However, the median transport time was same between the two groups, at 6.0 minutes. Additionally, the median first defibrillation interval was same between the two groups, at 3.0 minutes. An advanced airway was implemented in 42.6% and 73.8% of OHCA patients in the SDG and the DDG, respectively (P < 0.001), and intravenous access was implemented in 5.0% and 21.9% of OHCA patients in the SDG and the DDG, respectively (P < 0.001). TTM was implemented in 3.1% and 1.7% of OHCA patients in the SDG and the DDG, respectively (P = 0.153), and CAG was implemented in 8.4% and 6.9% of OHCA patients in the SDG and the DDG, respectively (P = 0.397).
Table 2
Prehospital EMS performance and hospital management in out-of-hospital cardiac arrest

Data are presented as median (interquartile range) or number (%).
IQR = interquartile range, TTM = targeted temperature management, EMS = emergency medical services.
aTime from the emergency call to EMS arrival at the scene site; bTime from EMS arrival to departure for the hospital; cTime from EMS departure to arrival at the hospital; dTime from EMS arrival at the scene site to first defibrillation in patients with shockable rhythm.
Effect of dual-dispatch on OHCA patient outcomes according to on-scene time
Table 3 shows OHCA outcomes according to on-scene time. For stratification per minute of on-scene time, 10 minutes of on-scene time presented the greatest variation in homogeneity using Breslow and Day's tests in relation to survival discharge (P = 0.238 for an on-scene time < 10 minutes; P = 0.027 for an on-scene time ≥ 10 minutes; and P = 0.005 using Breslow and Day's test) and neurological outcome (P = 0.060 for an on-scene time < 10 minutes; P = 0.028 for an on-scene time ≥ 10 minutes; and P = 0.027 using Breslow and Day's test).
Table 3
Out of hospital cardiac arrest outcomes according to on-scene time and dispatch types

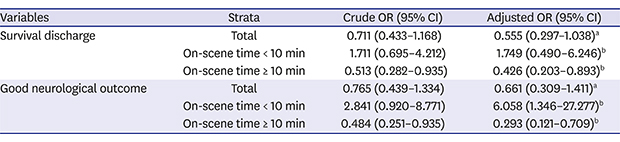
Table 4 shows multivariate logistic regression analysis of the effect of dual-dispatch in OHCA outcomes according to stratified on-scene time per 10 minutes. Dual-dispatch was not associated with better OHCA outcomes in the entire study population (adjusted odds ratio [aOR], 0.555, 0.661; 95% confidence interval [CI], 0.297–1.308, 0.309–1.411 for survival discharge and good neurological outcome, respectively). However, in situations where the on-scene time was < 10 minutes, dual-dispatch was associated with better neurological outcome (aOR, 1.749, 6.058; 95% CI, 0.490–6.246, 1.346–27.277 for survival discharge and good neurological outcome, respectively). Additionally, in situations where on-scene time was ≥ 10 minutes, dual-dispatch was associated with worse OHCA outcomes (aOR, 0.426, 0.293; 95% CI, 0.203–0.893, 0.121–0.709 for survival discharge and good neurological outcome, respectively).
Table 4
Multivariate logistic regression analysis of the effect of dual-dispatch in OHCA patient outcomes according to stratified on-scene time

ORs are calculated using single-dispatch as dummy variable.
OHCA = out-of-hospital cardiac arrest, OR = odds ratio, CI = confidence interval, ROSC = return of spontaneous circulation, CPR = cardiopulmonary resuscitation, ECG = electrocardiography.
aAdjusted for age, gender, underlying disease, witness existence, bystander CPR, initial ECG rhythm, place of cardiac arrest, airway management, intravenous access, response time, transport time, on-scene time; bAdjusted for age, gender, underlying disease, witness existence, bystander CPR, initial ECG rhythm, place of cardiac arrest, airway management, intravenous access, response time, transport time.
DISCUSSION
In this prospective observational study, dual-dispatch did not produce better outcomes in terms of survival discharge and neurological outcome compared to single-dispatch. However, with stratified analysis according to on-scene time, we found that if the on-scene time was < 10 minutes, dual-dispatch resulted in better neurological outcome than single-dispatch, and if the on-scene time was ≥ 10 minutes, dual-dispatch resulted in worse survival discharge and neurological outcome than single-dispatch.
Early recognition, prompt EMS activation, high-quality chest compressions, and early defibrillation are key components for favorable outcomes for OHCA patients.19 For this purpose, various strategies are operating in each EMS system, and there have been reports that a dual-dispatch could improve outcomes.56111213 However, the effect of dual- or multi-dispatch for OHCA could differ depending on demographic characteristics, medical resources, EMT scope of practice, and type of system.2021 For example, multi-dispatch and multi-tier are different concepts. Multi-dispatch means an OHCA response using multiple EMS teams, and multi-tier means an OHCA response using multiple EMS teams with different scopes of practice. Therefore, a multi-tier includes the concept of multi-dispatch, but multi-dispatch may or may not be multi-tier. Additionally, there are no definite guidelines indicating the best-operation model, and effect of multi-dispatch might vary according to each EMS system.
The aim of a dual-dispatch was to reduce the response time and provide high-quality CPR through increasing the number of EMTs. For OHCA, faster response time is a positive factor; however, optimal on-scene time remains controversial, and other factors could influence outcomes.2223 In this study, response time was reduced and on-scene time was increased in the DDG, but outcome improvement through dual-dispatch could not be proven. One possible reason for this is application of additional procedures and prolongation of the on-scene time. In this study, advanced airway and intravenous access were implemented more in the DDG. However, chest compression quality could be compromised when applying prehospital procedures, the effect of prehospital advanced airway in OHCA is still unclear, and the on-scene time could be extended due to these procedures.2425 Previous studies have reported negative effects of extended on-scene time on OHCA patients in BLS-based EMS systems. Kim et al.26 reported that 4–7 minutes of on-scene time was associated with better neurological recovery for OHCA patients, using an intermediate level EMS. Kim et al.27 reported that a prolonged on-scene time resulted in negative effects for OHCA patients in the “scoop-and-run” EMS model. Shin et al.28 reported that between 8 and 16 minutes of on-scene time was associated with good neurological outcome. Our EMS system provides BLS-based intermediate level EMS, basically the “scoop-and-run” model. We thought that the on-scene time was extended as more procedures were applied in the DDG, and this may explain why the positive effect was not seen across the entire DDG. Therefore, efforts should be made to improve CPR quality and reduce the shock delivery interval using dual-dispatch.
The BLS-based EMS system is applied in various regions, including many Asian countries, but there has been little evaluation of the on-scene time according to the number of EMTs for OHCA.26272829 In this study, the DDG showed better neurological outcome if the on-scene time was < 10 minutes. This could help determine the optimal on-scene time for OHCA in regions with BLS-based EMS systems.
Our study has several limitations. First, the proficiency of prehospital airway management was not assessed. There is no recommendation regarding a particular airway device for OHCA, but proficiency of EMT could have differed between teams and this difference might have influenced outcomes.4924 Second, we estimated in DDG that the quality of CPR would be better, but real-time quality measurements were impossible. In addition, the analysis included only the attempted rate of endotracheal intubation and IV access, but there were limitations that did not include accurate data related to more important information, endotracheal intubation, IV access success rate and time spent on processing. Third, detailed in-hospital management information, such as TTM timing, were not considered in our study. However, these cases only accounted for a very small percentage. Fourth, this study was citywide and investigated in the BLS-based system. Additionally, there was not enough study population in subgroup analysis, and it was possible that statistical significance was not obtained sufficiently. Therefore, our conclusion has limited generalizability and we cannot extrapolate our findings to advanced life support-based systems. Further studies with larger numbers or different EMS systems, such as nationwide or international investigation will be needed. Fifth, it could be possible that only cardiac arrest cases that were not recognized as such could have received single dispatch in our design. It may be that these cases that present in an atypical manner, causing the dispatcher to fail to recognize them as cardiac arrest, have a different baseline survival or neurologically intact survival rate. Therefore, further studies, such as those with a randomized design may be needed. Finally, while we considered covariates to the best of our ability, residual confounding factors may have existed.
Best practice guidelines of on-scene time for OHCA patients are still controversial. In this study, single-dispatch and dual-dispatch did not show differences in OHCA outcomes based on BLS-based EMS system. However, dual-dispatch had a positive effect on neurological outcomes after OHCA involving an on-scene time of < 10 minutes, and had a negative effect on both survival discharge and neurological outcomes, involving an on-scene time of ≥ 10 minutes. Although this result was derived from subgroup analysis, we believe it should be considered in future EMS policies.
 XML Download
XML Download