

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sleep is indispensable to human survival. Evidence suggests that sleep imbalance, such as deprivation and/or fluctuations in usual sleep episodes, is significantly associated with diminished quality of life while influencing adverse physical and psychological health outcomes.1 Studies have reported that sleep durations of more or less than 7 or 8 hours in a 24-hour period are associated with cardiovascular disease, diabetes, obesity, depression, automobile accidents, work failures, learning and memory problems, and excess mortality. Several socioeconomic, cultural, and racial factors influence sleep duration. Short sleep duration is more common in people who are older, care for young children, are unmarried, work long hours, consume alcohol, or are overweight or obese.2
Dizziness and vertigo are frequent and disabling symptoms in primary care units but remain unexplained in 40%–80% of patients. Dizziness and vertigo may have serious individual and social effects, causing interruption of daily activities in 40% of affected individuals.3 Falls pose an important health risk in the elderly and are known to be associated with morbidity and mortality. Negative physical and mental consequences from falls also can lead to impaired quality of life, loss of independence, or premature admission into a nursing home. Some authors reported that patients with dizziness showed a decrease in deep sleep and an elevated arousal index in comparison with healthy controls.45 Although no studies have investigated the relationships between various sleep disturbances and dizziness and falls among a community-population, sleep deprivation can modify the posterior parietal cortex, which is important for processing vestibular information regarding space representation.6 Additionally, gender differences could influence on the sleep and dizziness significantly. Gender difference in sleep become apparent after the onset of puberty. Menstrual cycles, pregnancy, and menopause can alter sleep architecture. For example, women have better sleep quality compared with men, with longer sleep times, shorter sleep-onset latency and higher sleep efficiency.7 Regarding the dizziness, women were more often affected compared with men. It could be suggested that a woman's monthly hormonal variation would be actually the trigger for migraine and dizziness episodes in the premenstrual period, as well as the use of hormones for contraceptive purposes.4 Hence it could be hypothesized that sleep disturbances may be associated with dizziness and gender factor may influence on the sleep and dizziness differently. Understanding and identifying the associations among these factors in a large-scale study would greatly contribute to patient care and relief of social burden for these conditions. The present study was undertaken to report the national prevalence of dizziness and vestibular dysfunction in South Korea, based on survey data obtained from the Korea National Health and Nutrition Examination Survey (KNHANES) 2010–2012 and to investigate the associated factors.
METHODS
Study population
This study was based on data collected during the 2010–2012 KNHANES and the secondary analysis of a large data set. The KNHANES is a nationwide survey designed to assess national health and nutrition levels accurately and has been conducted by the Division of Chronic Disease Surveillance under the Korea Centers for Disease Control and Prevention since 1998. A field survey team that included an otolaryngologist and nurse examiners for health assessments traveled with a mobile examination unit and performed interviews and physical examinations. The survey consists of a health interview, a nutritional survey, and a health examination survey. The survey amasses data via household interviews and by direct standardized physical examinations conducted in specially equipped mobile examination centers. The KNHANES methodology has been described in detail previously and further details are listed in “The 5th KNHANES Sample Design” and reports, made accessible on the KNHANES website (https://knhanes.cdc.go.kr/knhanes/index.do). The KNHANES annual reports, user manuals and instructions, and raw data are available on request.567
Every year, 10,000–12,000 individuals in about 4,600 households are selected from a panel to represent the population, using a multistage clustered and stratified random sampling method that is based on national census data. Survey sample weights were used in all analyses to produce estimates that were representative of the non-institutionalized civilian Korean population. The sample included 12,499 participants > 19-years.
Survey for sleep duration and dizziness
Sleep duration was assessed by self-reported questionnaire. Five categories of sleep duration were defined: less than 5 hours per night, 6 hours per night, 7 hours per night, 8 hours per night, and more than 9 hours per night. Participants were asked whether they had experienced dizziness or imbalance (“Have you been dizzy or unstable within the past year?”). Participants who responded positively to this question were queried concerning the positional dizziness and falls in the past 12 months using the following questions. “Have you had severe vertigo when you rotated your head into a supine position or when you sat up from bed or lay down in the morning?” (no/experienced in the past 12 months/experienced at the time of survey) and “Have you ever fallen unexpectedly in the past 12 months?,” respectively.
Lifestyle habits
Data on medical history and lifestyle habits were collected using self-reported questionnaires about recent and current behavior. Smoking status was classified into never smoker (persons who have never smoked), ex-smoker (persons who smoked in the past but do not smoke currently), and current smoker (persons who smoke currently). Based on the amount of alcohol consumed per day during the 1-month period before the interview, the subjects who drank more than 30 grams per day were designated as heavy drinkers. To assess physical activity levels, a regular exerciser was defined as an individual who incorporated at least 20 minutes of vigorous intensity physical activity at least 3 days a week or at least 30 minutes of light/moderate-intensity physical activity at least 5 days a week.
Anthropometric and laboratory measurements
Weight and height were measured by well-trained medical professionals such as nurses or medical technicians. Standing height was measured when the subject faced directly ahead with shoes off, feet together, arms by the sides, and heels, buttocks, and upper back in contact with the wall. The unit of height was measured in centimeters with one decimal point using SECA 225 (SECA, Hamburg, Germany). Body mass index (BMI) was calculated as weight (kg)/height (m2). Waist circumference (WC) was measured at the level of the midpoint between the iliac crest and the costal margin at the end of a normal expiration to the nearest 0.1 cm.
Metabolic syndrome was defined as 1) a WC more than 90 cm in men and more than 80 cm in women, according to the International Diabetes Federation criteria for Asian countries; 2) a fasting blood sugar more than 100 mg/dL or being on medication use for elevated glucose; 3) fasting triglyceride more than 150 mg/dL or cholesterol lowering medication use; 4) high-density lipoprotein-cholesterol less than 40 mg/dL in men and less than 50 mg/dL in women or cholesterol-lowering medication use; and 5) systolic blood pressure more than 130 mmHg and/or diastolic blood pressure more than 85 mmHg or being on an antihypertensive drug treatment for patients with a history of hypertension. Metabolic syndrome diagnosis requires at least three of the five components to be present.
Statistical analysis
Statistical analyses were performed using SAS ver. 9.3 software (SAS Institute, Cary, NC, USA) to reflect the complex sampling design and sampling weights of KNHANES and to provide nationally representative prevalence estimates. The procedures included unequal probabilities of selection, oversampling, and nonresponse so that inferences could be made about the Korean adolescent participants. Prevalence and 95% confidence intervals for dizziness were calculated. The Rao–Scott χ2 test (using PROC SURVEYFREQ in SAS) and logistic regression analysis (using PROC SURVEYLOGISTIC in SAS) were used in a univariate analysis to test the associations between gender and risk factors in a complex sampling design. Participant characteristics are described using means and standard errors for continuous variables and numbers and percentages for categorical variables. A final logistic regression model was used to examine the association between sleep duration and dizziness. We first adjusted for age (model 1), age, BMI, smoking status, alcohol intake, and regular exercise (model 2), and then for age, BMI, smoking status, alcohol intake, regular exercise, metabolic syndrome, stress, and tinnitus (model 3).
RESULTS
A total of 12,499 respondents were included in our study, comprising 5,406 (43.25%) males and 7,093 (56.75%) women, and 2,690 had experienced dizziness or imbalance in the prior 12 months. The baseline characteristics of the study subjects according to gender are shown in Table 1. Mean age was higher in women than in men (P < 0.001). Study participants with current smoker and heavy drinker had significantly higher in men. Routine exercise, job, and WC were significantly more frequent in men, whereas metabolic syndrome and tinnitus were significantly more frequent in women. The prevalence of dizziness was higher in women than that in men (P < 0.001).
Table 1
Characteristics of the participants by gender (n = 12,499)
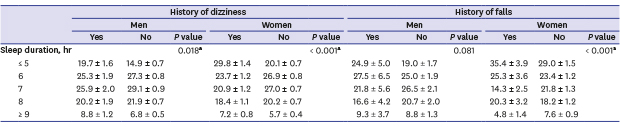
The association between sleep duration category and dizziness or falls is shown in Table 2. Both men and women with severe short sleep duration (≤ 5 hours) and severe long sleep duration (≥ 9 hours) tended to have more dizziness and falls than others.
Table 2
Prevalence of the dizziness according to the sleep duration by gender

Table 3 summarized the adjusted odds ratios (ORs) for dizziness in relation to sleep duration. The adjusted OR for sleep duration is not significant in dizziness for men. Meanwhile, the risk of dizziness was significantly associated with sleep duration in only women. Compared to participants with optimal sleep duration (six to eight hours), those with severe short sleep duration (≤ 5 hours) and severe long sleep duration (≥ 9 hours) adjusted for the confounders showed the high OR with larger than 1.4, which meant that severe short or long sleep duration had an increased dizziness risk after adjusting for the confounders.
Table 3
Adjusted ORs and 95% CIs for assessing relationship between sleep duration and dizziness using logistic regression model

OR = odds ratio, CI = confidence interval, BMI = body mass index.
aModel 1: adjusted for age; bModel 2: adjusted for age, BMI, smoking status, alcohol intake, and regular exercise; cModel 3: adjusted for age, BMI, smoking status, alcohol intake, regular exercise, metabolic syndrome, stress, and tinnitus; dSignificant at P < 0.05.
DISCUSSION
Although dizziness and falls are closely associated with excessive daytime sleepiness no study has evaluated the relationship between sleep duration and dizziness and falls in the general population.89 In the present study, we found that shorter or longer sleep duration were associated with dizziness and falls in Koreans. However, despite the similar tendency of the association between sleep duration and dizziness in both gender, only women had a significant association between shorter or longer sleep duration and dizziness.
Several population-based studies have attempted to estimate the distribution of sleep duration and prevalence of dizziness.13 In this study, sleep duration distribution in Koreans aged greater than 19 years was only 7.5% (men, 7.1%; women, 6.1%) for the individuals with severe long sleep duration, 19.1% (men, 15.6%; women, 22.6%) for the individuals with severe short sleep duration, and 73.4% (men, 77.3%; women, 71.4%) for the individuals with moderated sleep duration (6–8 hours), showing the highest percentage. These results are similar with those of Park et al.2 and Shankar et al.10 The overall prevalence of dizziness was 19.5% (men, 14.4%; women, 25.1%), and the prevalence of dizziness was significantly higher in women than that in men.
As methods to evaluate dizziness, age distribution, and the survey period of each study varied, substantial differences in dizziness prevalence may exist, and, subsequently, direct comparisons among studies are difficult. However, the prevalence of dizziness from previous studies was 15%–30%, showing that our results are similar with previous results.3 Although dizziness must be objectively diagnosed by a clinician, an appropriate evaluation of vestibular function is practically difficult in a large study. However, it is also important to know the prevalence of self-reported dizziness which can determine whether they are likely to seek medical attention.3911 Several authors have evaluated the prevalence of subjective dizziness and its risk factors in general or community populations with data based on self-reported dizziness questionnaires.3911
Previous studies have indicated that individual characteristics, such as eating patterns, physical activity, socioeconomic status, and smoking habits, are meaningful correlates of shorter or longer sleep duration.12 Several studies have reported that sleep disturbances and excessive sleepiness may be associated with dizziness.91314 However, these studies mainly evaluated the effect of sleep duration on general features except dizziness or assessed the impact of the partial sleep pattern on dizziness in specified aged population. By contrast, methodologically, our study evaluated the association of the classified sleep duration with dizziness among a community population. These features would mean that we could include large population (more than 10,000) and assess the detailed sleep duration effect. Additionally, we measured the dizziness and fall in the same population, respectively, which show the individual effect of sleep duration on vestibular function as well as physical imbalance.
In view of results, we demonstrated that both long and short sleep duration would be harmful to the vestibular function in the general population. Most of the related studies measured the effect of only short or long sleep duration on vestibular function. Considering the relationships between sleep duration and physical and psychological health outcomes, a significant relationship may exist between sleep duration and dizziness. We found a U-shaped association between sleep duration and dizziness using 2010–2012 KNHANES data. In other words, both short (< 6 hours) and long (≥ 9 hours) sleep durations have been associated with increased risks of dizziness in men and women. However, logistic regression analyses revealed that dizziness was more common in short and long women sleepers after adjusting for sociodemographic and health-related variables.
Although the underlying mechanism linking short or long sleep duration and dizziness is not yet known, an abnormal sleep pattern is known to have negative effects on cognitive function. Sleep deprivation seems to disrupt vital biological processes necessary for cognitive function and physical health.15 The short (< 6–7 hours) or long sleep duration (> 7–8 hours) was found to be related to the risk for stroke.16 Vertigo and balance disturbances may involve not only the brainstem and cerebellar structures, but the temporal lobes as well.17181920 Cognitive deficits, such as poor concentration and short-term memory loss, are associated with vestibular abnormalities.21 The mechanisms by which vestibular dysfunction is associated with cognitive dysfunction are unclear, although several potential pathways have been hypothesized. Loss of peripheral vestibular input may lead to atrophy of areas within the cortical vestibular network, which notably includes the dorsal thalamus, the temporo-parietal junction, and the hippocampus. Atrophy of these structures may in turn result in impairments in visuospatial memory and perception.22
Additionally, although our observation that abnormal sleep duration may be associated with a higher risk of dizziness among women is a novel finding, the mechanism underlying this gender-specific association is unknown. The possibility of a difference in self-reporting of sleep habits between men and women cannot be ruled out, as suggested in a previous analysis that evaluated the relationship between gender and subjective measures of sleepiness.23 Furthermore, more consideration may be given to social roles and psychosocial differences between men and women when interpreting vestibular health and sleep pattern findings. For example, men may be more reluctant to seek medical counseling and, thus, men seeking treatment may be more adversely affected than women.2425 Furthermore, a general increased sensitivity of reporting body sensations and/or a different reporting style of somatoform symptoms have been suggested to result into such an woman predominance.26 Further studies are needed to investigate the role of gender as a possible effect modifier on the association between sleep and functional outcomes.25
This study had three major strengths. First, we used a nationally representative, community sample of Korean adults. Secondly, we evaluated the relationships between sleep durations and dizziness by subdividing sleep duration into five categories. Based on this category and analysis, we found that short sleep duration (less than 5 hours per night) or long sleep duration (more than 9 hours per night) were associated with dizziness and falls in the Korean men and women. Additionally, we used three models that each considered possible confounding variables in a series of logistic regression analyses to minimize the confounding effect of possible sleep determinants.2 After adjusting the variables, we could identify that the above mentioned relationship was shown in the only Korean women.
By contrast, this study also had several limitations. First, sleep duration and dizziness were reported only by respondents and were not recorded or observed directly. This may bias our results, as there is only modest correlation between reported and recorded sleep. Additionally, the questionnaire evaluation for dizziness may be dependent on the participants' decision and answers, which could make the inclusion of dizziness more heterogeneous. However, although there were some studies with objective sleep data, those measures are not practical for large, nationally representative samples.27 Furthermore, self-reported sleep duration has been used widely in epidemiological studies examining the relationship between sleep duration and morbidity and mortality.11228 A previous study also evaluated the dizziness based on the same questionnaire data from the KNHANES.3
Although from one standpoint, one might consider the prevalence of dizziness as measured by objective balance function tests to be a more scientific estimation of the prevalence of dizziness, it is likely that patient-centered perceptions of their dizziness are more likely to be the drivers of healthcare seeking behaviors for dizziness. In other words, there is significant importance attached to determining the population-based self-reported prevalence of dizziness. Secondly, our data consider only abnormal duration of sleep. Additional sleep problems, such as snoring, apnea and daytime sleepiness, should be investigated in future studies. Third, the related variables of which the presence or absence may be associated with vestibular dysfunction and could affect the results were not able to be evaluated and the participants with other acute disease status, such as BPPV, were not able to be excluded from this study.
However, KNHANES is a nationwide cross-sectional study to select a representative sample of the Korean population. This survey employed stratified multi-stage design based on age, gender, and residence geographic area. The characteristics such as the nationwide population-based study would overcome the limitation related the acute disease status.2930 Finally, medications such as diuretics, antiarrhythmics and psychotropics were not evaluated in this study. Polypharmacy is regarded as an important risk factor for falling in the elderly. Despite these shortcomings, the present study is the first population-based study to assess the relationship between sleep duration and dizziness in the general Korean population. Our results could suggest that clinician need to consider the vestibular function of those with abnormal sleep duration. In future, further longitudinal studies or well controlled studies would be helpful to understand the complex relationship between vestibular dysfunction and abnormal sleep duration.
In conclusion, data from the 2010–2012 KNHANES indicate that abnormal sleep duration, such as short or long duration, is associated with dizziness in women. The results of this general population-based study on the prevalence of abnormal sleep duration and its relationship with dizziness will contribute to their prevention and management in the Korean population.
 XML Download
XML Download