

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Achalasia is a rare disorder resulting from the progressive degeneration of ganglion cells in the myenteric plexus of the esophageal wall. This leads to a failure of relaxation of the lower esophageal sphincter, accompanied by a loss of peristalsis in the distal esophagus.1 The recently developed high resolution manometry (HRM) method has allowed a more precise and simple evaluation of the esophageal motility function. After the announcement of the Chicago classification (CC) version 3.0, which is the standard criteria for diagnosing esophageal motility disorders, achalasia and esophagogastric junction outflow obstruction (EGJOO) were classified into different disease categories based on whether or not peristalsis in the esophagus is preserved.2
EGJOO is a distinct motility disorder that encompasses a heterogeneous disease group of underlying etiologies. Moreover, some experts have pointed out that peristalsis is preserved in early stage achalasia and could be diagnosed with EGJOO in HRM.34 This paper reports a case of early stage achalasia that was diagnosed initially as EGJOO using HRM and presented as a subepithelial tumor (SET).
CASE REPORT
A 58-year-old woman visited the Presbyterian Medical Center with symptoms of swallowing difficulty. Her dysphagia was relatively tolerable for solid food, but she could not swallow water at once. When she had two or three sips of water, she experienced dysphagia and complained of chest discomfort. Her symptoms began approximately 20 years ago and occurred about once a week. From the past year, however, her symptoms worsened and occurred at least once a day. Her Eckardt score was six points (dysphagia 2, regurgitation 1, chest pain 2, and weight loss 1). She had a medical history of diabetes and hypertension.
Her initial vital signs were in the normal range, but she had a chronically ill appearance. The physical examination revealed a regular heartbeat without murmur and a clear breathing sound across both lungs. The laboratory tests results were as follows: hemoglobin, 11.2 g/dL; white blood cell count, 6,200/mm3; platelet count, 235,000/mm3; CRP, 1.45 mg/dL; AST, 40 U/L; ALT, 25 U/L; BUN, 9 mg/dL; creatinine, 1.0 mg/dL, sodium, 141 mEq/L; potassium, 3.9 mEq/L; chloride, 100 mEq/L.
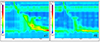
A barium esophagography test was performed initially. This test revealed a dilated esophagus of approximately 3 cm in diameter with pooling and stasis of contrast as well as narrowing of the distal esophageal segment. Uncoordinated tertiary esophageal peristalsis was also observed, but the passage into the stomach was favorable (Fig. 1A). The esophagogastroscopy revealed a tight esophagogastric junction (EGJ), but no abnormal esophageal lesion or food stagnation was observed (Fig. 1B).
HRM revealed a median integrated relaxation pressure (IRP) (4 seconds) of 15.5 mmHg (7.4-24.6) (normal IRP ≤15 mmHg), median distal contractile integral (DCI) of 817 mmHg.s.cm (normal 33%, weak 40%, and failed 27%), and median distal latency of 10.3 seconds (normal range ≥4.5 seconds) (Solar GI HRM; Medical Measurement Systems, Enschede, Netherlands) (Fig. 2 and Table 1). From these results, she was diagnosed with an EGJOO according to the CC version 3.0.
A chest CT scan was performed to exclude the cause of the mechanical obstruction. The CT findings revealed a SET at the upper part of the EGJ, which was estimated to be approximately 20 mm in diameter, and the esophageal lumen was displaced to 2 o'clock due to the SET lesion (Fig. 3). Therefore, surgical treatment was performed for SET lesion, which is believed to be the cause of EGJOO. Eccentric muscular hypertrophy of the distal esophagus (length, 4 cm; thickness, 1 cm) was observed in the surgical field, and the longitudinal myotomy and Dor fundoplication were conducted.
The histopathology examination showed that the normal nerve trunk was destroyed with lymphocyte infiltration, and the muscles of the esophagus were hypertrophied (Fig. 4). The histology findings were consistent with achalasia. Based on these findings, the patient was finally diagnosed with early achalasia. After surgery, barium esophagography revealed normal peristaltic activity and flow (Fig. 5), and her Eckardt score was one point (regurgitation 1), which was much better than that before surgery.
DISCUSSION
The esophagus consists of skeletal muscle in the upper part and smooth muscle in the distal part. Innervation of this muscle is composed of parasympathetic and sympathetic nerves, with peristalsis regulated form the vagus nerve and intrinsic enteric nerve system. Therefore, an imbalance of excitatory and inhibitory nerves can lead to a range of esophageal motor disorders.5 High-resolution esophageal manometry (HREM) is used widely to easily examine the physiological and clinical changes in esophageal motility disorders.
Currently, the CC version 3.0 reported by Kahrilas et al.2 is used widely for diagnosing esophageal motor disorders. In this classification, several pressure topography metrics are introduced to classify esophageal motility disorders. The most important component of a diagnosis of CC, IRP, is calculated as the mean of four seconds of maximal deglutitive relaxation in a 10 second window beginning at the time of upper esophageal sphincter relaxation. An IRP higher than the upper limit of normal indicates impaired swallow-induced lower esophageal sphincter relaxation.
Diseases with a higher IRP than normal include achalasia and EGJOO. According to the CC version 3.0, the definition of achalasia is that the IRP is higher than normal and shows 100% failed peristalsis or spasm, and is classified into three manometric subtypes based on the residual esophageal wave pattern: type I, which is characterized by 100% contractions failure; type II, as pan-esophageal pressurization occurring with at least 20% of swallows; and type III as the presence of at least 20% of swallowing where premature contraction is defined as distal latency <4.5 second.2
Unlike achalasia, EGJOO is diagnosed when intact or weak peristalsis is preserved. In the present patient, although some of the topography showed failed peristalsis, visible peristalsis remained. The patient did not show 100% failed peristalsis, which is an essential condition for the diagnosis of achalasia with the IRP higher than normal; therefore, the authors diagnosed her with EGJOO.
EGJOO and achalasia are divided into different disease categories. EGJOO is a heterogeneous group, including various causes, such as mechanical obstruction, including hiatal hernia, anti-reflux operation, stricture, eosinophilic esophagitis, infiltrative disease, and early expressing achalasia.6 Recently, it has been reported that the lower esophageal sphincter pressure may be increased when taken chronically with opioids and may appear as type III achalasia or EGJOO in these patients.1 On the other hand, although definite achalasia can be shown precisely, the CC 3.0 cannot identify the diverse causes of EGJOO according to the parameters. Therefore, further work-up is needed to find the cause of heterogeneous EGJOO.
Regarding the early phase achalasia as one of the causes of EGJOO, Scherer et al.3 suggested that some cases of functional EGJ obstruction may represent an incomplete achalasia syndrome. In Korea, Shin et al.4 reported a case, in which a patient with EGJOO in the first HRM examination was diagnosed with achalasia on the second HRM, which was performed due to a worsening of the patient's symptoms. Hirano et al.7 reported that the esophageal motility can vary and be heterogeneous depending on how the achalasia syndrome is expressed. While many have a flaccid esophagus, some have spastic contractions of the esophagus as a result of a preserved esophageal longitudinal muscle contraction, and others may have a preserved peristalsis with manometric evidence of outflow obstruction.7 In addition, some studies have reported cases where achalasia progressed gradually from the early stage and showed the characteristics of each subtype. Sodikoff et al.8 reported the histopathological patterns of achalasia subtypes. In this study, there was a similar but more ganglion cell loss in type I than in type II, indicating that type I had progressed from type II.8 Therefore, if achalasia is considered a progressive disease from the early stage, as described above, then early stage achalasia, which still retains peristalsis, can only be diagnosed as EJGOO in a manometry test. Similarly, the present case is believed to be early achalasia expressed as EGJOO, and the ganglion cell loss observed in achalasia appears in the esophagogastric junction, suggesting that the esophageal muscle is hypertrophied asymmetrically.
The general histopathological findings of achalasia revealed an absence of certain nerve cells of the myenteric plexus, lymphocytic infiltration, fibrosis, and most importantly, musculature hypertrophy.89 In a 2003 report by Mittal et al.,10 achalasia patients showed thicker esophageal muscle on the cross section than the normal subject groups. As in the case of the present patients, this muscle hypertrophy can be misdiagnosed as a SET, as with a lesion in imaging studies.
Regarding the treatment of EGJOO, there are pharmacological treatments and endoscopic approaches, such as botulinum toxin injection, balloon dilatation, and myotomy. One study reported that some patients may be subject to spontaneous resolution without treatment, and the factors associated with these results suggest that the typical symptoms of gastroesophageal reflux disease and the resting pressure of the upper esophageal sphincter of less than 50 mmHg are the main components.11
Clinicians should not overlook the fact that EGJOO is just a manometric diagnosis. When patients are diagnosed with EGJOO through manometry, it is important to find the cause of EGJOO to better manage them. In addition, early achalasia can be a cause of EGJOO, and muscle hypertrophy can occur during the progression of achalasia, which can be mistaken for a SET lesion, as in this case.





 XML Download
XML Download