

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION TO UT-HEART
With advancements in computational science bolstered by high-performance computing technology, it is now possible to reproduce the human heartbeat in a realistic three-dimensional simulation heart model implemented with mathematical models of functional molecules. The development and advancement of various novel diagnostic modalities require that heart simulators are not just multiscale but also multiphysics, to accurately compare with and examine multifaceted clinical data. Thus, we have developed a three-dimensional, multiscale, multiphysics heart simulator (UT-Heart). This simulator integrates the molecular and cellular mechanisms of cardiac excitation and contraction to reproduce the cardiac electrophysiology at the organ level and hemodynamics based on a finite element method with parallel computation [1].
First, we developed a method for analyzing fluid-structure interaction problems based on the arbitrary Lagrangian-Eulerian method [2], preconditioned iterative linear solvers for problems with constraint conditions [3], and a nonlinear homogenization method with low computational cost [4] as the numerical technique to realize the multiscale, multiphysics heart simulator. In our work, within the field of basic physiology, we also developed a three-dimensional cardiomyocyte-based model with the reproduction of detailed subcellular structures, including metabolism [56], a rational formula for accurate analysis of cardiac excitation propagation to overcome self-contraction of the bidomain equation [7], an excitation-contraction coupling model with the cooperativity effect [89], and an algorithm that optimizes the ventricular fiber structure of the human heart [10]. Moreover, we also investigated how the sinus of Valsalva relieves abnormal stress on aortic valve leaflets [11], developed a new echo-tracking method with deformable regions of interest aimed at rational pattern matching [12], and clarified the mechanism by which line block is generated in a non-contact mapping system using a heart simulator [13].
For the analysis of electrical phenomena in the heart, we reproduced the normal 12-lead electrocardiogram (ECG) tracing by using the finite element method [14]. This involved using the original, parallel, multilevel technique for solving the bidomain equations on a human heart with the use of Purkinje fibers and a human torso model [15]. For the analysis of mechanical phenomena in the heart, we started with the simulation of blood flow, left ventricular wall motion, and the relationship between them by fluid-structure interaction [1617]. We also established a multiscale heart simulation method that integrates the microscopic stochastic sarcomere kinetics into the macroscopic heartbeat via the mesoscopic myocardial cell assembly using a supercomputer [1819]. Although assembling these components to construct a comprehensive whole heart model was expensive in terms of computation, we have successfully achieved this, as shown in Fig. 1. We have also been granted numerous patents for this work (e.g., [2021]).We now intend to put UT-Heart to practical use in clinical medicine and pharmacology. In this article, we will focus on its application in predicting the effect of cardiac resynchronization therapy (CRT) and assessing the proarrhythmic risk of drugs. First, we review patient-specific heart models with realistic three-dimensional morphology based on clinical data recorded before treating nine patients with heart failure and conduction delay using biventricular pacing. Each model was individualized to reproduce the surface electrocardiography, echocardiography, and hemodynamic measurements corresponding to each patient. Next, we reviewed a system for assessing proarrhythmic risk combining in vitro channel assays and in silico simulation of cardiac electrophysiology using the developed UT-Heart. Furthermore, we extend this approach and develop a comprehensive hazard map on the various combinations of ion channel inhibitors using the RIKEN's K computer.
PREDICTING THE EFFECT OF CARDIAC RESYNCHRONIZATION THERAPY
Extensive clinical research and basic studies have suggested potential biomarkers associated with the therapeutic responses of individual patients treated with CRT. However, it was found that a significant proportion (~30%) of patients do not benefit from this invasive therapy. To overcome this problem, computer simulations of CRT have been widely used to study the mechanisms underlying the therapeutic effects of this approach [2223]. As described above, we have developed a heart simulator in which propagation of excitation, contraction and relaxation, development of pressure, and blood flow are reproduced based on molecular models of cardiac electrophysiology and excitation-contraction coupling. We also succeeded in performing patient specific simulation of body surface ECG before and after CRT [24]. By applying these technologies, we created an individualized simulation model of the heart to determine whether the effects of CRT could be predicted in a canine model of heart failure with a left bundle branch block [25]. We further extended this approach to test the predictive ability of our simulator as a tool for the patient-specific evaluation of pathophysiology in a retrospective study. For nine patients treated with CRT, we created patient-specific heart models of the failing heart with ventricular desynchrony based on the clinical data recorded before treatment, and performed CRT simulations according to the actual cardiac pacing protocol. The simulation results of the effects of CRT correlated well with the clinical parameters that reflected the therapeutic effect. Thus, we demonstrated the utility of patient-specific CRT simulation and its possible application in future clinical practice [26].
The outline of our multiscale, multiphysics heart simulator and the technique for its individualized application are shown in Fig. 2. Details of mathematical models and calculation methods are previously reported [26].
(1) Patient-specific three-dimensional finite element (FE) models of the ventricles and upper body (torso) were reconstructed using multi-slice computed tomography (multi-scale CT) or magnetic resonance imaging data.
(2) These ventricular models with realistic morphology and made using fiber structure were subdivided into FEs. The molecular models of the excitation-contraction coupling process and electrophysiological models representing endocardial, M, or epicardial cells were implemented for these elements.
(3) The standard 12-lead ECGs recorded from the patients before CRT were reproduced through simulation by identifying the earliest activation sites and timing of activation in an iterative manner.
(4) Each model was individualized to reproduce the measurements of hemodynamic monitoring for each patient. Simultaneously, the lumped parameter models of the systemic and pulmonary circulations and time-varying elastance models of the atria were connected to the FE heart model, and the parameters were adjusted accordingly for each patient.
(5) CRT simulation was performed for each heart model without making any changes to the heart or circulation parameters determined during baseline simulation. The positions of the pacing leads were estimated using biplane chest radiography or CT images, wherever available, and then adjusted to reproduce the 12-lead ECG for pacing.
From the simulation results, we calculated the width of the QRS, ejection fraction (EF) in the left ventricle, and maximum value of the time derivative of left ventricular pressure (dP/dtmax). Clinical outcome was evaluated according to the improvement in EF indicated on the ultrasound cardiogram.
Examples of the simulated and actual ECGs before and after CRT for the standard 12 leads are shown in Fig. 3A. The patient in Fig. 3 suffered from complete atrioventricular block and had already been implanted with a pacemaker in the right ventricle. The simulated ECGs agreed well with the actual recordings by reproducing a wide QRS pattern before treatment. The corresponding excitations and contractions in these ECGs are shown in Fig. 3B. As seen in the figure, normal excitation propagated only from the right ventricle before treatment (Fig. 3B, top row). Presence of biventricular pacemaker excited both the ventricles from the basal side (Fig. 3B, bottom row). The electromechanical simulation coupled with the systemic and pulmonary circulations allowed the evaluation of the hemodynamic effects of CRT. As a ventricular aneurysm caused due to the thinning of the myocardium can be corrected by biventricular pacing, CRT increased the EF with a concomitant rise in the end-systolic pressure, indicating improved contractility (end-systolic elastance) as shown in Fig. 3C. This improvement was further substantiated by an increase in dP/dtmax (Fig. 3D).
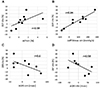
In the nine patients studied, CRT increased the EF by 8.7 ± 5.7% (range −19% to 41%), according to the clinical records. Simulated improvements in EF by CRT (ΔEFsim) weakly correlated with the clinically observed improvements in EF (Fig. 4A). The simulated improvements were also much smaller than those seen clinically. However, there was a tight correlation of the clinically observed improvement in EF and the simulated increase in dP/dtmax (ΔdP/dtmax sim) (Fig. 4B). These findings suggest that dP/dtmax (r = 0.94) is a better predictor of CRT responses than EF (r = 0.59). Although the simulation effectively reproduced the clinical changes in a QRS duration, the clinical and simulated changes in the QRS duration (ΔQRSsim and ΔQRSclin) did not correlate with the clinical improvement in EF (Fig. 4C and D). This discrepancy between electrical and mechanical improvements in dyssynchrony is consistent with earlier clinical observations.
Multiscale, custom-made heart simulation can reproduce most of the pathophysiology of the failing heart and responses to CRT, thereby, providing mechanistic insight into the pathophysiology of heart failure due to ventricular conduction block. Although this is a retrospective study with a limited number of subjects, the predictive ability of this simulation technique warrants further examination with regard to future clinical applications.
IN SILICO CARDIAC SAFETY ASSESSMENT OF DRUG EFFECTS ON MULTIPLE IONIC CURRENTS
Cardiac arrhythmias are a serious adverse effect of commonly used drugs. Among these, torsade de pointes (TdP) is a rare but potentially lethal type of ventricular arrhythmia often caused by inhibition of repolarizing potassium current of cardiac myocytes. The historical incidence of drug-related sudden cardiac deaths led to the establishment of regulatory requirements for cardiotoxicity testing, which include the measurement of repolarizing potassium current through the human ether-a-go-go-related gene (hERG) potassium current, in vivo QT assay in an animal model, and the examination of QT interval in healthy volunteers (a thorough QT study). However, these tests are costly and can sometimes lead to false-positive results, therefore, to overcome these issues, regulatory agencies have announced the future implementation of a new paradigm incorporating computational integration of a multiple ionic current assay into a cardiomyocyte model [272829]. Although the use of a cellular model is expected to greatly facilitate the screening process, accurate prediction of arrhythmia due to complex interactions among different types of cells in the heart tissues requires organ-level simulation. We proposed a system for assessing risk of proarrhythmia by combining in vitro channel assays using automated patch clamp technique and an in silico simulation of cardiac electrophysiology using UT-Heart (Fig. 5) [30]. The inhibitory effects of drugs are analyzed for the six ion channels (rapid delayed rectifier potassium current, sodium current, L-type calcium current, slow delayed rectifier potassium current, inward-rectifier potassium current, and transient outward potassium current), and the effects of drugs under various plasma concentrations are reproduced by changing the parameter values of 22 million cells implemented in the heart model. Our system succeeded in accurately predicting the arrhythmogenicity of 12 drugs (quinidine, D,l-sotalol, amiodarone, E-4031, cisapride, astemizole, terfenadine, bepridil, moxifloxacin, verapamil, dofetilide, and ranolazine) known to increase the risk of TdP, through the in vitro measurement of blocking actions on multiple ionic currents by reproducing a realistic human 12-lead ECG in silico. This heart simulator predicted proarrhythmic risk more accurately than the QT interval and hERG test. While all high-risk drugs can cause TdP at relatively low plasma concentrations, arrhythmia was not observed with safe drugs, even at high concentrations. Therefore, no false positive results were identified in our analysis. Various in silico methods have been proposed for accurate assessment of the risk of TdP induction by drugs.
This system can be applied to any drug candidate, but the requirement of a high-performance computer is an obstacle to its widespread use. To overcome this problem, we present a comprehensive hazard map of drug-induced arrhythmia based on an exhaustive in silico ECG database of drug effects, developed using RIKEN's K computer with performance of over 10 petaflops (SPARC64 VIIIfx, 705,024 cores; Fujitsu Ltd., Kawasaki, Japan [31]) [32]. We varied the extent of blocking of 5 ionic currents, which are known to affect arrhythmogenicity, incrementally by 10%, including that of rapid delayed rectifier potassium current (IKr: 0% to 100%), fast (INa: 0% to 40%) and late (INa,L: for this current, only 0%, 25%, and 50% blocks were tested) components of the sodium current, L-type calcium current (ICa,L: 0% to 40%), and slow delayed rectifier potassium current (IKs: 0% to 100%). Parallel computing on the K computer allowed us to obtain 9,075 patterns of electrophysiological simulations in 72,600,000 core hours. For every combination of current block, we simulated the electrophysiological activity of the heart and the associated 12-lead ECG to create a five-dimensional map of arrhythmia risk, in which the coordinates of the map represented the extent of block of each current. As we could not find a method to show a five-dimensional map in a single panel, we visualized the results in a five-dimensional presentation containing three-dimensional subspaces, where regions of arrhythmia were superimposed with the QT interval distribution. As the concentration-block relationship of each drug was traceable along a trajectory in these spaces, we were able to evaluate ECG changes and arrhythmogenicity (Fig. 6). This in silico ECG database facilitates the assessment of ECG characteristics and proarrhythmic risk without the need to computationally perform expensive heart simulations. Using this database, we can analyze the effect of each ion channel on the ECG characteristics (i.e., QRS duration and Tpeak-end, JT, and QT intervals) and the effect of this, in turn, on the risk of arrhythmias. Furthermore, because the safety margin of drugs at each concentration is assessed by the distance to the region of arrhythmia in these spaces, the database can provide not just the proarrhythmic risk, but also the margin of safety of these drugs. This database is now freely available at http://ut-heart.com/.
Drug-induced cardiotoxicity is not the only arrhythmogenic risk factor, heart's pumping function is also an important parameter to consider in cardiotoxicity testing. With UT-Heart, we can analyze the effect of drugs on pumping function. Fig. 7 demonstrates the pumping function during an arrhythmia provocation test. We applied an extra stimulus to the right ventricular apex in the presence of 12 times the free effective therapeutic plasma concentration range of cisapride. This led to early afterdepolarization (EAD) being induced that evolved to sustained ventricular arrhythmia. The area of EAD increased followed by a gradual increase in the frequency of excitation. Finally, the excitation evolved to ventricular fibrillation through TdP. The recorded history of blood pressure and left ventricular volume did not match the phase with corresponding electrocardiogram for arrhythmia (Fig. 7). Furthermore, the proarrhythmogenic risk of drugs sometimes conflicted with the negative cardiac inotropic effect. This can be exemplified with the fact that verapamil was found to be safe for arrhythmia in our simulation, as recognized clinically, despite significant QT prolongation on IKr inhibition [30]. However, on simultaneous inhibition of the L-type calcium current, verapamil caused a reduction in Ca transient in a dose-dependent manner. Such reduction in Ca transients, at the cellular level, results in impairment of ventricular pumping function, as shown by the small pressure-volume loops in Fig. 8. Verapamil is, thus, considered safe for arrhythmia, but it shows a significant negative effect on inotropic agents.
CONCLUSION AND PERSPECTIVE
We present a brief review of a method to predict the effect of CRT using a patient-specific simulator and a proarrhythmic risk assessment system combined with in vitro channel assays using automated patch clamp technique and an in silico simulation of cardiac electrophysiology. The patient-specific, multiscale heart simulation successfully predicted the response to CRT by reproducing the complex pathophysiology of the heart. With further verification, this technique may serve to be a useful tool in clinical decision-making. The database of cardiotoxicity under multiple ion channel block is freely available at http://ut-heart.com/; thus, it cannot just be used to assess the risk of drug candidates at any stage of R&D, but can also serve as a tool to design safe drugs without resorting to animal or clinical studies. Therefore, this database may constitute a high-throughput and cost-saving approach in the field of toxicology.
This 21st century approach based on heart simulation can revolutionize the process of drug discovery and decision-making in clinical medicine. This work is a breakthrough in computational biology, introducing a novel application of high-performance computation.







 XML Download
XML Download