

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hypertension is a major independent risk factor for the development of cardiovascular disease (CVD) including cardiac death, coronary heart disease (CHD), heart failure (HF), and stroke, thus early diagnosis, prevention and optimal management of hypertension is very important for the cardiovascular health.1)2) Recently published global hypertension guidelines aim to achieve earlier and lower blood pressure (BP) control throughout 24 hours.3)4) Since the awareness, treatment and control rates of hypertension are stationary worldwide,1)2)5) there are many unsolved issues and unmet medical needs for the proper control of hypertension. Because of lack of awareness with white-coat, masked, morning and nocturnal hypertension,6)7) patients used to measure their BP only at clinic. Recent analyses revealed nighttime BP is a stronger risk factor for CHD and stroke than clinic or daytime BP, and non-dipping pattern has been associated with an increased risk for CVD events and all-cause mortality.7)8)9)10)11) Therefore, out-of-office BP measurements through ambulatory BP monitoring (ABPM) or home BP monitoring provides better prognostic information than office BP alone.12)13)14) It is very important to understand the pathophysiology, clinical significance and therapeutic implication of nocturnal hypertension.
CIRCADIAN BP VARIATION AND NOCTURNAL HYPERTENSION
Circadian rhythm is associated with intrinsic factors (sympathetic nervous system and renin-angiotensin system) or extrinsic factors (physical activity, dietary sodium, alcohol, smoking, behavioral factors).15) As a normal physiologic change, BP and pulse rate are high in the waking hours and lower during sleep, the average BP at night decreases by 10–20% from daytime BP (dipper).16) A nighttime BP decrease of 20% or more (extreme dipper) may be associated with increased risk for ischemic stroke and silent cerebral diseases.17) Meanwhile, a difference of less than 10% (non-dipper) or an increase in the nighttime BP relative to the daytime BP (reverse dipper or riser) is also associated increased risk of death, myocardial infarction, and stroke16)17)18)19)20) and both non-dipping patterns may cause nocturnal hypertension (Figure 1).
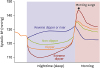 | Figure 1Four different dipping patterns of nocturnal BP and morning BP surge. Both nocturnal hypertension and morning hypertension are the new targets for the perfect 24-hour BP control for the prevention of target organ damage and cardiovascular events (modified from Kario K. Nocturnal hypertension: new technology and evidence. Hypertension 2018;71:997-100911)).BP = blood pressure.
|
Nocturnal BP, a night-to-day ratio of BP level and non-dipping patterns obtained by ABPM are stronger predictors of cardiovascular outcomes and/or target organ damages than daytime ambulatory BP. The outcome-driven threshold for nocturnal hypertension by ABPM has been reported to be BP ≥120/70 mmHg at night which corresponds to a clinic BP ≥140/90 mmHg. According to the latest 2017 American College of Cardiology/American Heart Association Hypertension Guideline, nocturnal hypertension is defined as a BP ≥110/65 mmHg by ABPM (lowered from the previous value of ≥120/70 mmHg). On the other hand, the 2018 European Society of Cardiology/European Society of Hypertension Guideline and the 2018 Korean Society of Hypertension Guideline21) maintained the criteria for nocturnal hypertension as systolic BP ≥120 mmHg and/or diastolic BP ≥70 mmHg at night.
The nocturnal hypertension is more important in Asian population because of higher salt intake and higher salt sensitivity. Moreover, masked hypertension and nocturnal hypertension is more common in Asian populations.22) According to the unpublished Korean ambulatory BP (KorABP) registry (n=3,745), prevalence of the masked hypertension and nocturnal hypertension in patients with well-controlled clinic BP was 47.4% and 59.4% respectively irrespective of antihypertensive treatment. These findings may be explained partly by the dipping patterns observed in this registry — dipper (35.7%), non-dipper (37.5%), extreme dipper (9.5%) and reverse dipper or riser (17.3%). In prior studies, more than 40% of all black and 20% of all white adults have had nocturnal hypertension.23)24) Among the Coronary Artery Risk Development in Young Adult study and Jackson Heart Study participants, prevalence of nocturnal hypertension was 41.1% and 56.9% and non-dippers were 32.4% and 72.8%, respectively.25) A Spanish ABPM Registry study of untreated (n=37,096) and treated hypertensive patients (n=62,788) reported that prevalence of the nocturnal hypertension was 40.9% in the untreated and 49.8% in the treated group.26) In addition, an international ABPM registry study demonstrated that nocturnal BP fall was smaller in Asians than in Europeans.27) Therefore, isolated nocturnal hypertension defined as a nighttime BP of ≥120 mmHg systolic or 70 mmHg diastolic and a daytime BP <135/85 mmHg) is more common in Asians (Chinese 10.9%, Japanese 10.5%) than Europeans (Eastern 7.9%, Western 6.0%, Northern 3.6%),20) but not in Koreans (3.9%) from the KorABP registry which needs further studies. Nocturnal hypertension and nocturnal non-dipping are considered as separate entities, however both of them are associated with target organ damage and poor cardiovascular outcomes, either separately or synergistically.
Despite the major advantage of ABPM which has been indicated as the gold standard for out-of-office BP measurement especially to evaluate the circadian rhythm of BP, nighttime BP recordings may interfere with sleep quality and it results inaccurate nocturnal BP measurement and lack of reproducibility. Recent technological advances in self-monitoring devices enabled to develop several kinds of home measurement devices for nocturnal BP — upper arm cuff oscillometric home BP devices (Omron HEM-747IC-N/HEM-5041/HEM-7252G-HP/HEM-5001[Medinote], Microlife WatchBP Home N)28)29)30)31)32)33) and wearable wrist-cuff oscillometric BP measurement devices (Omron HeartGuide).34) Recent guidelines recommend the use of a validated upper arm cuff oscillometric devices for home BP measurement because it is generally well aligned with the heart level. A recent meta-analysis revealed that the nocturnal home BP and ambulatory BP measurements provide similar values (home BP were 1.4 mmHg higher for systolic [95% confidence intervals {CIs}, 0.3 to 2.6 mmHg] and 0.2mmHg lower for diastolic values [95% CIs, −0.9 to 0.6 mmHg]) in comparison with ambulatory BP measurements.35) Currently, several wearable cuffless BP monitors are under developing to minimize the hazardous effects of cuff inflation and disturbance of sleep quality such as a wearable cuffless BP monitor using pulse transit time (SeismoWatch)36) and wearable surge BP monitoring of wrist-type tonometry (Omron WSP).11) Although BP measurement algorithm and accuracy of BP monitoring is not released yet, a new smartwatch (Samsung Galaxy Active) which will use an optical sensor to read BP using a technique called photoplethysmography, is hopefully supposed to monitor 24-hour BP continuously and can analyze the circadian BP rhythm and nocturnal BP level through My BP Lab app which is jointly developed with University of California, San Francisco.37)
CHARACTERISTICS OF NOCTURNAL HYPERTENSION
Although health behaviors predicting nocturnal hypertension are less clear, non-dipping patterns of nocturnal BP has been associated with several conditions or factors which disrupt the circadian rhythm. Possible mechanisms of nocturnal hypertension are volume overload condition, autonomic dysfunction, sleep disturbances, treated or untreated hypertension, and other lifestyle-related factors (Table 1).15)38)39)40) In salt-sensitive blacks and Asians, the diminished nocturnal BP fall can be restored and the circadian rhythm of BP shifts from the non-dipper pattern to the dipper pattern by salt restriction. Non-dippers were more prevalent in patients with chronic kidney disease (CKD). Wang et al.41) reported 21.9% were riser, 36.1% were dipper, and 42% of CKD patients were non-dipper, and Liu et al.42) found that non-dipping phenomenon was commonly found in patients undergoing hemodialysis with the prevalence up to 70%. Taken together, limited sodium metabolism and imbalance of nocturnal autonomic nervous system activation especially sustained sympathetic activation is considered as the causes of nocturnal hypertension and attenuated nighttime BP decline. However, as stated previously, the prevalence of isolated nocturnal hypertension shows prominent across-ethnicity difference, nocturnal hypertension might be a distinct clinical entity driven either by the inherited genes or by health behaviors or a gene-environment interaction.
Table 1
Factors and associated conditions responsible for the nocturnal hypertension or non-dipping patterns of nighttime blood pressure

![]()
Nighttime blood pressure and quality of sleep
The cardiovascular system is markedly affected by normal sleep with differential autonomic regulation during the different sleep stages.43)44) Because of parasympathetic predominance during non-rapid eye movement sleep, nocturnal dipping pattern of BP and heart rate occurs physiologically. However, sympathetic activity increases significantly and is highly variable during rapid eye movement sleep, nighttime BP is highly variable and sometimes elevates up to awake BP levels.45) Therefore, the regulation of nocturnal BP is tightly linked to sleep patterns. Any disturbance in sleep quantity or quality may contribute to the development of daytime or nocturnal hypertension or an increase in its severity, and it is associated with obesity, metabolic syndrome and glucose metabolism.
Obstructive sleep apnea (OSA)-related hypertension is predominately represented as a diastolic or nocturnal hypertension and is frequently accompanied with masked hypertension and non-dipper status.45)46) The average peak and the maximal nocturnal BP values may be related to the nocturnal BP surge triggered by the apnea or hypopnea episodes of OSA.47) According to meta-analyses derived from 19 randomized controlled trials have demonstrated that continuous positive airway pressure, the first-line therapy for moderate to severe OSA syndrome, reduces the 24-hour mean BP by approximately 2 mmHg (pooled estimated effect).48)49) Active or supportive measures to increase quality or quantity of sleep are advised to the patients with nocturnal hypertension with sleep disorders.
CLINICAL SIGNIFICANCE OF NOCTURNAL HYPERTENSION
Many retrospective studies have been conducted to identify the effect of nocturnal hypertension and non-dipping patterns on its clinical implications. Nocturnal hypertension is a risk factor for target organ damage for the brain, heart, kidney, and large and small arteries and for all CVD events including both hemorrhagic and ischemic stroke, CHD, HF (especially with HF with preserved ejection fraction), CKD, and sudden cardiac death, independently of clinic BP, in general populations and hypertensive patients.6)20)50)51) In the PAMELA study, the risk of cardiovascular death for each 10 mmHg increase of systolic BP progressively increased from office to home, day, 24-hour to night BP values.52) The International Database of Ambulatory blood pressure in relation to Cardiovascular Outcome (n=8,711) reported that nocturnal hypertension was associated with a higher risk of total mortality and all cardiovascular events.9) In a recent meta-analysis, nocturnal home and ambulatory BP measurements were found to be similarly associated with hard cardiovascular outcomes and indices of target organ damages, i.e., left ventricular mass index and carotid intima-media thickness.8) Moreover, not only thickening of carotid intima but also formation of atheromatous plaque were more frequently observed in uncontrolled non-dipping hypertensive patients than in dippers.53) Although clinic, home and/or daytime ambulatory BP are well controlled, masked uncontrolled nocturnal hypertension was associated with increases in arterial stiffness, the plasma BNP level and the urinary albumin/excretion ratio, suggesting that nocturnal hypertension is an independent risk for future CVD events.50)54)55) In addition to progression of CVD in non-dippers, cerebrovascular events such as intracerebral hemorrhage or silent cerebral infarct are more common in nocturnal hypertension and subsequent brain atrophy and lacunar infarcts may leads to memory impairments, physical and cognitive dysfunction especially in elderly people.56) Therefore, the nocturnal hypertension is the very important therapeutic target to prevent target organ damage and cardiovascular events in patients with hypertension.
THERAPEUTIC IMPLICATION OF NOCTURNAL HYPERTENSION
Although it is still unclear whether normalizing nocturnal BP or restoring the abnormal BP dipping pattern to normal pattern would improve prognosis, few studies were positive in this regards. In the Heart Outcomes Prevention Evaluation study, cardiovascular outcome was significant reduced in ramipril-treated high risk patients (relative risk, 0.68–0.80; p<0.001) in spite of modest decrease of office BP (−3/−2 mmHg).57) Small ABPM sub-study provides a clue for the explanation because nocturnal systolic and diastolic BP was markedly reduced by 17 mmHg and 8 mmHg respectively in the ramipril-treated patients and furthermore bedtime administration of ramipril could reduce nocturnal BP more efficiently than morning dosing.58) Other similar evidence was provided by the BP-lowering arm of the ABPM sub-study of Anglo-Scandinavian cardiac outcomes trial. Recent study suggested that a 5 mmHg reduction in nocturnal systolic BP by ABPM was associated with a 17% reduction in cardiovascular events (p<0.001), independent of changes in any other ambulatory BP parameters.59)
The initial step for treatment of nocturnal hypertension would be a pathophysiology-based management because there is no evidence-based treatment approaches so far. Since the circulating volume overload may contribute to nocturnal hypertension and non-dipping patterns, lifestyle modification with salt restriction and thiazide diuretics inducing natriuresis may reduce nighttime BP preferentially and also restore abnormal nocturnal BP variation.60)61)62) For the modulation of autonomic dysfunction, there is one positive report in reducing nocturnal BP with nighttime dosing with α-blocker doxazosin in uncomplicated hypertensive patients.63) Several new strategies to manipulate autonomic function such as baroreflex activation therapy needs more evidence.64) Renal denervation also significantly reduced nocturnal BP, indicating that sympathetic nervous activity may partly determine nocturnal BP by reducing sodium excretion and increasing peripheral vascular resistance.64)65)66) Active or supportive measures to increase quality or quantity of sleep and psychological consultation or proper management of neurologic diseases are also necessary in patients with nocturnal hypertension if they have specific diseases.
Generally, a long-acting antihypertensive drug is used as an initial treatment of hypertension with or without nocturnal hypertension in order to control 24-hour BP and to increase adherence. However, almost all currently available antihypertensive drugs used once daily are rarely effective for all day long. Chronotherapy, the scheduled administration of pharmaceutical agents with respect to an individual's circadian rhythm, may enhance drug effectiveness and tolerance.66)67)68)69)70)71)72) The Ambulatory Blood Pressure Monitoring and Cardiovascular Events study, which included 2,156 hypertensive adults with a median follow-up of 5.6 years, revealed that the administration of at least one antihypertensive drug at bedtime has been reported to be more effective than morning dosing, not only at lowering nocturnal BP and restoring circadian variability in BP, but also for reducing cardiovascular events and total mortality.67)69) The use of chronotherapy with angiotensin-receptor blocker (ARB; telmisartan, olmesartan, valsartan), ramipril, or calcium-channel blocker (amlodipine, nifedipine gastrointestinal therapeutic system) had shown similar beneficial effects in reducing prevalence of non-dippers and improving nocturnal BP fall more significantly than morning administration without loss of daytime BP control.58)59)70)71)72) In addition, a chronotherapy trial using combination antihypertensive drug (valsartan/amlodipine) revealed that BP control was better when treated both at bedtime than both in the morning or one morning and the other at bedtime.31)73) In patients with resistant hypertension, chronotherapy can also improve BP control and revert the non-dipper pattern.74) In addition, the SYMPLICITY HTN-3 trial demonstrated that renal denervation reduces the nighttime systolic BP very effectively in patients with OSA and resistant hypertension suggesting renal denervation is expected to be one modality in treating patients with nocturnal hypertension.66)
In patients with diabetes and uncontrolled nocturnal hypertension, empagliflozin and ARB combination therapy showed significant reduction of not only nighttime BP but daytime BP compare to ARB only group.75) An earlier 2016 American Diabetes Association (ADA) statement notes evidence that taking at least 1 antihypertensive medication at bedtime may significantly reduce cardiovascular events.76) However, the latest 2019 ADA statement, while recognizing the impact of nocturnal hypertension, does not make a clear directive for bedtime drug administration.77) Likewise, recent global hypertension guidelines do not make any specific recommendation on nighttime BP medication dosing to alleviate nocturnal BP elevation.3)4)21)
There are several already finished, on-going, or planned clinical trials to investigate the advantages of chronotherapy with ARBs in patients with CKD with or without maintenance hemodialysis, and to evaluate possible repositioning effects of new drugs such as sodium-glucose co-transporter 2 inhibitor (empagliflozin) or ARB-neprilysin inhibitor (valsartan/sacubitril) on preventing HF in patients with nocturnal hypertension.78)79)80)
CONCLUSIONS AND PERSPECTIVES
Nocturnal hypertension and abnormal nighttime BP dipping status, either alone or together, is believed as stronger risk factors for target organ damage and cardiovascular outcome in both population and hypertensive patients, suggesting that nocturnal BP is worth monitoring in addition to clinic and home BP to detect the residual cardiovascular risk. Since out-of-office BP measurement is essential to evaluate diurnal BP rhythm and nocturnal BP level, simple, accurate, reproducible and sleep non-disturbing ambulatory or self-measuring home BP measurement devices are necessary to provide nocturnal hypertension as a new therapeutic target in the management of hypertension.
Further prospective studies are needed to identify useful diagnostic or prognostic markers of nocturnal hypertension, to demonstrate clinical benefits of lowering nocturnal BP and restoring abnormal BP variations, to investigate the most effective therapeutic strategy for nocturnal hypertension, and finally to determine whether the reduction in cardiovascular events by the nocturnal BP-guided approach exceeds to current guideline-directed management alone.
 XML Download
XML Download