

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pediatric hepatobiliary imaging is important for evaluation of congenital or structural disease as well as metabolic or diffuse parenchymal disease and tumors. A range of imaging modalities, including ultrasonography, magnetic resonance imaging (MRI), and computed tomography (CT) can be used for these purposes. In ultrasonography, echotexture analysis can be performed on conventional grayscale images. Both conventional Doppler imaging and advanced microvascular imaging can evaluate tissue vascularity and perfusion. Ultrasound (US) elastography can evaluate tissue stiffness, while contrast-enhanced ultrasonography (CEUS) can determine hemodynamic changes in pathologic conditions. Various sequences can be used to quantify hepatobiliary disease in MRI, including fat quantification, T2/T2* mapping, diffusion-weighted imaging (DWI), magnetic resonance (MR) elastography, and dynamic contrast-enhanced (DCE) MRI. Separately, even though ionizing radiation exposure is a concern, advanced CT techniques such as dual-energy CT (DECT) can differentiate between materials by using multi-material decomposition algorithms.
With these techniques, quantitative imaging can enhance the diagnostic accuracy for hepatobiliary diseases. Moreover, quantitative imaging results can be used to determine disease status and evaluate treatment response and follow-up. In this review, we present the use of each tool in the management of hepatobiliary disease in children, including discussions on the imaging techniques along with the relevant physics and clinical applications for patient care.
Imaging Techniques in Ultrasonography
Ultrasonography is the first modality of choice for imaging assessment of hepatobiliary disease in infants and children due to its widespread availability, easy accessibility, high resolution, and lack of the need for sedation.
Conventional Ultrasonography
The normal echotexture of the hepatic parenchyma in the pediatric liver generally does not differ from that seen in normal adult livers. Normal liver echogenicity is homogeneously low to intermediate and similar to that of the renal cortex or spleen, and the peripheral portal venous vasculature can be clearly seen (1). In cases with hepatic fat infiltration, increased liver echogenicity, a lack of distinction between vessels and bile ducts, posterior beam attenuation, poor diaphragm visualization, and a tightly packed echo pattern are observable (2). However, it is not always easy to quantify these imaging findings. This method has low accuracy with high variability and limitations in patients with high body mass indices.
The common bile duct should measure less than 1 mm in neonates, less than 2 mm in infants up to one year of age, less than 4 mm in older children, and less than 7 mm in adolescents and adults (1). In cases of hepatobiliary disease, splenomegaly can appear as a secondary finding. In children, the standard value for a normal spleen size increases with age, height, and weight (3).
Ultrasonographic Vascular Imaging
Doppler imaging employs the Doppler effect to generate images of the movement of fluids such as blood, and the relative velocity to the probe can be calculated by determining the frequency shift of a particular sample volume. A recent US microvascular imaging technique, superb microvascular imaging (SMI), has been designed for detection of subtle low-flow components (4). Both blood flow and tissue motion, called “clutter,” produce ultrasonic Doppler signals. Conventional Doppler ultrasonography uses a wall filter to remove clutter and motion artifacts, resulting in the loss of low-flow components. However, in comparison, SMI can separate flow signals from underlying clutter by using an adaptive algorithm.
US Elastography
US elastography employs ultrasonic echoes to observe tissue displacement as a function of time and space after application of a force. The displacement measurements can be performed using three approaches: 1) tissue displacement may be displayed directly, as in acoustic radiation force impulse (ARFI) imaging; 2) tissue strain may be calculated from the spatial gradient of displacement and displayed, producing what is known as strain elastography; or 3) when the force is dynamic only, the time-varying displacement data may be used to record the arrival times of propagating shear waves at various positions (5). Among these, different shear wave technologies have been developed, including transient elastography (FibroScan®, Echosens, Paris, France), point shear wave elastography (SWE), and two-dimensional (2D) or three-dimensional (3D) SWE. SWE uses sound waves to interrogate the mechanical stiffness properties of tissues and provides quantitative information on shear wave propagation.
When applying this technique in children, the use of different probes and acquisition depths to account for variable body sizes (67) and optimal acquisition numbers to reduce the scan time as much as possible should also be considered. Three acquisitions may be sufficient for hepatic shear wave velocity measurements in children older than six years regardless of breathing status; however, more acquisitions are recommended for children younger than five years (8). To enable a comparison between different US elastography techniques, the interconversion of elasticity measurements is also required (9). For an example, a phantom elasticity of 13.0 kPa can be considered as 8.8 kPa on the 1–6-MHz convex transducer of 2D SWE and 5.9 kPa on the M probe of transient elastography by using the reported equations.
The reported normal liver elasticity value using 2D SWE in children including newborns to 16-year-olds in one study was 4.29 ± 0.59 kPa (range: 2.7–5.76 kPa) (10). This prior investigation revealed that liver elasticity had a significant nonlinear association with age, since the values in neonates and infants as well as adolescents were significantly higher than those in children aged 2–12 years. A previous study using ARFI also demonstrated that the liver shear wave velocity changed with age in children older than 10 years (11). In clinical applications, however, liver shear wave velocity is often increased and elasticity is diminished because of variable conditions, including fibrosis, inflammation, congestion, portal hypertension, and cholestasis.
Contrast-Enhanced Ultrasonography
CEUS is a safe and highly sensitive imaging modality that does not involve radiation exposure to the patient or operator and can be used for evaluation of focal liver lesions, intra-abdominal parenchymal injuries, and organ transplantations in children (1213). Safety considerations regarding the intravenous use of US contrast agents in children have primarily focused on “off-label” usage, although a large cohort study of adults demonstrated a comparable adverse events rate (< 0.01%) to that seen with MRI procedures (13). The recommended dose of sulfur hexafluoride gas containing contrast in children is based on body weight, as follows: 0.03 mL/kg as an intravenous injection, up to a maximum of 2.4 mL per injection.
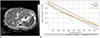
CEUS has shown comparable performance to that of CT and MRI in the pediatric work-up of focal liver lesions and blunt abdominal trauma in a systematic review (14). However, only a few studies have been conducted to date regarding the assessment of pediatric diffuse liver disease using CEUS. An animal study of rabbits demonstrated the feasibility of CEUS in evaluating liver fibrosis from biliary obstruction since the peak signal intensity of the liver was significantly associated with hepatic fibrosis grade (odds radio = 1.392; 95% confidence interval [CI], 1.114–1.741; p = 0.004) (Fig. 1) (15). This may indicate that CEUS can be used in liver fibrosis patients. However, further evaluation is needed.
Imaging Techniques in Hepatobiliary MRI
Fat Quantification
Measurement of the MR proton density fat fraction (PDFF) is a widely used method to quantify the amount of fat in the liver by using chemical shift gradient-recalled echo (GRE) sequence (16). Chemical shift imaging employs differences in precession frequencies in water and fat protons (17). In opposed-phase (OP) images, a difference in frequencies between water and fat causes a signal reduction, while in-phase (IP) images demonstrate increased signal intensities as a result of the addition of water and fat signals. By comparing these IP and OP images, the fat fraction can be quantified by using the following equation: fat fraction (%) = ([IP − OP] / [2 × IP]) × 100 (18). Application of a fast GRE technique in chemical shift imaging, as in a modified Dixon method, offers benefits due to its rapid image acquisition, capability for use in breath-holding, and decreased misregistration (17). The cutoff values for diagnosing hepatic steatosis using PDFF are 5% in adults and 6% in children (1718).
T2 or T2* Mapping
T2 or T2* imaging is the most-used hepatic iron quantification method that employs MRI. Iron accelerates T2 relaxation and T2* signal decay due to its paramagnetic properties in the liver. The heterogeneously distributed iron creates focal magnetic field inhomogeneity, which causes precession of protons at different frequencies and results in dephasing and signal decay. The greater the tissue iron levels, the smaller T2 and T2* become (19). R2 or R2* values are preferred because they directly correlate with iron concentrations and increase linearly with iron concentration, as determined by liver biopsy (20). R2* is more often used versus R2, since it can be measured in a single breath-hold and is less sensitive to variations in the size and distribution of iron particles (Fig. 2) (21).
Hepatic iron overload is the abnormal and excessive intracellular accumulation of iron in liver cells and is caused by excess intestinal absorption or repeated blood transfusions. This is problematic because free intracellular iron can cause cellular damage and may lead to fibrosis and cirrhosis in the liver (22). Conditions associated with hepatic iron overload include hereditary hemochromatosis, thalassemia, sickle cell disease, chronic hepatopathy, and transfusional and parenteral iron overload. T2* imaging can accurately measure parameters adequate for both the diagnosis and treatment as well as follow-up of these diseases, even at low iron concentrations (23).
In the case of 1.5T MRI, a T2* value below 16 ms or R2* value over 60 s−1 is accepted as indicating hepatic iron overload, while a T2* value of 4 ms or R2* value of 270 s−1 discriminates moderate to severe hepatic iron overload from absent to mild hepatic iron overload (24). Relaxation rates (R2 and R2*) increase with field strength and liver R2* values measured with 3T were almost double those observed at 1.5T (25). High field strengths may be useful in detecting low degrees of iron overload but may present difficulties in the quantification of heavy iron overload (19).
Mono-, Bi-, and Stretched Exponential Models DWI
DWI quantifies water molecular motion using gradient pulse sequences (26). Usually, a single-shot spin-echo T2-weighted image is used and two symmetric diffusion gradients are applied before and after a 180° refocusing pulse (27). In restricted diffusion, phase shifts of spins after two diffusion gradients occur in the same direction, causing increased signal intensity. In free diffusion, phase shifts of spins will be held in different directions and this could lead to decreased signal intensity after application of two diffusion gradients (28). Conventionally, DWI and apparent diffusion coefficient (ADC) are measured from a mono-exponential model (27).
A bi-exponential model or intravoxel incoherent motion (IVIM) contends that the mono-exponential model is influenced by perfusion-related diffusion and true water molecular diffusion (29). Fast diffusion (D*, pseudo-diffusion), representing relative blood flow, and the perfusion fraction (f), which represents relative blood volume, can be measured from the slope in low b-values. Slow diffusion (D, true diffusion) can be calculated from the slope in high b-values and represents the true water molecular diffusion. However, in an actual environment, proton pools cannot be divided completely, and so the mono- and bi-exponential models can be confounded by a mismatch from the heterogeneous nature of tissues. Therefore, the stretched exponential model was introduced recently to overcome the limitations of previous models (30). It measures the heterogeneity of the diffusion in an environment by measuring the degree of deviation from the mono-exponential behavior (3132). This model is based on the theory that protons show a continuous distribution of diffusions at different diffusion rates without an assumption of tissue compartmentalization (30). From this model, the heterogeneity index (α) and distributed diffusion coefficient (DDC) can be measured. Heterogeneity index (α), which presents values ranging from 0 to 1, represents the deviation of signal intensities from the mono-exponential curve (33). A high α value close to 1 indicates low intravoxel diffusion heterogeneity by approaching mono-exponential decay (30). The DDC represents the mean intravoxel diffusion rate in the presence of heterogeneity.
DWI can be applied in the evaluation of both focal liver lesion and diffuse liver disease in children (2634). The stretched exponential model is an emerging technique, and only a few studies have utilized this model to date for pediatric imaging, such as in the context of brain tumors or body oncology (3536). In adults, the stretched exponential model showed higher diagnostic performance for determining significant hepatic fibrosis than did the mono-exponential model (32).
MR Elastography
MR elastography assesses tissue stiffness by measuring the speed of shear waves propagating within it. When performing MR elastography, special hardware is required. The active driver, which is similar to an audio device, is located outside the scanner room. It delivers vibrational energy to the passive driver (60 Hz for liver MR elastography) through the connecting tube. The passive driver is located near the right anterior abdominal wall and delivers vibrations into the liver. The passive driver must be in contact with the body, and a folded towel is occasionally placed between the driver and child to improve mechanical coupling between the body wall and the driver (37). The driver power is reduced by 20% in pediatric patients (aged 5–18 years) and by 40% to 50% in very young children (younger than two years of age) versus the level in typical adult patients in order to prevent theoretical injuries. For patients aged between two and five, an appropriate intermediate power level can be subjectively selected based on the patient's height, weight, and size (38).
The MR elastography technique can be implemented on conventional 1.5T or 3T scanners, and the measured mechanical properties do not depend on magnetic field strength, since the measured stiffness is contingent upon frequency (39). The response of the tissue to the mechanical stress generated by the vibrations is measured using standard MR phase-contrast imaging sequences with the addition of motion-encoding gradients synchronized with the vibration input. At 1.5T, a 2D GRE sequence is often used, while at 3T, either a 2D GRE or 2D spin-echo echo-planar imaging (EPI) sequence is generally used. Spin-echo EPI MR elastography sequences have been reported to demonstrate fewer artifacts and to generate larger regions of interest in comparison with 2D GRE imaging (4041). These sequences produce wave images, which allow the visualization of the propagating shear waves within the target tissue. Inversion algorithms are applied to the acquired wave images and quantitative maps of tissue stiffness are generated, so-called elastograms (42). Regions of interest are selected, avoiding large blood vessels, to provide an overall estimate of parenchymal stiffness in kPa. MR elastography should ideally be performed after 4–6 hours of fasting. Postprandial status does not significantly change the stiffness of the normal liver, but may cause increased liver stiffness in chronic liver disease because of the transient increase in portal venous flow after meals (43).
MR elastography has been proven to be an accurate method for diagnosing and staging liver fibrosis, albeit mostly in adults (44). In comparison with other methods, liver MR elastography covers much larger volumes of the liver cross-sectionally and provides a global noninvasive assessment of liver parenchyma. Liver MR elastography can be performed in most patients, including those with obesity, anatomical variations, and substantial ascites (37). MR elastography is associated with a high rate of successful examinations in clinical practice, including with a more than 96% success rate in pediatric and young adult patients (45). MR elastography also shows good reproducibility and repeatability with high reliability across vendor platforms, field strengths, and pulse sequences, with an overall intraclass correlation coefficient of more than 0.68 (46).
Dynamic Contrast-Enhanced MRI
DCE MRI involves continuous measurement of the T1 signal intensity of the region before, during, and after the contrast injection (47). For the acquisition of DCE MRI images, three steps are performed as follows: 1) baseline T1 mapping, 2) dynamic data acquisition, and 3) arterial input function (AIF) assessment (4748). For T1 mapping, a fixed T1 value or measured T1 value obtained from variable flip angles, inversion recovery, or the look-locker technique can be used (47). For dynamic data acquisition, short temporal resolutions (about 2–4 seconds) and an adequate spatial resolution (in-plane resolution of 0.5–1.7 mm) are required for quantification (47). After quantification, measurement of AIF is performed to identify the contrast concentration gradient between the intravascular space and extravascular extracellular space (EES) to minimize inflow effects from large vessels (49). Using a semiquantitative model-free method, parameters such as the area under the curve and maximum or relative signal intensities can be quantified from the slope (4750). Quantitative analysis from a pharmacokinetic model, such as the extended Toft's model, has recently been adopted and yields more physiologic, accurate, and reproducible results in comparison with those obtained using the model-free method (48). The extended Toft's model is based on the two-compartment theory, considering the idea that contrast can move between the intravascular plasma space and EES. Using this model, the volume of the plasma compartment (Vp), volume of the extracellular compartment (Ve), volume transfer constant between the plasma and EES (Ktrans), and rate constant (Kep = Ktrans/Ve) can be measured (4750).
Several specific considerations are needed in liver DCE MRI (51), because the liver receives a unique dual supply of blood from the portal vein and hepatic artery. Moreover, the contrast agent can freely pass through plasma and extracellular spaces because of the highly fenestrated endothelial cells in the liver. Previous studies have applied different models for analyzing DCE MRI findings in the liver, but a single method has not been standardized yet for liver application. A dual-input single-compartment model was applied, but it could not reflect the relationship between plasma space and EES (51). A few previous studies have also considered a dual-input two-compartment model using software (5253), but no software considering this model is available at this time from major vendors. Therefore, as an alternative method, a single-input two-compartment model was used in recent investigations by considering that the abdominal aorta could be used as a surrogate input source of the liver (5154).
No study to date has assessed the utility of liver DCE MRI in the pediatric population. This technique is more in the realm of research rather than a clinically accepted technique and the post-processing is not widely available. The performance of DCE MRI is still challenging in the liver and also in children, because accurate T1 mapping, high temporal resolution, the selection of an adequate kinetic model, and reliable reproducible AIF acquisition are necessary. Therefore, the standardization of imaging acquisition and data analysis methods is crucial for stable utilization of DCE MRI in the liver and in pediatric patients.
CT
With the advances in CT technology, DECT can be used for material differentiation and contrast identification. DECT-based multi-material decomposition algorithms generated fat volume fraction images, enabling accurate and reproducible liver fat quantification in an adult study (55). DECT could thus be a less-invasive technique for the assessment of hepatic fat content. However, the radiation exposure associated with CT is still a major limitation in its use in children.
In 2016, Siegel et al. (56) demonstrated reduced radiation exposure in DECT in comparison with estimated single-energy CT levels in children while maintaining a similar contrast profile and contrast-to-noise ratio. Therefore, if used as an optimized study method in appropriate indications, DECT could help in diagnosing liver diseases in children.
Clinical Applications of Quantitative Hepatobiliary Imaging
Biliary Atresia
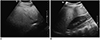
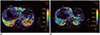
Biliary atresia is a perinatal disease of unclear etiology characterized by inflammatory obstruction of the biliary tress, leading to biliary cirrhosis. US elastography, especially SWE, have been used in the diagnosis of biliary atresia patients since liver SWE values are higher in biliary atresia patients compared to those in other infantile liver diseases (5758). However, one study showed that its diagnostic performance does not exceed that of grayscale US (59). When using MRI, the T2 relaxation time was not different in patients with and without biliary atresia and did not correlate with the stage of hepatic fibrosis in infants with cholestasis (60). However, liver ADC values in biliary atresia patients were lower than those in a control group and had a negative correlation with the degree of liver fibrosis following Kasai operation (6162). On IVIM assessments, hepatic D* values were lower than those in normal children and showed negative correlation with increased liver stiffness (63). Figure 3 shows the utility of mon-, bi-, and stretched exponential models in the liver of a biliary atresia patient. However, there is no published study evaluating the usefulness of bi- or stretched exponential models for the diagnosis and follow-up of biliary atresia patients yet.
Hepatic Fibrosis
US elastography, especially SWE, allows accurate assessment of liver fibrosis with a high success rate, even in children with early stage fibrosis (64). US elastography also showed good performance in diagnosing portal hypertension in children in a systematic review and meta-analysis (65). The summary sensitivity was 90% (95% CI: 83–94%), while specificity was 79% (95% CI: 73–84%). Another study performed only on the subjects of transient elastography also showed good diagnostic performance, with a sensitivity of 95% (95% CI: 74–99%) and a specificity of 90% (95% CI: 81–95%) for the diagnosis of significant liver fibrosis (stage ≥ F2) in children (66). However, the cutoff values for differentiating each fibrosis stage and for diagnosing portal hypertension varied greatly (6566). Optimal cutoff values according to the specific cause of liver disease are yet to be established. As an alternative, additional spleen SWE measurements could be helpful in differentiating portal hypertension in children (Fig. 4) (67). The cutoff value of splenic point SWE for portal hypertension was 3.14 m/s, with a specificity of 98.6% and a sensitivity of 68.2%, even though the diagnostic performance was lower than that for the liver.
One meta-analysis in the adult population had reported the high diagnostic performance of liver MR elastography in staging fibrosis, with an area under the receiver operating characteristic curve of more than 0.88 in patients with significant fibrosis (≥ stage 2), regardless of body mass index and the etiology of chronic liver disease (68). Another adult meta-analysis reported that a measured change of 22% or greater in hepatic stiffness indicated that a true change in stiffness occurred over time with 95% confidence (Fig. 5) (44). MR elastography also has been used in the pediatric population. Xanthakos et al. (69) evaluated 35 patients aged 4–20 years with chronic liver disease, mainly nonalcoholic fatty liver disease (NAFLD), and suggested a cutoff value of 2.71 kPa for significant fibrosis (stages 2–4). There was no difference between liver MR elastography values in patients with and without portal hypertension or gastroesophageal varices, even though spleen MR elastography values were higher with a cutoff value of 9.9 kPa for predicting gastroesophageal varices (Fig. 6) (70). Since there may be confounding factors related to the liver parenchyma in these patients, such as inflammation, the presence of these confounding factors should always be considered prior to interpreting liver MR elastography values.
Nonalcoholic Fatty Liver Disease
NAFLD is a condition that is characterized by the presence of > 5% fat in hepatocytes and is an increasing cause of chronic liver disease in children. If adequate and early precautions are not taken, it can progress to cirrhosis. Quantitative ultrasonographic techniques have been developed to evaluate hepatic fat, including speed of sound estimation, backscatter coefficient, shear wave dispersion, and attenuation parameters (2). A recent study suggested simple grayscale US quantification of a hepatorenal ratio, which was obtained by dividing the mean liver by the mean kidney values using a readily available picture archiving and communication system (Fig. 7) (71). This parameter showed 88.2% sensitivity and 91.4% specificity for predicting hepatic steatosis when using the cutoff value of 1.5 in children. However, other pathologic conditions such as fibrosis and inflammation may intensify liver echogenicity and can result in misinterpretations in this context.
PDFF is known to have high correlation with the histologic grades of hepatic steatosis in adults (r = 0.69–0.74) and also in children (r = 0.73) (272). PDFF has also shown a close agreement with MR spectroscopy values in children (73). Moreover, the radial sampling technique provides an accurate measurement of PDFF in free-breathing status by showing mean differences of less than 0.7% in comparison with PDFF in breath-holding status in children (74). In addition to the diagnosis of hepatic steatosis, PDFF can be used as a tool for the follow-up of hepatic steatosis in children (Fig. 8) (75).
NAFLD patients may show coexisting hepatic iron overload and fat accumulation, and this feature is known to accelerate liver injury (76). In these cases, both detection and quantification of iron and fat can become difficult, especially with conventional MRI. However, the quantification of both iron and fat is still feasible using recent methods that can calculate R2* and PDFF simultaneously (77). This approach can help clarify the coexistence of siderosis and steatosis. In such cases, it is essential to use the multi-peak fat model for accurate quantification of fat (78).
In recent studies with children, liver steatosis and fibrosis showed independent effects on DWI. Bi-exponential model DWI (IVIM) revealed that microvascular perfusion and true water molecular diffusion affected liver steatosis and fibrosis differently (6379). Hepatic fat and blood volume measured by f value showed a positive correlation, while hepatic fibrosis and endovascular blood flow velocity measured by D* showed a negative correlation (63).
These findings are different from those obtained with MR elastography in NAFLD patients. MR elastography performs significantly better in distinguishing stages 0 and 1 versus stage 2 or higher fibrosis in patients without steatosis than in those with steatosis (80). This suggests a confounding effect of steatosis or inflammation in assessments of fibrosis in the population with NAFLD. Moreover, there was a lack of agreement between MR elastography stiffness values and histopathological scores in the presence of moderate to high liver fat in pediatric and young adults (81).
A few recent trials used DCE MRI in animal models for diffuse liver disease, including one that found increased Ktrans in hepatic steatosis and fibrosis in NAFLD (52). However, in another study using a rat liver fibrosis model without the effect of steatosis, Ktrans was negatively correlated with fibrosis stages (53). The utility of DCE MRI in evaluating diffuse hepatic disease in children needs further research.
Hepatic Veno-Occlusive Disease
Sinusoidal obstruction syndrome (SOS) or hepatic veno-occlusive disease (VOD) is a complication that occurs after hematopoietic cell transplantation. It occurs more commonly in children (up to 20%) and demonstrates a high mortality rate (5). Therefore, accurate and early diagnosis of SOS/VOD is clinically important. Even though the diagnosis of SOS/VOD is based on clinical criteria, US imaging findings of both grayscale and Doppler criteria linked to portal hypertension are important in order to successfully differentiate other conditions. Here, the combination of hepatomegaly, ascites, reduced flow in the portal vein measured in the intrahepatic portal vein (threshold of 10 cm/s), elevated resistive index (> 0.8) in the hepatic artery, and reduced but monophasic flow in the right hepatic vein (measured > 80 mm from the inferior vena cava) seem to be the most promising imaging features (Fig. 9) (5). Even though SMI successfully detected differences in flow grades between normal and undescended testes in young children better than conventional power Doppler imaging (4), little is known regarding the utility of SMI for assessing pediatric liver disease at present.
A combination of Doppler US with SWE could assist in the diagnosis and follow-up of SOS/VOD (Fig. 9) (5). Liver shear wave velocity was elevated in an SOS/VOD animal model in proportion to the degree of sinusoidal injury and lobular inflammation (82). This finding might be more sensitive than the conventional Doppler criteria of larger hepatic vessels for the early diagnosis of SOS/VOD. Another study showed that time-intensity curve analysis could provide a more objective approach in the early diagnosis of SOS/VOD (83). CEUS might best reflect pathophysiological changes in SOS/VOD (5).
Hepatic Mass
Previous reports suggested that SWE may help in differentiating malignant from benign focal liver lesions with good intra-observer reproducibility in the adult population (8485). However, SWE has limited application in assessments of pediatric focal liver lesion.
The use of the mono-exponential model DWI is better than T2-weighted images for the detection of focal liver lesions and facilitates differentiation of benign and malignant lesions (2686). In neonates and young infants, hepatic lesions with decreased signal intensity on an ADC map could lead to the diagnosis of hepatoblastoma (Fig. 10) (87). In addition, the differentiation of hepatic adenoma or hepatocellular carcinoma could be aided by DWI as it is in adults (86).
Using DCE MRI in an animal model for the evaluation of liver lesion, Ktrans was shown to increase in hepatocellular carcinoma (88). Our institution uses pediatric liver DCE MRI at 1.5T with a 3D turbo field echo sequence and a temporal resolution of one dynamic per 4 to 5 seconds and 60 dynamics (at least 20 dynamics are required for the analysis). As in our cases, liver DCE MRI could be used for the quantification of liver lesions (Fig. 11) and for the monitoring of treatment response in hepatic tumors (Fig. 12) in serial standardized protocols. However, further validation using this technique is still needed.
CONCLUSION
At this time, we can use variable quantitative imaging techniques to better understand hepatobiliary diseases in children. Specifically, not only MRI but also US can be used to evaluate changes in tissue components, vascularity, and elasticity. We can use these techniques for evaluation of biliary atresia, hepatic fibrosis, NAFLD, SOS/VOD, and hepatic masses in children. Due to the risk of radiation, the effectiveness of DECT for material differentiation has not yet been verified in children. With current and ongoing advances in technology, each imaging technique offers a unique advantage, and the use of the appropriate imaging modality according to a particular disease or patient condition may help to improve diagnosis and treatment by presenting more accurate and objective data in children.









 XML Download
XML Download