

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Eikenella corrodens, one of the Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella (HACEK) group, is fastidious, slow-growing, facultatively anaerobic, gram-negative rod commonly found in oral cavity, gastrointestinal and genitourinary tracts.1) Since recognized as a clinical pathogen in 1974, Eikenella infections have been described primarily in adults. Eikenella species is known to cause central nervous system (CNS) infection, sinusitis, endocarditis, intraabdominal infection, liver abscess, and osteomyelitis in adults.23) However, E. corrodens infection in children and adolescents have rarely been reported and clinical characteristics of Eikenella infections in children are not well described.4)
Here, we report a case of E. corrodens epidural abscess complicated by sinusitis in a previously healthy 13-year-old boy who recovered after management with antibiotics and surgery.
CASE
A 13-year-old boy was referred to our hospital for management of uncontrolled fever. A week prior to referral to the hospital, he had headache, vomiting, and fever. During the 2 months before this visit, he complained of occasional headaches requiring no medical attention. He denied any specific past medical history including recurrent acute otitis media or sinusitis. The patient was managed with oral amoxicillin/clavulanic acid for 5 days with a diagnosis of bacterial sinusitis. His symptom did not respond to the management, and he was first admitted to other hospital where he began to receive empirical treatment with intravenous vancomycin and cefotaxime under the impression of bacterial meningitis. At this admission, the patient was alert and oriented, had a fever up to 40°C with chill. Initial laboratory results were as follows: white blood cell (WBC) count 2,300/μL (81.4% neutrophils, 17.9% lymphocytes), hemoglobin 12.2 g/dL, platelet count 43,000/μL. Lumbar puncture and brain imaging were not performed.
Two days later, he was referred to our hospital because his symptoms worsened. On admission, he was febrile and conscious, but drowsy for a brief moment. No abnormalities were found in the cardiovascular, respiratory or gastrointestinal systems. He did not have signs of meningeal irritation nor show abnormal neurologic signs. His pupils were normal, but purulent discharge from right ear was noticeable. Right tympanic membrane was erythematous and bulging.
His initial vital signs were as follows: blood pressure, 144/61 mmHg; pulse rate, 140 beats per minute; respiratory rate, 20 breaths per minute; and axillary temperature, 39.5°C. A complete blood count revealed a WBC count of 5,850/μL, with a differential of 87.2% neutrophils, 11.1% lymphocytes, and 1% monocytes. The hemoglobin was 12.2 g/dL and platelet count was 21,000/μL. C-reactive protein was 10.96 mg/dL and erythrocyte sedimentation rate was 6 mm/hr.
Brain magnetic resonance imaging (MRI) revealed 4.5 cm sized diffusion restrictive lesion with air-fluid level anterior to right temporal lobe suggesting epidural empyema. Sphenoid sinusitis along with bilateral ethmoid sinusitis, right mastoiditis and otitis media were also noticed (Fig. 1A). Lumbar puncture was performed on the third hospital day when platelet counts were 33,000/μL. Lumbar puncture demonstrated clear cerebrospinal fluid (CSF) with an opening pressure of 27.5 cmH2O. CSF analysis revealed 10 lymphocytes/mm3, zero polymorphonuclear cell, protein of 53 mg/dL and glucose of 61 mg/dL. No organism grew from CSF and blood. Culture of ear discharge grew Staphylococcus epidermidis, suggesting contamination of skin flora. The patient continued to receive intravenous cefotaxime and vancomycin and the fever resolved after 8 days.
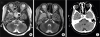 | Fig. 1Brain T2 weighted image show 4.5×3.5 cm sized epidural empyema with air-fluid level in the right temporal lobe (white arrow) as well as bilateral ethmoid (black arrow), sphenoid sinusitis (arrow head), and mastoiditis (asterisk) (A), empyema size increase to 5.6×3.4 cm (white arrow) with interval development of an abscess at the right sphenoid sinus (arrow head) (B). Post-operative brain computed tomography showed near-complete removal of epidural abscess and fluid accumulated in the sphenoid sinus (C).
|
On the 7th day, intravenous meropenem replaced cefotaxime because of redeveloped high fever and increased amount of purulent otorrhea. Increased size of subdural or epidural empyema to 5.6×3.4 cm and probable abscess formation at right sphenoid sinus were noticed on follow up brain MRI (Fig. 1B). Exploratory burr hole trephination of cranium and endoscopic sphenoidotomy were performed (Fig. 2). During the burr hole trephination, 13 mL of foul-smelling pus was evacuated from the abscess that was located at epidural space near the right temporal lobe. Sphenoid sinus with accumulated pus was massively irrigated with normal saline. Immediate postoperative brain CT revealed near complete removal of the epidural abscess and fluid within the sphenoid sinus (Fig. 1C). Following surgery, fever subsided and general condition improved gradually. Bacterial culture of pus obtained from epidural empyema and specimens taken from right sphenoid sinus yielded E. corrodens. It was sensitive to ceftriaxone, imipenem, amikacin, gentamicin, and levofloxacin but was nonsusceptible to penicillin. Vancomycin and meropenem were discontinued after 12 days of administration and cefotaxime was resumed. He was discharged without any symptoms after completing 23 days of intravenous cefotaxime treatment. He continued oral cefixime for 3 weeks. He remains well until 6 months after surgery.

DISCUSSION
We report a case of E. corrodens epidural abscess presumably originated from sphenoid sinusitis in a previously healthy child. The patient recovered without complications after the management with antibiotics and surgical intervention.
E. corrodens is commonly found in oral cavity, gastrointestinal, and genitourinary tracts as normal flora.5) It has been reported primarily in adults presenting head and neck infection, sinusitis, pulmonary infection, cervical spinal epidural abscess, endocarditis, and liver abscess.2567) As E. corrodens is inhabitant of oropharynx, head and neck infections were most frequently reported, some of which were associated with dental manipulation and human bites.89) Patients having predisposing factors were more commonly affected than those who did not have; Sheng et al.8) reported about two thirds of patients (63–77%) had underlying medical illness including malignancy, alcoholism, stroke, or diabetes mellitus, and Brooks et al.7) demonstrated 95% of cases had medical illness or history of trauma. It mostly presents indolent and prolonged course and often causes polymicrobial infection with coexisting organisms such as Staphylococci, Streptococci, and Bacteriodes species, and Escherichia coli.47)
Pediatric E. corrodens infection has been reported less frequently than adults. Paul et al.4) demonstrated E. corrodens could be a significant pathogen in children by reviewing 54 cases of pediatric E. corrodens infection. As reported in adults, head and neck region (41%) was most commonly affected, followed by extremities (16%), CNS (11%), gastrointestinal tract (9%), and respiratory tract (9%). Coinfection with other organisms was also commonly observed, and predisposing factors for infection had a greater association with Eikenella infection.
Literature search revealed 16 cases of CNS infection in children among 38 cases of Eikenella infection from 1944 to 2015.910111213141516171819) CNS infection caused by Eikenella species included subdural, epidural, intraparenchymal and intraventricular abscess, meningitis and septic cavernous sinus thrombosis. Sinusitis preceding the development of CNS infection was found in 7 patients, and 3 had congenital cyanotic heart disease. Foreign body aspiration was noted in 2 cases and trauma history in one case. In addition to antibiotic administration, surgical procedures such as drainage of abscess, sinusectomy, or mastoidectomy were required to cure the Eikenella CNS infection except one case.
Seven cases of Eikenella infection in adults have been reported in Korea.6202122232425) The majority of them had predisposing factors and their mean age was 62.9 years old with male preponderance. Three presented pulmonary infection such as lung empyema. Others presented with a cervical epidural abscess, gastrostomy site infection, liver abscess, and mediastinal abscess. It had a tendency to form abscess involving liver, mediastinum or lung area in 4 cases. However, to our knowledge, there was no report of E. corrodens infection in children and adolescents in Korea.
In particular, this report illustrated epidural abscess developed from chronic sphenoid sinusitis in a previously healthy boy. Initial brain MRI suggested that epidural empyema to right temporal lobe area was secondary to chronic sphenoid sinusitis. Furthermore, E. corrodens grew from both the epidural abscess and right sphenoid tissue, which supports that sphenoidal sinusitis was the primary lesion of epidural abscess. This patient had occasional headaches that were never treated with antibiotics, which might have led to a formation of bacterial abscess in the sinuses. At the time of presenting worsening symptoms of sinusitis and fever, E. corrodens might have already resulted in subsequent spread to the temporal lobe. When a patient with acute sinusitis shows worsening symptoms or signs of increased intracranial pressure, a high index of suspicion for intracranial extension is essential.
E. corrodens was often overlooked as pathogens for sinusitis. There are several reasons: 1) There are always possibilities of contamination since it is normal flora of oral cavity.1) 2) It usually takes indolent course until symptoms appear.4) 3) It has not been regarded as a critical or common pathogen in bacterial sinusitis.
E. corrodens has shown distinct antibiotics susceptibility pattern from that of other anaerobes.7) This bacterium has been primarily susceptible to penicillin, amoxicillin, third generation cephalosporins, carbapenems, and new quinolones.8) Although it is a facultative anaerobe, antibiotics against anaerobes such as clindamycin and metronidazole are reported to be resistant.8) Aminoglycosides are reported to be relatively ineffective.7)
This case was first treated with vancomycin and cefotaxime as the empirical antibiotics for bacterial meningitis, but he did not respond well. After a drainage of abscess and sinusotomy, the patient finally recovered. The improvement after operation supports that adequate and timely surgical management is critical to achieve clinical resolution with favorable outcome.48)
In conclusion, E. corrodens can cause serious complication, particularly in children with untreated bacterial sinusitis. Clinician should consider brain abscess as a complication of bacterial sinusitis. E. corrodens should be investigated as a possible pathogen causing sinusitis and CNS infection even in previously healthy children.
 XML Download
XML Download