

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Overseas travel has become increasingly popular. In 2014, the annual number of international tourists exceeded 1,133,000,000 globally and is estimated to reach 1,800,000,000 by 2030.1 International travelers are at risk of contracting infectious diseases while abroad.2 As many as 75% of short-term travelers to developing nations report experiencing some health impairment.3
Travelers are potentially susceptible to diseases related to their destination country, activities during travel, and their own preexisting illnesses.4 Communicable diseases are preventable or can be minimized by precautions taken before, during, and after the journey.5 Travel health counseling is recommended before departure and is aimed at updating vaccination status and providing health-related travel advice. The World Health Organization (WHO)6 recommends consulting a physician 4 to 6 weeks before departure to receive necessary vaccines and ensure adequate prevention of travel-associated risks.6
Yellow fever, a mosquito-borne hemorrhagic fever, is the only disease for which there is a mandatory vaccine policy for individuals traveling to endemic countries.7 Receiving a yellow fever vaccination (YFV) is one of the common reasons travelers seek pre-travel consultations. YFV is offered by government-designated clinics and quarantine offices in Korea.8 Often other infectious diseases that are preventable by vaccines or chemoprophylaxis are also communicable in yellow fever-endemic regions, such as Africa and South America. Such infectious diseases include malaria, typhoid, meningococcal diseases, hepatitis A, and cholera. Further, depending on the travelers' immunity or the season, boosters of regular vaccines such as of hepatitis B, tetanus, and influenza should be recommended.
Even though previous studies have reported the patterns and characteristics of travelers, none revealed the factors that affected the compliance of travelers to receive recommended vaccination or malaria prophylaxis. In this study, we analyzed the determinants of compliance of travelers, who sought pre-travel consultation for YFV, with other vaccination.
METHODS
Data collection
The study was conducted at the travel clinic of the Infectious Diseases Department, Inha University Hospital, Korea. This travel clinic provides counseling before international departure and offers vaccines as well as preventive measures against other travel-related risks. We used data of the clients who visited our clinic to receive YFV between January 2016 and September 2018.
The information obtained included attendees' demographic characteristics (age, gender); travel pattern (length of stay, purpose of travel, destination); time of visiting clinic before departure; vaccines prescribed; and the price of prescribed vaccines.
Four physicians who are trained in vaccines and tropical diseases counseled the travelers. Advice was based on the recommendations of the Centers for Disease Control and Prevention (CDC) (United States)9 and the Korean Centers for Disease Control and Prevention.1011 Physicians recommended the appropriate vaccines and explained about the adverse effects of vaccines or drugs.
They surveyed which vaccinations the travelers have received either for travel or for mandatory recommendation for adults, and decided the required vaccination or malaria prophylaxis for each traveler. For hepatitis B, the traveler was inquired whether he or she has immunity against it, and if he or she did not cognize immunity, serology for hepatitis B antibody was checked. For hepatitis A, if the traveler was younger than 40 years old, vaccination was recommended without confirming the immunity unless he (or she) received the vaccination before.11 If the traveler was aged between 40 to 49 years, immunity was checked and vaccination was recommended according to immune status. If the traveler was aged equal to or older than 50 years, hepatitis A vaccination was not recommended.
Cholera vaccination was recommended for those who travel to countries where active Cholera transmission has occurred according to the CDC (United States).9 For those who travel to areas without active transmission, but where cholera outbreak has been reported, the risk of ingesting contaminated water or food was assessed, and if the risk was equal to or higher than moderate, vaccine was recommended.
Tetanus vaccine is a mandatory adult vaccine. However, according to CDC, it is recommended for those who travel to provinces with limited access to health care service, who plan to do humanitarian aid work, and who are at risk of being injured during travel.12 Thus, we recommended tetanus vaccine to those who are assessed to be at risk during travel.
The term “visiting friends or relatives (VFR)” referred to the broadened definition suggested by Barnett et al.13, including those whose primary purpose of travel is to visit friends or relatives, regardless of epidemiologic risk, race, ethnicity, administrative or legal status.
Data analysis
Clients who received at least one vaccination or malaria prophylaxis following a physician's recommendation were considered to be compliant. Those who did not receive other prophylaxis despite physician's recommendation but only received YFV were considered to be noncompliant.
Factors that affected compliance of the clients were analyzed. Factors included age, gender, length of stay, purpose of travel, destination, the time the travelers visited the clinic before departure, and the price of the prescribed vaccines. The associations of compliance and the factors were analyzed by a χ2 test and logistic regression model using SPSS version 19.0 software (SPSS statistics, IBM, Armonk, NY, USA).
RESULTS
During the period from January 2016 to September 2018, 658 clients visited the travel clinic for YFV.
Travelers' demographics
The demographic data of the study population are shown in Table 1. The population included travelers from 19 to 77 years old with a median of 48 years. Travelers were evenly distributed in each age group, while 2% were over 70 years. Men comprised 61.9% of the population. Approximately half of the patients (52.3%, 344/658) who received other vaccination or malaria prophylaxis were considered to be compliant. Malaria prophylaxis was most commonly prescribed with YFV (70.3%, 209/344), followed by typhoid vaccination (60.8%, 209/344) and tetanus vaccination (29.9%, 103/344). The median cost for other chemoprophylaxis was USD 72.93, four fold the cost of YFV. Travelers who sought pre-travel health advice 14 days before departure comprised 40.3% (213/528), while those who sought advice more than 21 days before departure comprised 38.5% (204/528). The destination for half of the travelers (52.4%, 344/528) was South or Central America. Africa was the second frequent destination; 15 Asia travelers (Indonesia, India, Malaysia, Myanmar, Saudi Arabia, Sri Lanka, and Philippines) were included, also. The most common purpose of travel was tourism or VFR (27.9%, 183/528). The majority of attendees traveled for fewer than 30 days (80.5%, 377/528).
Table 1
Demographic characteristics of travelers

![]()
Univariate analysis
Significantly more travelers sought pre-travel consultation more than 21 days before their trip and were considered to be compliant (62.3%, P = 0.02) (Table 2). A higher percentage of compliant clients traveled to Africa and Asia (58.4% and 60.0%, respectively; P = 0.011). Further, travelers with a specific reason for travel were more likely to be compliant (business or education, 55.1%; missionary, 64.5%; tourism, 60.1%; P = 0.008). Gender, age and length of stay did not significantly affect compliance.
Table 2
Predictive factors for compliance with vaccination or malaria prophylaxis before international travel

![]()
Multiple analysis
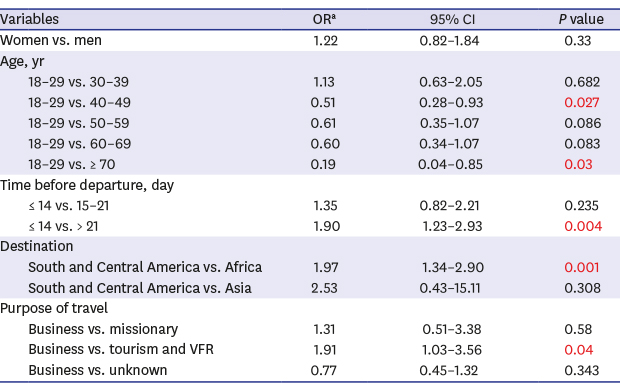
When odds ratio (OR) was adjusted by its variables, age and gender, travelers in age groups of 40–49 years and over 70 years were less compliant than the 19–29 years old population (OR, 0.51; 95% confidence interval [CI], 0.28–0.93; P = 0.027 and OR, 0.19; 95% CI, 0.04–0.84; P = 0.03, respectively) (Table 3). Travelers who visited the clinic more than 21 days before departure were more compliant than those who visited 14 days or fewer before (OR, 1.90; 95% CI, 1.23–2.93; P = 0.004). Travelers to Africa were more compliant than those visiting South and Central America (OR, 1.97; 95% CI, 1.34–2.9; P = 0.001). Also, those who traveled for tour or to visit friends or relatives were more compliant than those who departed for business (OR, 0.77; 95% CI, 1.03–3.56; P = 0.04).
Table 3
Multiple logistic regression analysis of predictive factors for compliance with vaccines and malaria prophylaxis at a travel clinic

VFR = visiting friends or relatives.
aAdjusted by its variables, age and gender; bStatistically significant.
![]()
DISCUSSION
Yellow fever is a mosquito-borne flavivirus infection endemic in 32 countries in Africa and 13 in South America.14 It is a viral hemorrhagic fever and carries a case-fatality rate of 20% to 50%. The WHO reports approximately 50 to 1,200 cases of yellow fever each year.15
The growth of air travel has diminished the barriers to the spread of this disease. Each year, approximately 9 million tourists travel to countries where yellow fever is endemic.16 YFV is currently the only vaccine that is required for international travel under International Health Regulations.7 For many decades, vaccination against yellow fever has been required for travelers entering endemic countries in order to prevent the importation of the yellow fever virus.16 In the Republic of Korea, doctors who work at 43 internationally authorized vaccination-designated centers are authorized to prescribe YFV.10
The destinations of most travelers who seek travel centers for YFV are tropical regions in Africa or South America. Those continents are endemic for not only yellow fever but also other communicable diseases, such as malaria, typhoid, meningococcal disease, polio, rabies, hepatitis A and B, and cholera.1517 Administering vaccines or malaria prophylaxis for endemic diseases as well as routine vaccinations is a crucial responsibility of pre-travel consultation, because vaccine-preventable diseases contribute significantly to morbidity and mortality in travelers.4
The most frequently prescribed vaccines or prophylaxis with YFV was that for malaria, followed by typhoid vaccination, in our study. Because malaria is the most common disease that contributes to morbidity and mortality among travelers to tropical regions, accentuation of malaria prophylaxis at pre-travel clinics is important.18 The high incidence of malaria prophylaxis prescription at our clinic is consistent with the knowledge that malaria is the most fatal infectious disease contributing to travelers' morbidity. However, adherence to malaria prophylaxis was not traced. Because of the long course of malaria prophylaxis, previous studies reported that 37% to 92% of travelers did not complete courses of prophylaxis.1920 Further evaluation is required to trace the adherence to the prophylaxis and the determinants of appropriate adherence.
Compared with travelers in other countries, a large proportion of Korean travelers sought health advice only 1 or 2 weeks before departure. In Swedish studies, 40% to 50% of travelers sought pre-travel health advice 1 month or more before leaving.521 In our study, approximately 40% of travelers visited a clinic for consultation fewer than 14 days before travel, while only 38.6% visited more than 21 days before departure. Even though the Korean government recommends travelers to seek pre-travel consultation at least 21 days before departure, many travelers showed lack of insight of importance of sufficient beforehand time to visit travel clinics. Short interval between visiting the travel clinic and departure may cause insufficient immunity following vaccination, as well as inappropriate schedule for multiple vaccinations. Because having consultation at least 21 days before departure was significantly associated with compliance with vaccination or malaria prophylaxis in our study, visiting a clinic before travel with sufficient time should be emphasized. Poor adherence to vaccination or malaria prophylaxis in old age groups (40–49 years and over 70 years) compared to higher compliance in young age group (19–29 years) indicates plans to enhance compliance of old age groups should be contrived. Due to longer life expectancy and a better quality of life, a growing number of travelers are over 65 years old.22 Previous study has shown that despite their age and chronic conditions, many elderly traveled to countries with low medical standards, including malaria and yellow fever endemic countries.23 Lower percentage of the elderly travelers received vaccination at consultation compared to young and middle-aged travelers, the finding is compatible to that of our study.23 The reason for poor adherence in the old attendees may be explained by low risk behavior during travel, fear of side effects of vaccination, cost, and that they had already been immunized previously. However, considering their impaired immunity, plans to increase pre-travel consultation and compliance to vaccination should be contrived.
Another finding in this study is that, business travelers were less complaint with vaccination or malaria prophylaxis than tourists and those who travel to visit friends or relatives (VFR). Previous studies reported poor adherence to vaccination or malaria prophylaxis among business travelers.2425 Because they usually visit for pre-travel advice closer to departure date, travel for short duration, and obtain pre-travel health advice not for their own volition but because of responsibility, they are less likely to be compliant to physicians' recommendations.24 In the light of severe business travel related illness and mortality,19 employers should highlight the importance of pre-travel health consult and receiving appropriate vaccination.
This study has several limitations. First, this study includes only one travel clinic. More centers should be added for more significant results. Second, the study was conducted retrospectively. We are planning to conduct a prospective study in a larger number of centers and include surveys for travelers. Third, we considered the traveler compliant if he or she received one or more other vaccinations other than YFV. Further analysis that distinguishes those who got all vaccinations required and those who received only some vaccinations is in need. Fourth, our recommendations referred to CDC guidelines, which might be high standard for Korean travelers. For example, cholera vaccination was recommended not only for travelers who visit provisions where there are ongoing cholera outbreak, but also where there have been outbreaks before. High standard of vaccine recommendation may have exaggerated the number of noncompliant. Another limitation is that purpose of travel was unknown for a large number of travelers (336, 51.1%), which may have weakened accuracy in analysis.
Despite these limitations, our study is noteworthy in that it is the first study to evaluate compliance with pre-travel vaccination and its relationship with visiting time, as well as other factors. Even though the WHO recommends seeking pre-travel consultation 4 to 6 weeks before departure, the association between the time and actual compliance of vaccination is unknown.6 This study is also unique because it was conducted in a travel clinic specialized for YFV. A limited number of clinics exist that are authorized to prescribe YFV in the Republic of Korea; therefore, the travel patterns of attendees who seek YFV have not been studied sufficiently.
In conclusion, in our YFV clinic, pre-travel consultation at least 3 weeks before departure is associated with a high compliance with vaccination or malaria prophylaxis. Further, travelers to Africa were more compliant with receiving vaccinations, suggesting that both physicians and travelers should not disregard the risks in South and Central America, as well as tropical countries in Asia. Also, poor compliance of the elderly and business travelers is a challenge to physicians, and plans to enhance adherence should be contrived. Further study including surveys for travelers at multiple centers is required.
 XML Download
XML Download