

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chest pain is a common cause of emergency department (ED) visits and a major burden on healthcare resources [1]. Because not all patients need immediate medical treatment or intervention, ruling in and ruling out pathologies are equally important. Rapid diagnosis of acute myocardial infarction (AMI) is important for early initiation of appropriate treatment in patients with this life-threatening disorder; AMI must be excluded to ensure safe discharge of low-risk patients intended for outpatient follow-up. Biomarkers, such as creatine kinase myocardial band (CK-MB) and troponin I (TnI), are considered the gold standards for the diagnosis of AMI; however, their elevation requires some time once myocardial necrosis has occurred [23]. Accordingly, early diagnosis of AMI in patients with no or mild TnI elevation is challenging.
Biomarkers with a pathophysiological background independent of cell necrosis might facilitate early diagnosis of AMI. Copeptin, a 39-amino-acid peptide on the C-terminal portion of pro-arginine vasopressin, is an early biomarker and is secreted with vasopressin during acute events such as AMI [4]. By having a different pathophysiology with a time course that is complementary to that of TnI as a biomarker of myocardial necrosis, copeptin may have value in the early diagnosis of AMI at initial presentation. Copeptin levels peak early (0–1 hour) after AMI symptoms onset and decrease to routine levels within 12–36 hours in early presenters [5]. The Copeptin Helps in the Early Detection of Patients with Acute Myocardial Infarction (CHOPIN) trial demonstrated the value of copeptin in early rule-out of MI [6]. Furthermore, the 2015 European Society of Cardiology guidelines on the management of patients with acute coronary syndrome (ACS) presenting without ST-segment elevation myocardial infarction (STEMI) state that the use of copeptin with troponin may add diagnostic value [7]. However, recent studies have suggested that copeptin elevation in serum occurs under various conditions [8], such as lower respiratory tract infection [9], sepsis [10], and stroke [11], as well as after AMI [412]; copeptin might be a useful non-specific biomarker [4]. We investigated the performance of copeptin to diagnose AMI as a way to overcome the delay in release of CK-MB and TnI in patients with ACS in an ED setting.
METHODS
Patient selection
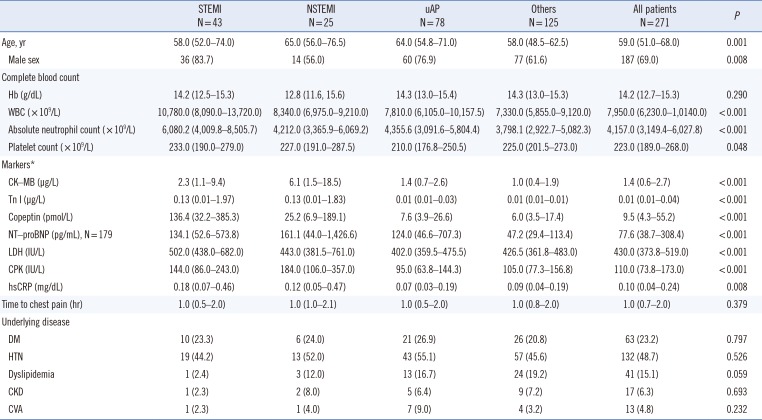
We enrolled 271 patients older than 18 years with chest pain onset within six hours of presentation and suspected ACS who presented at the ED of Gachon Gil Medical Center, Incheon, Korea, between May 2017 and August 2017. The time of chest pain onset was determined based on patient/bystander information, and the times of symptom onset and ED arrival were recorded in an electronic medical record. Patients with traumatic causes of chest pain were excluded. Initial patient assessments included a physical examination, 12-lead electrocardiogram (ECG), chest X-ray, and blood assays including conventional serum CK-MB and TnI assays. The initial diagnosis was made by an emergency physician and verified by internal medicine physicians using all available data, which included serial ECG, cardiac markers, and percutaneous coronary intervention results. The clinical characteristics of all patients are summarized in Table 1. Their median age was 59.0 years, and 69.0% were men. Patients were classified into four groups by etiology: (1) ST elevation myocardial infarction (STEMI; N=43), (2) non-ST elevation myocardial infarction (NSTEMI; N=25), (3) unstable angina (uAP; N=78), and (4) other diseases (other; N=125). CK-MB, TnI, and copeptin levels were higher in patients with AMI than in patients with uAP or other diseases (Table 1). This study was approved by the Institutional Review Board of Gachon Gil Medical Center (GCIRB2017-160), which waived the requirement for informed consent.
Determination of serum CK-MB, TnI, and copeptin levels
Venous blood for investigational biomarker analysis was routinely collected at the time of ED arrival. Serum CK-MB and TnI levels were measured using an automated, sandwich chemiluminescent immunoassay (Advia, Centaur XP, Siemens Healthcare Diagnostics Inc., Tarrytown, NY, USA). After routine laboratory tests, residual serum samples (≥500 µL) were kept frozen at <−70℃ until measurement of copeptin in August 2017. Morgenthaler, et al. [13] showed that prolonged frozen storage does not affect copeptin levels. Copeptin levels were measured using a commercial sandwich immunoluminometric assay, the BRAHMS Copeptin KRYPTOR kit on a BRAHMS KRYPTOR compact plus analyzer (BRAHMS GmbH, Hennigsdorf, Germany). The precision of the copeptin assay was tested at two levels (6.12 pmol/L and 110 pmol/L) by running five replicates over five days. The within-run precision and between-run precision CVs were <10%, demonstrating satisfactory repeatability. The limit of quantification (LoQ) was 1.23 pmol/L, and the analytical measurable range (AMR) was 500 pmol/L. Initial studies used a copeptin cut-off level of 14 pmol/L; however, recent studies have suggested that a 10 pmol/L cut-off level might be more appropriate for ruling out early AMI [1415]. Accordingly, we used a second-generation copeptin assay and 10 pmol/L as the cut-off level.
Statistical analysis
Baseline characteristics including sex, age, and laboratory findings were analyzed using SPSS, Ver. 22.0 (IBM, Chicago, IL, USA). Data were not normally distributed. Hence, data were presented as median (interquartile range, IQR) and analyzed using the Kruskal-Wallis test. Pearson's chi-square test was used to compare categorical variables. P<0.05 was deemed significant.
Diagnostic performance was assessed by ROC curve analysis using MedCalc (Ver. 18.2.1; MedCalc Software, Ostend, Belgium), which was performed using Youden's index. This index is the point on the ROC curve furthest from the line of equality (diagonal line) and can be used to differentiate non-informative (area under the curve [AUC]=0.5), less accurate (0.5<AUC≤0.7), moderately accurate (0.7<AUC≤0.9), highly accurate (0.9<AUC<1), and perfect assays (AUC=1). We assessed the performances of the three biomarkers alone and in combination by comparing AUCs [12]. ROC curve comparison to analyze the diagnostic performance of the three biomarkers was calculated for times of ≤1, ≤2, or ≤6 hours after chest pain onset. The time of onset was defined as the time that had elapsed between symptom onset and ED presentation. Additionally, sensitivity, specificity, positive predictive values (PPVs), and negative predictive values (NPVs) for the markers were also assessed by applying a marker-specific cutoff value.
RESULTS
Diagnostic performance of markers
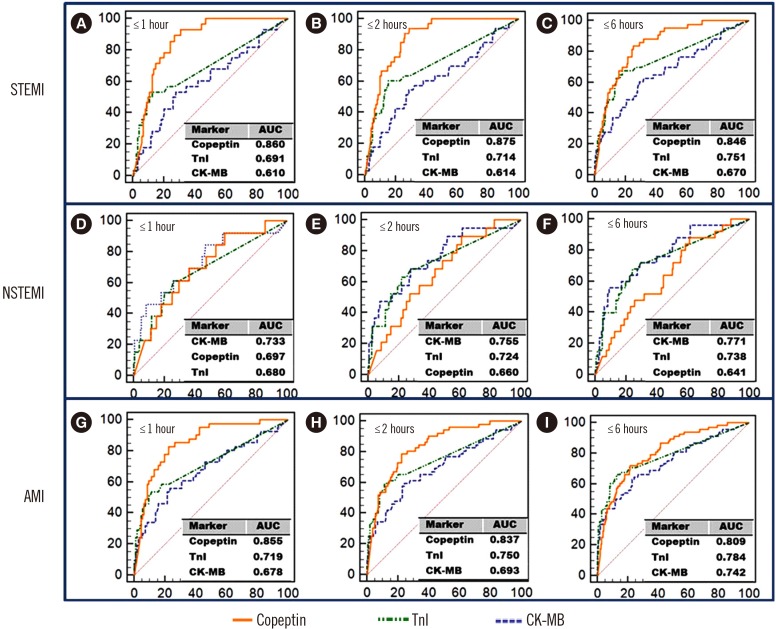
In AMI patients with a chest pain onset of ≤one hour, the ROC AUC at ED arrival was 0.678 (95% confidence interval [CI], 0.596–0.753) for CK-MB, 0.719 (95% CI, 0.639–0.790) for TnI, and 0.855 (95% CI, 0.787–0.907) for copeptin. In AMI patients with a chest pain onset of ≤two hours, the ROC AUC values for CK-MB, TnI, and copeptin were 0.693 (95% CI, 0.626–0.754), 0.750 (95% CI, 0.687–0.807), and 0.837 (95% CI, 0.780–0.884), respectively. In AMI patients with a chest pain onset of ≤six hours, the corresponding values were 0.742 (95% CI, 0.685–0.793), 0.784 (95% CI, 0.731–0.832), and 0.809 (95% CI, 0.757–0.854), respectively. The diagnostic performance of CK-MB and TnI increased with time after chest pain onset. However, the AUC of copeptin peaked within two hours of pain onset (AMI: ≤1 hour; STEMI: ≤2 hours, and NSTEMI: ≤1 hour). Furthermore, copeptin showed moderately accurate diagnostic performance in patients with AMI or STEMI (AUC: 0.809–0.875). ROC curve comparisons showed copeptin had significantly better diagnostic performance than TnI in patients within 1–2 hours of chest pain onset (AMI: P=0.022 at ≤1 hour after chest pain onset; STEMI: P=0.017 at ≤1 hour, P=0.010 at ≤2 hours).
Diagnostic performance of combined biomarkers
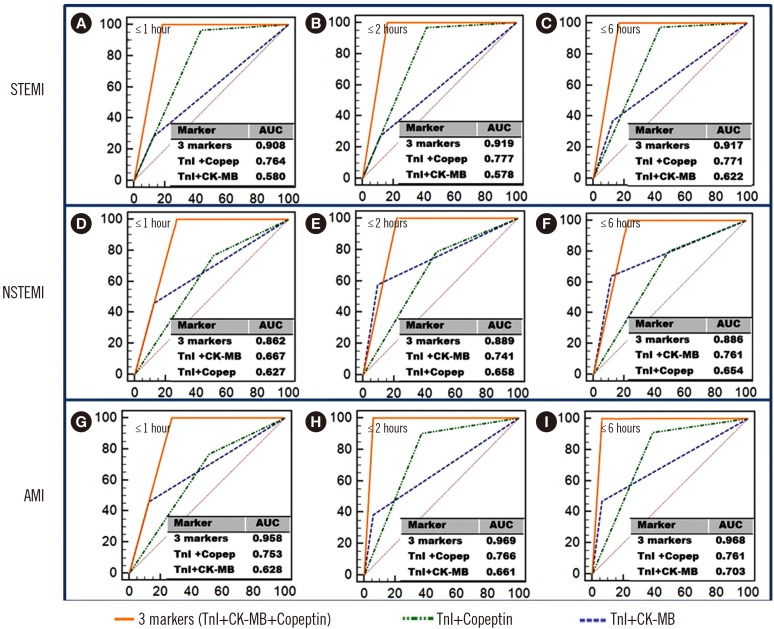
The use of copeptin as a single diagnostic biomarker or in comIbination with TnI was superior to other markers or the CK-MB plus TnI combination currently used for diagnosing AMI and STEMI (Figs. 1 and 2). ROC curve comparisons also showed that copeptin plus TnI had significantly better diagnostic performance than CK-MB plus TnI in the AMI and STEMI groups.
Analysis for sensitivity, specificity, PPV, and NPV
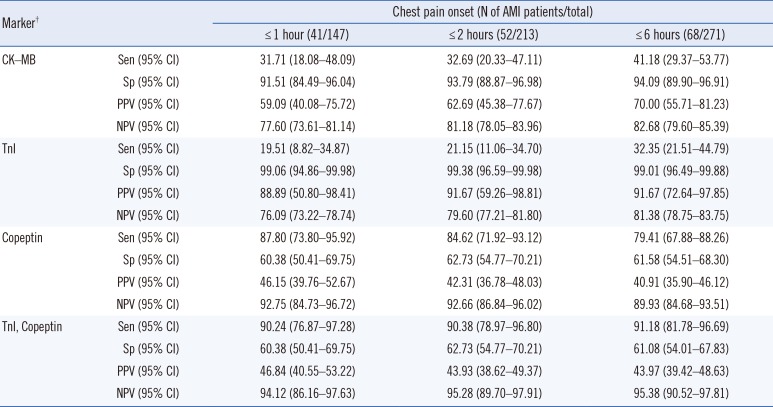
TnI showed the highest specificity and PPV; however, NPV was the lowest among the three biomarkers. Copeptin presented the highest sensitivity and NPV but the lowest PPV among the biomarkers. The addition of copeptin to TnI improved the sensitivity and NPV compared with TnI alone (Table 2).
Biomarker response according to time after chest pain onset in AMI
Copeptin appeared to be able to diagnose AMI shortly after symptom onset, even before TnI elevation (Table 3). In patients at ≤one hour after chest pain onset, only 19.5% showed TnI elevation, whereas copeptin was elevated in 87.8% of AMI patients. In particular, at ≤two hours after chest pain onset, copeptin was elevated in more than 90% of STEMI patients. Copeptin responded more rapidly after chest pain onset than TnI or CK-MB (Table 3).
DISCUSSION
We assessed the diagnostic performance of serum copeptin alone and in combination with CK-MB and/or TnI in patients with acute chest pain (≤six hours) who presented at an ED. Approximately 25.1% of the patients had AMI, and more than half of our patients (147/271) presented within one hour of chest pain onset. Thus, our cohort was suitable for evaluating the diagnostic performance of copeptin as an early biomarker of AMI.
AMI is a major cause of mortality, and rapid diagnosis of AMI is essential for treatment. Although cardiac troponin has a diagnostic value and is mostly used to diagnose AMI, it remains suboptimal in terms of early risk assessment due to the releasing pathophysiology. In the case of early AMI, repetitive tests for cardiac troponin are needed to achieve prognostic accuracy. The 2014 American Heart Association/American College of Cardiology (AHA/ACC) guidelines also recommend a first measurement at presentation and a second measurement within six hours of arrival. Therefore, a diagnostic maker for AMI that responds earlier than TnI is needed.
Boeddinghaus, et al. [16] reported that only 6–22% of patients presenting at an ED with suggestive AMI had mild TnT/I elevation at presentation. In the present study, only 19.5% (STEMI: 17.9%, NSTEMI: 23.1%) of patients who presented within one hour of chest pain onset showed TnI elevation, whereas serum copeptin levels were elevated in 87.8% of AMI, 92.9% of STEMI, and 76.9% of NSTEMI patients. Our results confirm that TnI elevation in AMI is delayed for several hours after chest pain onset [171819]. The early copeptin response was especially prominent in STEMI patients (Table 3, Fig. 1), which concurs with the findings of Reichlin, et al. [17].
The diagnostic value of copeptin as a single biomarker was superior to that of CK-MB or TnI in AMI and STEMI patients within one hour after chest pain onset (Fig. 1). Although copeptin showed high sensitivity and NPV (sensitivity: 79.41–87.80%; NPV: 89.93–98.17%), its specificity and PPV were low (specificity: 60.38–62.73%; PPV: 40.91–46.15%), which hinder its use as a single diagnostic biomarker in AMI. Addition of copeptin to TnI improved sensitivity and NPV compared with TnI alone (Table 2). These findings are consistent with the previous findings [2021]. ROC curve comparison results showed that a combination of TnI and copeptin also improved diagnostic performance, specifically at ≤two hours after chest pain onset; thus, this combination might accelerate therapeutic decision-making in patients with suspected AMI. Using TnI, copeptin, or a combination of two biomarkers may be more efficacious than using CK-MB, especially in STEMI. The CHOPIN trial also showed that copeptin and TnI in combination allowed AMI to be ruled out in patients presenting early with suspected ACS [6]. Furthermore, a combination of copeptin and TnI at presentation has a high NPV to obviate serial analysis beyond three hours of chest pain onset and to facilitate decision making in patients with chest pain in an ED setting [6].
This study is limited by its single-center design and because the blood samples were not obtained serially from the time of symptom onset, which prevented us from examining the relationship between copeptin levels and the time after pain onset in individual patients. Furthermore, we did not perform additional statistical analyses such as the integrated discrimination increment and net reclassification indices.
In summary, copeptin used in combination with TnI improves the diagnosis of AMI in early presenters because copeptin is different from pathophysiological biomarkers. Addition of copeptin to TnI improved sensitivity and NPV, and both markers are complementary in early diagnosis of AMI. A TnI plus copeptin dual marker strategy, rather than a TnI plus CK-MB strategy, might facilitate “ruling in” and “ruling out” AMI in early presenters in the ED setting.

 XML Download
XML Download