

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hyperbaric oxygen (HBO) therapy, which involves high-pressure oxygen, has been applied for medical purposes [12]. The mechanism of HBO therapy follows the simple law that oxygen dissolves in solution in a direct proportion to its partial pressure [3]. The principal effect of HBO is to increase the oxygen concentration in tissues by increasing the amount of oxygen dissolved in blood plasma. HBO therapy could help in the wound healing phase [34]. HBO has also been found to play a role in bone healing. In previous studies of rabbit, osteoid formation in the HBO group was faster than in the non-HBO group (NHBO group) [56]. In other studies of rat calvarial defects, it was found that HBO was effective in stimulating vascularization and bone formation [78]. After a 4-week healing period in rat calvarial defects, the possibility of a synergistic effect of HBO on new bone formation and angiogenesis was proposed [8]. This possible synergistic effect has not yet been evaluated after a longer healing period with the same study design. In most clinical cases, HBO is applied to improve the speed and/or quality of healing in tissue with impaired healing capacity caused by radiotherapy or systemic disease [34]. HBO could also improve bone regenerative capacity in normal tissue without any impairment of healing. However, the effects of HBO remain controversial [4].
Biphasic calcium phosphate (BCP) is a synthetic bone graft material that simulates the inorganic phase of human bone tissue. BCP is composed of hydroxyapatite (HA) and beta-tricalcium phosphate (β-TCP). HA is insoluble, allowing it to prevent collapse of the augmented area and maintain the integrity of the grafted space throughout the entire healing period for new bone formation. In contrast, β-TCP is resorbed more quickly than HA and it degrades into calcium and phosphate ions. The dissolved space is replaced by newly formed tissue [910]. By applying BCP, it is possible to achieve ideal space maintenance by HA and ideal material degradation by β-TCP. The osteoconductive characteristics of BCP have been well documented in previous studies [11]. However, the osteoinductive characteristics of BCP have rarely been investigated because the main role of this synthetic bone graft material is to maintain space for other tissues to grow into.
In order to improve the osteoinductive characteristics of BCP, various surface modifications have been devised. Escherichia coli-derived recombinant human bone morphogenetic protein-2 (ErhBMP-2) can be used to modify the surface of BCP. Enhancement of new bone formation was confirmed after applying ErhBMP-2 to the surface of BCP [1213]. However, several side effects of bone morphogenetic protein-2 (BMP-2) are still concerning, such as the formation of an ectopic bone void and soft-tissue swelling, which could be life-threatening in some conditions [141516]. Therefore, it is recommended not to use BMP-2 at high concentrations [12]. Slow release of BMP-2 through a proper carrier or coating process is also required to minimize possible clinical complications. Epigallocatechin-3-gallate (EGCG), which is the most abundant catechin in green tea, can be used to modify the surface of BCP [13]. EGCG is known to induce apoptosis of osteoclasts and to inhibit osteoclast formation. Side effects of EGCG have been reported infrequently [1718]. In the present study, ErhBMP-2 and EGCG were used for surface modification of BCP to minimize possible clinical complications and to investigate the possibility of a synergistic effect on the enhancement of osteogenic potential. In addition, the synergistic effect of HBO was investigated.
The purpose of this study was to evaluate the synergistic effect of adjunctive HBO therapy on new bone formation and angiogenesis after 8 weeks of healing.
MATERIALS AND METHODS
Study design and animals
This study included 28 male Sprague-Dawley rats. The body weight of the rats was from 250 to 300 g. They were maintained in cages with free access to standard laboratory food pellets and water. An ambient temperature of 21°C was maintained. All research procedures, including animal selection, the surgical protocol, and management were approved by the Institutional Animal Care and Use committee of Yonsei Medical Center, Seoul, Korea (2013-0295-1). The animals were split into 2 groups (HBO [n=14] and NHBO [n=14] groups), which were then subdivided into BCP and ErhBMP-2-/EGCG-coated BCP (mBCP) subgroups according to the type of applied bone graft material.
Preparation of BCP and mBCP
The bone graft material used for the BCP group in this study was BCP (OSTEON, Genoss, Seoul, Korea). The ratio of β-TCP to HA was 3:7. The bone graft material used for the mBCP group was prepared with a coating procedure on BCP, for which ErhBMP-2 (0.05 mg/mL, Cowellmedi, Busan, Korea) and EGCG (5 mg/mL, purity >90%, Sigma-Aldrich, Ishikari, Hokkaido, Japan) was used [1317]. The process was conducted as follows [1920]: 1) the hydroxide ion of HA was combined with the silane coupling agent (3-aminopropyltriethoxysilane, Sigma-Aldrich), 2) amino radicals were combined with a bifunctional cross-linker (N-succinimidyl-3-maleimidopropionate [SMP], Sigma-Aldrich), 3) SMP was combined with ErhBMP-2 and EGCG, 4) lyophilization was performed, 5) the material was dried (2 hours in a pressure chamber at 7–10 mTorr and more than 2 hours at −20 to 20°C), and 6) sterilization was performed using ethylene oxide.
Surgical procedures and HBO therapy
All surgical procedures were completed under general anesthesia (intramuscular injection with Zoletil [30 mg/kg] and Rompun [10 mg/kg]) and local anesthesia (infiltration with 2% lidocaine with 1:100,000 epinephrine). The surgical site was shaved, isolated, and sterilized with povidone-iodine solution. Two bilateral identical calvarial defects with a 6-mm diameter were created in the parietal bone in each animal. One defect was grafted and the other was not grafted. BCP was applied to the BCP subgroup, and mBCP was applied to the mBCP subgroup. The surgical sites were sutured with 4-0 polyglactin 910 suture material (Vicryl, Ethicon, Somerville, NJ, USA). Two-week adjunctive HBO therapy (1 hour, 5 times a week) in a high-pressure oxygen chamber (2.4 atm) was administered to the animals in the HBO group.
Histologic analysis
The animals were euthanized (CO2 asphyxiation) at 8 weeks after surgery. The samples including calvarial bones were fixed, decalcified, and embedded in paraffin. Specimens were stained with hematoxylin/eosin for the histologic evaluation. The sections were examined at ×12.5 magnification. New bone area and soft tissue area were measured by TOMORO ScopeEye 3.6. New bone (%) was calculated as follows (Figure 1):
 | Figure 1Method of measuring new bone, graft particles, and soft tissue area. Each slide was painted using Photoshop. The number of pixels corresponding to new bone, graft particles, and soft tissue in each image of a calvarial defect was quantified (ScopeEye 3.6, TOMORO, Samkyung, Seoul, Korea). New bone: navy blue color; graft particles: orange color; soft tissue: green color.
|
Microvessels and vascular endothelial growth factor (VEGF) were detected by immunohistochemical staining (endothelial cell adhesion molecule-1 [CD31] monoclonal antibodies). The sections were then incubated with immunoglobulin antibody (Dako, Glostrup, Denmark) for 30 minutes. The sections were rinsed in Tris-buffered saline and incubated at room temperature for 30 minutes. After staining with diaminobenzidine, the distribution and localization of the stained endothelial cells in the defect were confirmed with an optical microscope (×200 magnification). Blood vessel count (%) and VEGF staining (%) were quantitatively assessed.
Statistical analysis
The statistical analysis was performed with descriptive data (mean±standard deviation) using SPSS version 20.0 (IBM Corp., Armonk, NY, USA). Differences between the NHBO and HBO groups, as well as differences within each group according to the graft material, were compared with the Mann-Whitney U test. The level of statistical significance was set at P<0.05.
RESULTS
Histologic evaluation
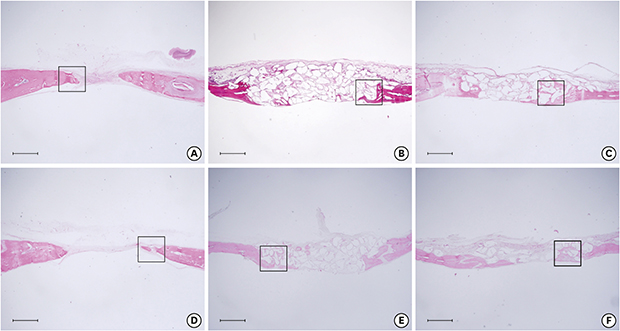
After the 8-week healing period, complete defect closure was observed in all the study groups (Figure 2B, C, E, and F). Overall, in the HBO groups (Figure 2D-F), the defects shrunk more in height, and more bone graft material was resorbed than in the NHBO groups. More new bone formation and blood vessels were found in the HBO-control group (Figure 3D) than in the NHBO-control group (Figure 3A). More matured new bone was found in the HBO-BCP group (Figure 3E) than in the NHBO-BCP group (Figure 3B). More matured, interconnected new bone was also found in the HBO-mBCP group (Figure 3F) than in the NHBO-mBCP group (Figure 3C).
 | Figure 2Histologic evaluation (hematoxylin and eosin staining). (A) NHBO-control group, (B) NHBO-BCP group, (C) NHBO-mBCP group, (D) HBO-control group, (E) HBO-BCP group, (F) HBO-mBCP group. The area of interest close to the defect margin was designated with a rectangle on each slide.HBO: hyperbaric oxygen, NHBO: non-hyperbaric oxygen, BCP: biphasic calcium phosphate, mBCP: Escherichia coli-derived recombinant human bone morphogenetic protein-2-/epigallocatechin-3-gallate-coated biphasic calcium phosphate.
|
 | Figure 3Histologic slides (hematoxylin and eosin staining) of the area of interest. (A) NHBO-control group, (B) NHBO-BCP group, (C) NHBO-mBCP group, (D) HBO-control group, (E) HBO-BCP group, (F) HBO-mBCP group. Red dotted line: defect martin; arrow head: new bone; arrow: residual material; asterisk: connective tissue and blood vessel.HBO: hyperbaric oxygen, NHBO: non-hyperbaric oxygen, BCP: biphasic calcium phosphate, mBCP: Escherichia coli-derived recombinant human bone morphogenetic protein-2-/epigallocatechin-3-gallate-coated biphasic calcium phosphate.
|
Histometric analysis
More new bone (%) was found in the NHBO-mBCP group than in the NHBO-BCP group and the NHBO-control group (P<0.05). A significant difference in new bone formation (%) between the HBO-mBCP and HBO-BCP groups was not found. A significant difference in new bone formation (%) between the HBO and NHBO groups was not found either.
A higher blood vessel count (%) was found in the NHBO-BCP group than in the NHBO-mBCP group (P<0.05). A higher blood vessel count (%) and level of VEGF staining (%) were found in the HBO-mBCP group than in the NHBO-mBCP group (P<0.05) (Table 1, Figure 4).
Table 1
New bone (%), blood vessel (%), VEGF staining (%)

HBO: hyperbaric oxygen, NHBO: non-hyperbaric oxygen, BCP: biphasic calcium phosphate; mBCP, Escherichia coli-derived recombinant human bone morphogenetic protein-2-/epigallocatechin-3-gallate-coated biphasic calcium phosphate, VEGF: vascular endothelial growth factor.
a)Statistically significant difference from the NHBO-BCP group (P<0.05); b)Statistically significant difference from the NHBO-control group (P<0.05); c)Statistically significant difference from the HBO-mBCP group (P<0.05).
![]()

DISCUSSION
In a previous study with a 4-week healing period, HBO therapy and ErhBMP-2/EGCG coating had positive effects on angiogenesis and new bone formation [8]. However, a synergistic effect of the combination of HBO and ErhBMP-2/EGCG was not found. The present study was designed to investigate the possibility of such an effect when the bony healing period was extended to 8 weeks. However, a synergistic effect of HBO on new bone formation was likewise not found after an 8-week healing period. This result is in accordance with that of the previous study with a 4-week healing period [8]. A synergistic effect of HBO on angiogenesis was found at 8 weeks, as more blood vessels were found in the HBO-mBCP group than in the NHBO-mBCP group. This result is different from that of a previous study with a 4-week healing period [8]. Most likely, 4 weeks of healing was not enough to see the synergistic effect of HBO on vascularization.
The healing period used in this study was representative of those used in previous studies with similar defects in rats with or without adjunctive HBO [67]. In an 8-week healing study with adjunctive HBO, upregulated gene expression of osteogenic markers, downregulated expression of pro-inflammatory cytokines, a greater number of CD31-positive cells, and higher radiopacity on radiographs were found in rat calvarial defects [7]. In most studies investigating the effects of HBO, rabbit calvarial defects [5621]. The healing period was 6 or 12 weeks. There is difference in healing time between rats and rabbits, as commonly used healing periods for calvarial defects in rats are 2, 4, or 8 weeks [7822]. Therefore, in most studies with rats, a shorter healing period is used than in studies with rabbits. However, too long of a healing time can obscure the difference between the control and experimental groups [23]. In the present study, an 8-week healing period was used to explore the differences from the 4-week period used in the previous study [8].
HBO therapy (2.4 atm) in a high-pressure oxygen chamber was applied to the animals 8 times (one hour per day) in the present study, while in the previous study, HBO therapy (2.5 atm) was applied to rats 10 or 20 times (90 minutes per day) [7]. HBO therapy (2.4 atm) was applied to rabbits for 10 or 20 times (60 minutes per day) in another previous study [24]. Because a few rats died in the high-pressure chamber when 10 sessions of HBO (90 minutes) were applied in the pilot study, the present study used a decreased time (60 minutes) and number of sessions (8 times). However, this change in the protocol seems to have had a negative effect. In a future study, more and longer sessions of HBO therapy should be applied.
During defect healing, the number of newly formed blood vessels and the amount of oxygen (oxygen tension) is important for favorable healing. VEGF is a growth factor that promotes neovascularization. Expression of VEGF was established to be increased by HBO therapy in a previous study [25]. Injuries cause hypoxic zones in soft and hard tissue, and an increased amount of oxygen is important for resolving hypoxic wound conditions. Oxygen tension is increased by HBO therapy [34]. For calvarial defects in rats, a 4-week healing period could be considered as early healing, while an 8-week period corresponds to late healing. It is known that the critical healing time in rat calvarial defects is between 4 and 8 weeks. Additional healing was limited between 8 and 12 weeks [2627].
Based on the results of the present study, it seems that HBO therapy had more beneficial effects on neovascularization and oxygen tension, as indicated by blood vessel count (%) and VEGF (%), than on new bone formation. In other previous studies [2627], extended healing with new bone formation could be expected when HBO therapy is applied; the higher blood vessel count (%) and VEGF expression (%) induced by HBO therapy in an 8-week healing period might explain the prolonged continuation of healing. More new bone formation was not found in the 8-week HBO group than in the 8-week NHBO group. This result is not in accordance with a previous study [728]. Most likely, this difference can be attributed to differences in the types of bone graft material and barrier membrane. In the present study, BCP and mBCP were used. These bone graft materials were found to be less effective than a customized poly (LLA-co-DXO) scaffold in preventing soft tissue ingrowth, by which space for new bone formation could collapse. Therefore, the effect of HBO was limited in collapsed bony defects. It can likewise be assumed that the barrier membrane plays an important role in preventing defect collapse [29]. In another study of calvarial defects in rabbits, it was found that bony healing was compromised when the barrier membrane was not supported properly [30]. In a future study, the application of different bone grafts and a rigid barrier membrane could be considered. The healing pattern also could be investigated during extended healing periods.
Within the limitations of this study, HBO therapy did not have a positive influence on bone formation irrespective of the type of bone graft material applied after an 8-week healing period. Nonetheless, HBO therapy had a positive effect on angiogenic activity.
 XML Download
XML Download