

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The maxillary sinus is a critical anatomical structure for dental implant procedures on the maxilla. Depression of the sinus floor is a frequent finding that interferes with dental implant placement. In such cases, a sinus lift procedure may be required. Shanbhag et al. [1] observed residual ridge heights of ≤4 mm in nearly 50% of edentulous molar regions. This may be an indication for sinus floor elevation procedure to develop the implant site.
Several anatomical details are relevant for sinus lift procedures, including the residual ridge height; the maxillary sinus shape; the presence of an artery; and the presence, location, and appearance of sinus septa. Computed tomography (CT) is the technique of choice to evaluate these anatomical structures [23], as the residual ridge height determined using CT could affect the sequence of the treatment plan in terms of whether a 1- or 2-stage approach is chosen. Additionally, presurgical CT imaging can provide information regarding the location, size, and other clinical details of the anastomotic vessel in the maxillary sinus region. Neugebauer et al. suggested that a proper imaging evaluation be performed before sinus surgery based on the observation of a strong connection between the presence of septa and the complications and success rate of the procedures [4].
Few studies have evaluated the epidemiological distribution of sinus-related anatomy relevant for dental implant placement. The available data are focused on Caucasians, lacking Asian references [5]; however, these anatomical structures are likely to be different between Caucasian and Asian populations. Ball et al. [6] compared the head shapes of Caucasians and Chinese and observed significant differences, with a tendency for Chinese individuals to have a rounder head with a flatter back and forehead. Another study by Gu et al. [7] investigated the cephalometric norms of Chinese versus Caucasian young adults and found smaller midfaces in the Chinese group than in the Caucasian group. Differences in the head and maxillary structures could be indicative of further disparities in the maxillary sinus. In this study, we aimed to analyze the anatomy of the maxillary sinus over edentulous ridges in the bilateral posterior maxillary area in Taiwanese patients, using cone-beam computed tomography (CBCT).
MATERIALS AND METHODS
The medical protocol of this study followed the Core of Ethics of the World Medical Association (Declaration of Helsinki). The Institutional Review Board of Chang Gung Medical Foundation approved this study (approval No. 102-6030B).
Patients’ preimplant CBCT sample images obtained between 2012 and 2013 were collected for evaluation from Kaohsiung Chang Gung Memorial Hospital. These images displayed edentulous ridges extending from the first premolar to the second molar region. Patients with sinusitis and images of edentulous areas from unhealed extraction sites were excluded. CBCT images were acquired using the Asahi PSR 9000n device with a 4×4 cm field of view, tube voltage of 88 kV, current of 10 mA, scanning time of 20 seconds, and slice thickness of 0.1 mm. The Asahi Neo3D Client software (Asahi, Kyoto, Japan) was used to interpret the cross-sectional images.
The images were studied using various views. Slices were first oriented at the midcrest of the edentulous area (Figure 1).
 | Figure 1Images were studied in different views. Slices were first oriented at the midcrest of the edentulous area.
|
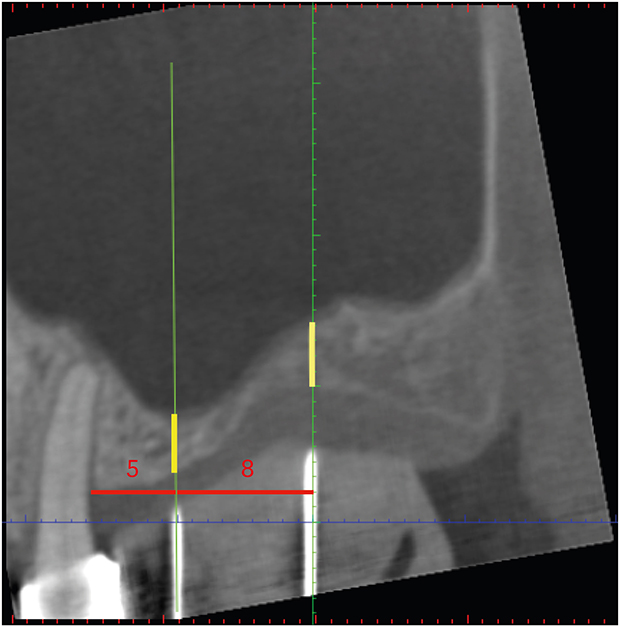
(1) Sagittal slices were used to determine the residual ridge height from the crest of the alveolar ridge to the sinus floor (Figure 2). The reference point for the ridge crest was the planned site of the dental implant. When a single tooth was missing, the midpoint of the edentulous ridge was used as the reference point. When multiple teeth were missing, the reference point was 5 mm from the neighboring tooth and 8 mm from the first point for the next implant site. The reference height was parallel to the axis of the neighboring tooth.
 | Figure 2In areas missing multiple teeth, the residual ridge height was measured from the crest of the alveolar ridge to the sinus floor at the planned site of the dental implant. The measurement point was 5 mm away from the neighboring tooth and 8 mm away from the first point of the next implant site.
|
(2) Coronal slices at the implant site were used to evaluate the width of the edentulous ridge. A horizontal line was drawn to measure the width at the reference point, which was 2-mm coronal to the edentulous crest (Figure 3).
 | Figure 3A horizontal line was drawn at the reference point, which was 2-mm coronal to the edentulous crest and was used to measure ridge width.
|
(3) The same view was used to measure the lateral wall thickness of the maxillary sinus. A perpendicular line drawn from the horizontal plane was used to make measurements 3- and 10-mm coronal to the sinus floor (Figure 4).
 | Figure 4A perpendicular line was drawn from the horizontal plane, and measurements were taken at 3- and 10-mm coronal to the sinus floor to measure the thickness of the lateral wall.
|
(4) With a sagittal view of the sinus septum, the height of the septum from the sinus floor was recorded.
(5) When coronal slices revealed the posterior superior alveolar artery (PSAA), its distance from the alveolar crest and diameter were recorded.
Statistical analyses, including a descriptive analysis and the Scheffé method for post hoc comparison, were performed using statistical software (SPSS version 12.0; SPSS Inc., Chicago, IL, USA). The descriptive analysis determined the mean, standard deviation, and range of the data. Differences in the residual ridge height, ridge width, and lateral wall thickness at the premolar and molar areas were analyzed using the Scheffé method for post hoc comparisons. The measurements of the residual ridge height and ridge width in our study had >95% power for detecting the difference between the means versus the alternative of equal means using the F test with a significance level of 0.05. The power calculation was performed using statistical software (G*Power 3.1). A P value <0.05 was considered to indicate statistical significance.
RESULTS
Subjects
We collected 101 CBCT scans of edentulous ridge areas from 61 patients (35 male, 26 female). Their mean age was 55.26±9.68 (range, 25–73 years). These 101 CBCT scans included 32 premolar and 69 molar regions. The independent t-test was used to compare the measurements according to gender, bilateral edentulous ridge and the number of missing teeth. No statistically significant differences were observed (P>0.089). Therefore, the data for subgroups defined by gender, bilateral edentulous ridges, and the number of missing teeth were merged for further statistical analyses. The intraclass correlation coefficient, as a measurement error, was 0.998, indicating high intrarater reliability.
Ridge width
The average ridge width was 10.26±3.16 mm (range, 4.34–19.07 mm). A significantly greater ridge width was observed in the second molar region than in the premolar and first molar regions (Table 1). Moreover, all of the ridge width narrower than 6 mm were present in the premolar regions.
Table 1
Ridge width

The average ridge width was 10.26 mm and the measurements revealed a significantly greater ridge width in the second molar region than in the premolar and first molar regions.
SD: standard deviation.
a)P<0.05, b)P<0.005.
![]()
Residual ridge height
The mean residual ridge height was 8.55±4.09 mm (range, 1.58–22.79 mm). In contrast to ridge width, we observed a significantly lower ridge height in the molar region than in the second premolar region (Table 2). A ridge height <10 mm was seen in 63 sites (62.3%), of which 51 were in the molar region. Insufficient bone height (<5 mm) was present at 23 sites (22.7%), all but 1 of which were located in the molar region.
Table 2
Residual ridge height


The mean residual ridge height was 8.55 mm and the measurements revealed a significantly lower ridge height in the molar region than in the second premolar region.
SD: standard deviation.
a)P<0.05, b)P<0.005.
![]()
Sinus septum and posterior superior artery
Measurements revealed a sinus septum at 6 sites (5.9%), with a mean height of 6.74 mm. The PSAA was observed at 25 sites (24.5%). The average distance between the alveolar crest to the PSAA was 17.11 mm, and the average arterial diameter was 1.22 mm (Table 3).
Table 3
Distance from the crest to the PSAA and diameter of the PSAA (n=25, 24.5%)

| Variables | Mean±SD (mm) | Range (mm) |
|---|---|---|
| Distance from crest to PSAA | 17.11±4.88 | 6.70–25.77 |
| Diameter of PSAA | 1.22±0.42 | 0.49–2.15 |
The PSAA was observed at 24.5% of the sites in our study. The average distance between the alveolar crest and the PSAA was 17.11 mm and the arterial diameter was 1.22 mm.
PSAA: posterior superior alveolar artery; SD: standard deviation.
![]()
Lateral wall thickness
The average thickness of the lateral wall of the maxillary sinus was 2.08±0.94 mm. The mean thickness of the lateral wall at 3- and 10-mm coronal to the sinus floor was 2.16±0.98 mm and 1.97±0.88 mm, respectively (Table 4). While no significant relationship between the tooth position and lateral wall thickness was observed, we observed that the lateral wall thickness increased from the premolar to molar region at 3-mm coronal to the sinus floor.
Table 4
Thickness of the lateral wall (mm)

No significant difference among these 3 positions was observed (P>0.773); however, we observed that the lateral wall thickness increased from the first premolar to the second molar region at 3 mm coronal to the sinus floor region.
LWT: lateral wall thickness; LWT-3 mm: mean lateral wall thickness at 3 mm coronal to the sinus floor; LWT-10 mm: mean lateral wall thickness at 10 mm coronal to the sinus floor; SD: standard deviation.
![]()
DISCUSSION
In this study, we assessed edentulous ridges and various anatomical structures related to implant placement in the maxillary sinus region. The average ridge width was 10.26 mm and the average residual ridge height was 8.55 mm. Statistically significant differences were observed between the second premolar and molar regions for both anatomical structures. We observed a significantly greater ridge width in the second molar region than in the premolar region, while the opposite outcome was found for the residual ridge height. Nunes et al. [8] reported similar data. Specifically, premolar sites exhibited a reduced crest width, but sufficient bone height for implant placement, while the opposite pattern was found at molar regions. We observed a ridge width of less than 6 mm at 5.89% of all sites, all in the premolar area, indicating that these areas were more likely to require ridge augmentation for standard-size implant placement. We observed residual heights of less than 10 mm in 61.76% of our data. Traditionally, appropriate osseous anchorage acquisition as a support for occlusal force requires a minimal length of 10 mm for a single unsplinted implant at molar site [8]. Recent long-term studies have shown that the survival rate and biological outcomes of implants shorter than 10 mm were similar to those of longer implants [91011], and the clinical advantages of short implants include less technique sensitivity in the surgical intervention, less morbidity by avoiding extensive bone augmentation procedures, increased number of sites available for implant therapy, and easier removal in case of failure [1213]. However, for most clinicians, if the goal is to place an implant longer than 10 mm, sinus lift procedure in the maxillary posterior area should be considered. A ridge height of <5 mm was recorded in 22.55% at the sites analyzed in this study, predominantly in the molar area, suggesting the need for more complicated surgical procedures due to insufficient bone height. Wang and Katranji [14] presented the ABC Augmentation Classification, according to which residual ridge height of <5 mm is categorized as class C. The failure rate of implants placed in ≤5 mm of residual bone was significantly higher than that of implants placed in >5 mm of residual bone. Sinus lift procedures can be performed via the lateral window or transcrestal techniques. The lateral window approach, originally described by Tatum et al. [1516] and Boyne and James [17], can achieve a substantial gain in bone height and can be performed using a 1- or 2-stage approach. While placing implants in areas with insufficient bone height in the maxillary posterior region, primary stability is the key to the implant's success. Reduced bone height might cause less contact between the bone and dental implant, leading to higher failure rates. Additionally, a minimal residual bone height of 6 mm is recommended for immediate implant placement during stabilization [18].
Maxillary septa and the PSAA are also important factors linked to a higher risk of complications following sinus lift procedures. The presence of a septum can increase the risk of membrane perforation and procedural difficulty [19]. We observed a 5.9% prevalence of septa, with a mean height of 6.74 mm. Our result is discordant with other studies, which have found the prevalence of septa in the maxillary sinus to vary between 25% and 31.7% [202122]. A study by Pommer et al. [22] reported a prevalence of septa of 28.4%, with a significantly higher rate in atrophic sinuses than in dentate maxillae.
The PSAA is a branch of the maxillary artery divided into intraosseous and extraosseous branches. The intraosseous branch of PSAA provides blood supply to the posterior bony wall and the sinus membrane, whereas the extraosseous branch supplies the attached gingiva and the mucosa of the maxillary posterior teeth region [23]. Güncü et al. [24] reported that the PSAA was observed in 64.5% of all sinuses, with the intraosseous branch observed in most cases (68.2%). The presence of the PSAA is linked to the risk of major complications during sinus lift procedures, including postoperative bleeding and hemorrhage [32526]. We observed that CBCT could detect the intraosseous branch of the artery in 24.5% of cases, which is a lower prevalence than the rates of 43.5% to 52.9% reported in previous studies of Caucasians [32427]. In the present study, the mean distance between the ridge crest and the PSAA was 17.1 mm, a lower value than the range of 18–19.6 mm that has been reported previously in Caucasians [232428]. We observed that the artery was located within 10 mm from the ridge crest at 2.94% of sites, suggesting that with a 5-mm height for a lateral window approach, damage to the artery during the procedure could be avoided if the residual ridge height is >5 mm; however, the distance between the ridge crest and PSAA ranged from 6.7 to 25.77 mm, indicating wide individual variation.
Sinus membrane perforation is a commonly reported complication of maxillary sinus lifting procedures [293031]. Techniques reported to reduce the risk of this complication include using a piezoelectric tip during preparation of the bony window [3233]; however, few studies have evaluated the thickness of the lateral wall of the maxillary sinus. The latter is also crucial during the lateral window approach while preparing a window. Previous observations suggest positioning the lower border of the surgical window either at the sinus floor or up to 3 mm above it [34353637]. Window size has varied across reports [383940]. Therefore, we used a vertical reference of 3- and 10-mm coronal to the sinus floor to measure the lateral wall thickness. We observed a mean thickness of 2.16 mm, whereas it was 1.75 mm in the study of Yang et al. [41] on Korean individuals. Their measurements were greater than those obtained for European skulls by Neiva et al. [42], who reported a mean thickness of 0.91 mm. The measurements in our study are higher than those reported in the Korean study. Potential ethnic differences should be investigated in further studies.
This study presents information on the residual ridge height, ridge width, prevalence and location of septa, presence of the PSAA, and lateral wall thickness in edentulous ridges of the maxillary sinus. All images analyzed in this study were obtained for implant therapy due to missing teeth; therefore, the exact timing of teeth loss is difficult to confirm. According to previous studies, the amount of resorption of the alveolar ridge is related to the duration of tooth loss [4344]. Therefore, a limitation of this study is the effect of the duration of missing teeth on edentulous ridge resorption. Although this study presents data on many anatomical features of the maxillary sinus relevant for sinus lift procedures, other anatomical factors should also be considered, such as the sinus floor shape, the angle between the buccal alveolar and palatal alveolar walls, and sinus membrane thickness [8184546]. We suggest further investigations of those anatomical features in the Taiwanese population in further studies.
In conclusion, the study presents data on the anatomical features of the maxillary sinus, which should be considered in sinus lift procedures for implant placement, in the Taiwanese population. A presurgical evaluation using CBCT to gather detailed information on the relevant anatomical structures is recommended to avoid procedural complications.
 XML Download
XML Download