

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cardiac implantable electronic devices (CIEDs) have evolved in technology with increased reliability and safety during the recent years.1) The indications for CIED implantation have been changed based on recent clinical trials, especially in patients with heart failure, in whom implantable cardioverter-defibrillators (ICDs) and cardiac resynchronization therapy (CRT) were recommended for primary prevention of sudden cardiac death and improvement of left ventricular dysfunction.2)3)4) Consequently, CIED implantations have increased dramatically over the past several years.5)6)7)8) Although the use of CIED in western countries has been well described, there is a paucity of information regarding the incidence and temporal trends of CIED treatment in Asian population. Furthermore, with population aging, patients with CIED are becoming older and having more comorbidities.8)9)10) Increasing complexity of baseline characteristics of patients with CIED was closely associated with increased risks of CIED-related complications and worse prognosis.9)10)11) A more comprehensive understanding of CIED epidemiology and its temporal changes is essential to establish appropriate management strategies for patients with CIED in the contemporary era. Therefore, this study aimed to evaluate the temporal trends of the prevalence and incidence of CIED implantations in Korea between 2009 and 2016 by using a Korean nationwide cohort database. In addition, the changes in comorbidities of CIED recipients were assessed.
METHODS
Data sources
The claims database from National Health Insurance Service (NHIS) of Korea was used. The NHIS system is a universal and mandatory health insurance service that provides comprehensive medical care coverage to 97% of the Korean population. The remaining 3% with low income are covered by the Medical Aid program. Since 2006, the information of individuals in the Medical Aid program has been merged into a single NHIS database. Data of all Koreans aged ≥20 years between January 2009 and December 2016 were included. All individuals' demographic information, diagnoses, prescription dispending records, medical device, and procedure codes from inpatient and outpatient services were collected. Diagnoses were coded according to International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM). This study was exempt from review by the Seoul National University Hospital Institutional Review Board (E-1807-033-955) and complied with the Declaration of Helsinki.
Cohort definitions
Between 2009 and 2016, all patients who underwent CIED procedures (new implantation and generator replacement) were identified using procedure codes and their corresponding device codes for claims reimbursement in Korea. The detailed information regarding the procedure definitions are described in Supplementary Table 1.
Indications of cardiac implantable electronic devices implantations
The main indications for CIED implantation were analyzed using ICD-10-CM diagnosis codes. For pacemaker (PM) implantation, patients with atrioventricular conduction disturbance (I441, I442, I443), sick sinus syndrome (I495), and atrial fibrillation with slow ventricular response (I48 without I441, I442, I443, or I495) were identified. For ICD implantation, ventricular tachyarrhythmia (I472), ventricular fibrillation or flutter (I490), and aborted cardiac arrest (I460, I469) were classified as indications for secondary prevention, and other diagnoses were classified as indications for primary prevention. The details of definitions used are described in Supplementary Table 2.
Comorbidities
Baseline characteristics of patients, including age, sex, comorbidities (hypertension, diabetes mellitus, coronary heart disease, peripheral artery disease, and atrial fibrillation, dilated cardiomyopathy, hypertrophic cardiomyopathy) and previous medical history (stroke or transient ischemic attack [TIA], intracranial hemorrhage, myocardial infarction) were obtained. Detailed definitions are presented in Supplementary Table 2. Baseline comorbidities were identified based on the information during the 1-year period preceding the study enrollment.
Statistical analyses
Continuous variables were expressed as means with standard deviations (SDs) and categorical variables were presented as actual numbers and percentages. The incidences of PM, ICD, and CRT devices implantation were determined annually. The annual incidence per 100,000 was calculated as the number of patients with newly implanted CIED divided by the total person at risk among all individuals (age ≥20 years) of that year. Temporal differences in categorical variables were assessed by χ2 tests. Statistical significance was defined by a 2-tailed p value <0.05. Statistical analyses were performed with SAS version 9.3 (SAS Institute, Cary, NC, USA). For times series analysis, autoregressive integrated moving average (ARIMA) model was used with R programming version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org).
RESULTS
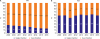
Between 2009 and 2016, a total of 35,421 CIED procedures (27,771 new implantations and 7,650 generator replacements) were performed. The annual number of new implantations and generator replacements of CIED has substantially increased during the study period (Figure 1A and 1B).
 | Figure 1Temporal trends of new implantations (A), generator replacements (B), and annual new implantation rates (per 100,000) of cardiac implantable electronic devices.CRT = cardiac resynchronization therapy; ICD = implantable cardioverter defibrillators; PM = pacemakers.
|
Pacemakers
The mean age for new implantation of PM increased from 68.4±12.3 years in 2009 to 72.0±11.8 years in 2016 (Table 1). The prevalence of hypertension, diabetes mellitus, heart failure, ischemic stroke/TIA, myocardial infarction, and atrial fibrillation has also increased over time. The most common indication for new PM implantation in 2009 was atrioventricular block (55%), followed by sick sinus syndrome (37%), and atrial fibrillation with slow ventricular response (4%), and their proportion remained relatively stable until 2016 (Table 1).
Table 1
Baseline characteristics of patients undergoing new implantation of cardiac implantable electronic device

Values are expressed as mean±standard deviation or number (%).
AF = atrial fibrillation; AVB = atrioventricular block; CAD = coronary artery disease; CRT = cardiac resynchronization therapy; CRT-D = CRT-defibrillator; DCMP = dilated cardiomyopathy; ICD = implantable cardioverter defibrillator; ICH = intracranial hemorrhage; MI = myocardial infarction; SSS = sick sinus syndrome; SVR = slow ventricular response; TIA = transient ischemic attack.
![]()
The number of new implantations of PM doubled during the study period, from 1,977 cases in 2009 to 3,910 cases in 2016 (Figure 1A). Furthermore, the number of generator replacement of PM increased 1.6 times, from 638 cases in 2009 to 1,010 cases in 2016 (Figure 1B). The rate of new PM implantation per 100,000 persons (≥20 years) was 5.1 in 2009 and increased to 9.3 in 2016 (Figure 1C). Notably, the annual increment of new implantation rate was more prominent in the elderly group (Figure 2A). Among patients with the new implantation, the percentage of dual chamber PM has increased from 73.2% to 84.9%, while that of single chamber PM has decreased from 26.8% to 15.1% (p for trend: <0.001, Figure 3A).

Implantable cardioverter defibrillators
During the study period, the mean age of new ICD recipients increased from 53.1±15.1 years to 57.7±15.0 years (Table 1). The prevalence of hypertension, diabetes mellitus, heart failure, coronary artery disease, and atrial fibrillation in these patients also significantly increased. The demographic characteristics of new ICD recipients were different between the primary prevention group and the secondary prevention group (Supplementary Table 3). The primary prevention group was significantly older (60.1±13.7 years vs. 54.4±15.2 years, p<0.001) and had a higher prevalence of hypertension, diabetes mellitus, heart failure, dilated cardiomyopathy, hypertrophic cardiomyopathy, coronary artery disease, myocardial infarction, and atrial fibrillation compared to the secondary prevention group (Supplementary Table 3).
The number of new implantations and replacements of ICD increased 3.6 times (from 230 cases to 822 cases) and 4.3 times (from 48 cases to 204 cases), respectively (Figure 1A and 1B). Among the patients with newly implanted ICD, the proportion of the primary prevention has increased from 18.7% in 2009 to 29.7% in 2016 (p for trend <0.001, Table 1). The rate of new implantation of ICD per 100,000 persons (≥20 years) increased from 0.6 in 2009 to 1.9 in 2016 (Figure 1C). The annual increment of new implantation rate was more prominent in the elderly group (Figure 2B). The patients aged 70–79 years showed the highest new implantation rate of ICD throughout the study period (Figure 2B). The proportions of single and dual chamber ICD remained steady during the study period (dual chamber ICD: 41.7% to 41.6%, p for trend: 0.336, Figure 3B).
Cardiac resynchronization therapy
The age of new CRT devices recipients increased from 64.1±9.8 years in 2009 to 66.9±11.1 years in 2016 (Table 1). The prevalence of hypertension, diabetes mellitus, coronary artery disease, stroke/TIA also increased significantly, while the prevalence of dilated cardiomyopathy remained approximately 70% throughout the study period. Among the patients with newly implanted CRT devices (CRT-pacemaker [CRT-P] and CRT-defibrillator [CRT-D]), the proportion of CRT-D accounted for 72.7% in 2009 and increased to 93.1 in 2016 (p for trend: <0.001, Table 1).
The new implantation of CRT device increased 4.9 times (44 cases to 217 cases), while the replacement rate increased 11.4 times (5 cases to 57 cases) between 2009 and 2016. The rate of new implantation of CRT devices per 100,000 persons (≥20 years) increased 5 times (0.1 to 0.5, Figure 1C). The overall rate of new implantation of CRT increased in those over 60 years, while those aged 70–79 years showed the highest rate of new implantation of CRT (Figure 2C).
Trend forecasting of the new implantations of cardiac implantable electronic devices in Korea
The temporal trends of monthly new implantation number of CIED between 2009 and 2016 and their forecasted numbers to 2022 are depicted in Supplementary Figure 1. For forecasting, ARIMA(3,1,0)(2,1,0)12, ARIMA(3,1,1)(2,0,1)12, and ARIMA(3,1,2)(0,1,1)12 models were constructed for PM, ICD, and CRT devices, respectively. Each model had the best Akaike information criterion value and all models passed the residual test. Although there are some monthly variations, the means of monthly implantation number of PM, ICD, and CRT devices were 166.1, 19.2, and 3.8 in 2009, and increased to 325.8, 68.8, and 18.1 in 2016. In 2022, the monthly implantation number of PM, ICD, and CRT devices are expected to reach approximately 400, 90, and 30, respectively (Supplementary Figure 1). Considering the expected the number of adult population in 2022 (age ≥20 years, n=43,495,386) by the Korean Statistical Geographic Information Service (https://sgis.kostat.go.kr), the new annual implantation rates (per 100,000) of PM, ICD, and CRT devices are expected to be close to 11.0, 2.5, and 0.8 in 2022.
DISCUSSION
To the best of our knowledge, this is the first study reporting the temporal trends of CIED procedure of entire Korean adult population using a nationwide database. The major findings of this study were as follows: 1) the numbers of new implantations and generator replacements of CIED have rapidly increased during the recent 8 years; 2) the new CIED recipients became older and have more comorbidities; 3) the increase of new CIED implantation rate was more prominent in the elderly group. Based on these results and the apparent trend of fast aging in Korean population,12) we expect that the medical expenditure for CIED therapy would increase substantially in the near future.
Although we found that the CIED implantation in Korea has increased over the last 8 years, this implantation rate is still quite low compared to other countries. In the US, the implantation rate of PM per 100,000 persons increased from 47.6 in 1993 to 61.6 cases in 2009.8) Especially, the ICD implantation rate increased dramatically from 6.1 to 46.2 cases per 100,000 persons from 1993 to 2006.9) In Western Europe, the PM implantation rate increased from 82.9 to 93.8 cases per 100,000 persons, and the CRT devices implantation rate increased from 6.0 to 14.0 cases per 100,000 persons between 2005 and 2011.3) However, more recently the implantation of PM and ICD is no longer increasing in some countries. According to a survey in 2015, the PM implantation rate per 100,000 persons decreased from 106.4 to 102.6 during the period of 2010 to 2014 in Western Europe. The ICD new implantation rate also decreased from 26.2 to 25.5. Only the CRT implantation rate (per 100,000 persons) increased from 15.0 to 19.7 during that period.13) In Japan, the implantation rate of PM (per 100,000 persons) increased from 21.0 in 2001 to 27.2 cases in 2009, while the ICD implantation rate increased from 0.9 in 2001 to 4.2 cases per 100,000 persons in 2009.5)14) Therefore, the PM implantation rate of Korea was one-fifth of that of Japan (5.1 vs. 27.2 in 2009) and one-twentieth of that of Western Europe countries (5.4 vs. 106.4 in 2010) during the period of 2009 to 2010. Furthermore, the ICD implantation rate of Japan and Western Europe were 7 times (0.6 vs. 4.2 in 2009) and 37 times (0.7 vs. 26.2 in 2010) higher than that of Korea during the period of 2009 to 2010.
Several randomized control trials demonstrated the survival benefit of CRT and ICD (primary prevention) in select patients with heart failure.15)16)17) Based on these trials, global guidelines strongly recommend the ICD and CRT implantation in whom met the guideline criteria.4)18)19)20) However, adherence with the guidelines seems to be unsatisfactory in clinical practice of heart failure device therapy even in advanced countries.17) According to the surveys in late 2000s, only approximately 35–50% of patients with heart failure who were eligible for ICD and CRT eventually received the device therapy in US.21)22) In a report from Sweden which shows the average implantation rates of ICD and CRT in Europe, they reported the acceptable awareness rate of ICD indication was only 61% even in cardiologists.23) In Japan, only 44% of eligible patients for class I indication of primary prevention received ICD therapy.24) They pointed out the low referral rate from primary physician to general cardiologist and from general cardiologist to electrophysiologist as one of the main reasons for the underuse of the ICD. Considering that Korea has a similar prevalence of heart failure to that of other countries including Japan,25)26) we believe the ICD and CRT devices therapy are apparently being underused in Korean heart failure patients. The risk of sudden cardiac death of Korean patients with heart failure was not lower than that in patients enrolled in Western population studies.27) Korean patients with heart failure who met the criteria of ICD implantation for primary prevention showed comparable rates of all-caused death and risk of sudden cardiac death to those of patients in the MADIT-II and DEFINITE standard therapy groups.27)
Additionally, reimbursement criteria were also one of the barriers of low implantation rate in Korea. Recently, the Korean reimbursement criteria for primary prevention ICD therapy have been expanded close to those recommended by the global guideline; therefore, the primary prevention ICD implantation is expected to increase in near future. Furthermore, the change of temporal trends of ICD and CRT devices implantation in Korea reflects the improved awareness of physicians for the benefits of device therapy in patients with heart failure. The education of referring physicians to improve their awareness for device therapy would be a reasonable strategy to improve the underutilization of ICD and CRT devices in Korea.
In present study, the ratio of single-chamber to dual-chamber ICDs did not change significantly from 2009 to 2016. Theoretically, dual-chamber ICD may offer benefits, such as better rhythm discrimination, reduction in inappropriate shocks, and probability of reducing the rate of hospitalization. However, these potential benefits were not confirmed by randomized clinical trials. The benefits of reducing inappropriate therapy in dual chamber device is not very clear over single chamber device for primary and secondary prevention.28)29)30) Recent study reported that dual-chamber ICD showed an increased risk of periprocedural complications and generator replacement, whereas the risk of inappropriate shock is similar to the single-chamber ICD.31) There are huge geographical variations on device selection of single- or dual-chamber ICD.32) Interestingly, the ratio of single-chamber to dual-chamber ICDs (6:4) in Korea is similar to that in German and Belgium.32)
There are overlaps between the guidelines indications for CRT and ICD implantation for primary prevention.2)3)20) In reimbursement criteria of Korea, most of patients who are indicated for CRT implantation were also indicated for ICD implantation. Thus CRT-D has been used overwhelmingly over CRT-P in Korea.33)34) The ratio of CRT-P and CRT-D in the present study was 1:2.7 in 2009 then increased to 1:13.3 in 2016. Although the evidences supporting CRT-D over CRT-P is weak in CRT eligible patients,35)36) we assumed that the reimbursement criteria of CRT might affect the device selection in Korea. In the US, the share of CRT-P has increased from 12% in 2008 to 20% in 2013.35) While in the Europe, the average ratio of CRT-P/CRT-D is 1:2.7 in 2015 though there are huge geographic differences (1:1.3 in United Kingdom and 1:5.0 in German).13) Although the recommendations of American and European guidelines for CRT are similar, there are different pattern of selecting CRT device.
Using national data that includes the entire Korean population is a major strength of the present study. All reimbursement claim data were searched; therefore, we think that the present study reflects the real-world practice pattern accurately. However, several limitations of this study should be acknowledged. First, detailed medical information of patients was not available in the NHIS database. Second, patients with implanted CIED before the study period who did not need generator replacement within the study period could not be included in this study. We could access only the procedure codes and device codes that were reimbursed during the study period. Therefore, only the data of patients with new implantation or generator replacement could be analyzed, and the annual prevalence of total CIED population could not be assessed. Finally, the ARIMA forecasting model is based on a pre-assumed linear form of the associated time series. The expected monthly implantation numbers were calculated based on the previous increasing trends and the seasonal variations. The forecasted values could be less accurate when the age distribution of the whole population changes significantly. Thus, relatively short-term periods were forecasted in this study.
As Korean population ages, the CIED implantations have been dramatically increased during the past 8 years. Consequently, higher economic burden for device therapy are expected in the future. Meanwhile, compared to other advanced countries including Japan, the new implantation rate of CIED is still low, especially in ICD and CRT. Deliberate strategies to improve underutilization of ICD and CRT are required to improve heart failure care in Korea.
 XML Download
XML Download