

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ovarian cancer is the eighth most common cancer in women; 290,000 new ovarian cancer cases and 184,000 ovarian cancer-related deaths were estimated to occur in 2018 worldwide [1]. Early detection of ovarian cancer is associated with good prognosis, whereas the five-yr survival rate is very poor (20%–40%) in patients diagnosed at advanced stages. However, only 20% of ovarian cancers are diagnosed at an early stage. Therefore, there is a need for effective detection of early-stage cancer, which requires screening tools with high sensitivity and specificity [12].
Estimation of cancer antigen 125 (CA125) levels and transvaginal sonography are the best and most frequently recommended methods for diagnosing ovarian cancer [345]. However, abnormally high CA125 levels are detected in malignancies of different origins [6]. CA125 levels are strongly affected by various physiological factors (e.g., pregnancy and different phases of the menstrual cycle) and benign conditions, including endometriosis [7]. Therefore, new markers, including human epididymis 4 (HE4) and CA72-4, have been proposed and evaluated. HE4 is overexpressed in ovarian cancer tissues compared with normal ovarian tissues [8]. CA72-4 levels are increased in various epithelial cancers [9]. Although CA72-4 is less sensitive than CA125, it has the advantage of not being influenced by the menstrual cycle or pregnancy [1011]. However, the usefulness of CA72-4 in differential diagnosis of ovarian cancer is not well known.
As no single marker is sufficient for diagnosing ovarian cancers, multiple tests or testing patterns can be combined to achieve high sensitivity and specificity. Potential serum markers that can be tested in combination include CA125, HE4, CA72-4, and TP53 autoantibodies [12]. For example, multiple markers are incorporated in the Risk of Ovarian Malignancy Algorithm (ROMA), Risk of Malignant Index, OVA1 test, and LR2 index [13].
To our knowledge, no study has evaluated the clinical usefulness of tumor markers including CA72-4 in Korean patients with ovarian tumors. We evaluated the clinical usefulness of CA125, HE4, and CA72-4 levels and ROMA values for differential diagnosis of malignant and borderline tumors among suspected ovarian tumors. We also examined the ability of a combination of tumor makers to improve diagnostic yield for malignant and borderline tumors. The effects of endometriosis on tumor markers were also evaluated.
Go to : 
METHODS
Study design and population
This was a retrospective and observational single-center study. Blood samples were collected from 354 patients who underwent a planned surgical procedure at the gynecology clinic at Pusan National University Hospital, Busan, Korea, for a symptomatic or suspected malignant ovarian tumor between June 2015 and July 2018. Samples were collected within one month before surgery; 88 patients were excluded because they underwent pre-operative testing but did not undergo surgery. The sera and clinical information used in this study were provided by the Biobank of Pusan National University Hospital, a member of the Korea Biobank Network. The study protocol was approved by the Institutional Review Board of Pusan National University Hospital (E-2015088). Informed consent for collection, storage, and use of blood samples in biobank was obtained from the patients.
Information on menopausal status, age, diagnosis, histological type of tumor, and day of surgery was collected; when information about menopausal status was not provided, patients <50 years were considered premenopausal, and patients ≥50 years were considered postmenopausal. Two pathologists confirmed the status of surgically resected ovarian tumor tissue histologically, using the International Federation of Gynecology and Obstetrics (FIGO) ovarian staging classification [14].
Two hundred and sixty-six patients (213, 14, and 39 with benign, borderline, and malignant tumors, respectively) were enrolled. The median age (range) at initial diagnosis was 40 years (13–80 years), 42.5 years (13–79 years), and 51 years (13–78 years) for the benign, borderline, and malignant groups, respectively. In total, 177 premenopausal and 89 postmenopausal patients were enrolled. Among the benign group patients, 150 were premenopausal, and 63 were postmenopausal. In the borderline and malignant groups, eight and 19 patients were premenopausal, respectively, whereas six and 20 patients were postmenopausal, respectively. The histological types of the ovarian tumor are shown in Table 1. In the malignant group, there were 15 patients with FIGO stage I, four with stage II, 14 with stage III, and six patients with stage IV.
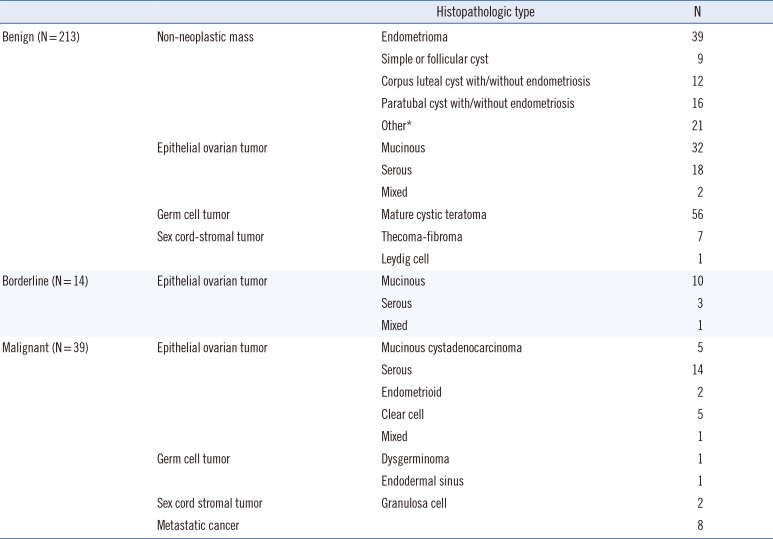
Table 1
Histopathologic types of tumor in patients with ovarian tumors enrolled for differential diagnosis of malignant tumor (N=266)
![]()
Testing of tumor markers
Blood samples were collected in serum separator tubes, centrifuged within 30 minutes after arrival at the laboratory, and stored at −70℃ before use. After the samples were thawed, the markers were measured simultaneously. CA125, HE4, and CA72-4 were measured using Elecsys electrochemiluminescence immunoassays (Roche Diagnostics, Basel, Switzerland) for in the cobas e602 analyzer (Roche Diagnostics). The measurable ranges were 0.6–5,000 U/mL for CA125, 15–1,500 pmol/L for HE4, and 0.2–300 U/mL for CA72-4.
ROMA values for pre- and postmenopausal patients were calculated based on CA125 and HE4 assay results. The ROMA value (%) was calculated as:
exp (PI)/[1+exp(PI)×100], where exp(PI)=ePI and PI is the calculated predictive value [20].
The PI was calculated for pre- and postmenopausal patients separately; PI (premenopausal) was calculated as −12.0+2.38×LN[HE4]+0.0626×LN[CA125], and PI (postmenopausal) was calculated as −8.09+1.04×LN[HE4]+0.732×LN[CA125] [15].
Recommended cut-off levels were CA125≥35 U/mL, HE4 (premenopausal) ≥92.1 pmol/L, HE4 (postmenopausal) ≥121 pmol/L, CA72-4>6.9 U/mL, ROMA (premenopausal) value ≥11.4%, and ROMA (postmenopausal) value ≥29.9%, according to the manufacturer's instructions.
Statistical analysis
Continuous variables were expressed as medians and interquartile ranges (IQRs). Significant differences in parameters among groups were evaluated using the Kruskal-Wallis test for three-group comparisons, and the Mann-Whitney U-test for two-group comparisons. Box plots were constructed to represent marker levels (displaying with the middle two, range and median). The outlier are data points that more than lower quartile −1.5×IQR or upper quartile+1.5×IQR and extreme are data posint that more extreme than lower quartile −3×IQR or upper quartile +3×IQR. To analyze the diagnostic performance of each tumor marker and the ROMA value, sensitivity and specificity were calculated, ROC curves were constructed, and the area under the curve (AUC) of each marker was calculated.
All analyses were performed with SPSS version 23 (IBM Corp, Armonk, NY, USA). P<0.05 (for two-group comparisons) and P<0.017 (for three-group comparisons) were considered significant. Sensitivity and specificity for differential diagnosis of patients in the malignant and borderline groups were calculated for single and various combinations of tumor markers.
Go to :
RESULTS
Tumor markers for differential diagnosis of malignant tumor
For each group, CA125, HE4, and CA72-4 levels and ROMA values were estimated (Table 2). In premenopausal patients, HE4 levels and ROMA values were higher in the malignant group than in the benign group (P<0.001). In postmenopausal patients, CA125 and HE4 levels and ROMA values were higher in the malignant group than in the borderline (P=0.009, P=0.002, and P=0.001, respectively) and benign (all P<0.001) groups. CA72-4 levels were higher in the malignant group than in the benign group (P<0.001).
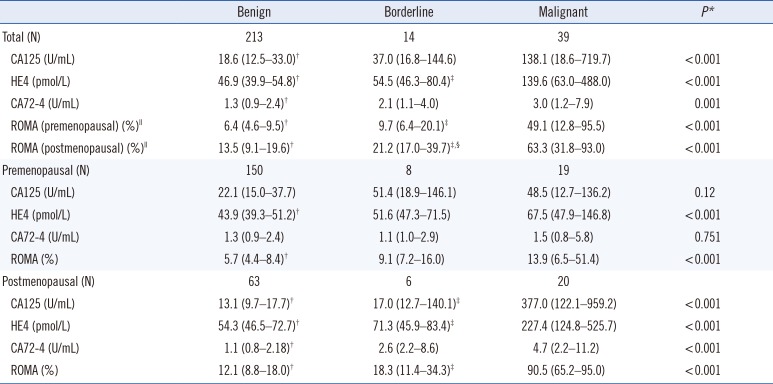
Table 2
Serum marker levels and ROMA values according to menopausal status
Values are expressed as medians and interquartile ranges.
*Indicates a significant difference between malignant, borderline, and benign groups by the Kruskal-Wallis test (P<0.017); †Malignant group vs benign group (P<0.05); ‡Malignant group vs borderline group (P<0.05); §Borderline group vs benign group (P<0.05); ∥Results included patients in premenopausal and postmenopausal state.
Abbreviations: CA, cancer antigen; HE4, human epididymis 4; ROMA, Risk of Ovarian Malignancy Algorithm.
![]()
Among the 19 premenopausal patients in the malignant group, four patients showed high CA125 and HE4 levels; six patients showed high CA125 levels; two patients showed high HE4 levels; and 10 patients showed high ROMA values (≥11.4%). The seven patients with CA125 and HE4 levels below the reference range were patients with mucinous carcinoma, metastatic carcinoma, granulosa cell tumor, or low-grade serous tumor. The two patients with only high HE4 level had endometrioid-type carcinoma. Among the five patients who showed a high CA72-4 level, two showed high CA125 and HE4 levels, two showed only a high CA125 level, and one patient showed CA125 and HE4 levels below the reference range. Among the 20 postmenopausal patients in the malignant group, 14 showed both high CA125 and HE4 levels, four showed only high CA125 level, one showed only high HE4 level, and 19 patients showed a high ROMA value (≥29.9%). One patient with CA125 and HE4 levels below the reference range had clear-cell carcinoma. Among the eight patients with a high CA72-4 level, six showed high CA125 and HE4 levels, and two showed only a high CA125 level.
Among the eight premenopausal patients in the borderline group, one showed both high CA125 and HE4 levels and a high ROMA value (≥11.4%), whereas four showed only a high CA125 level and one only a high HE4 level, respectively. Two patients showed CA125 and HE4 levels below the reference range, whereas there were no patients with a high CA72-4 level. Among the six postmenopausal patients in the borderline group, one showed both high CA125 and HE4 levels and a high ROMA value (≥29.9%), whereas one patient showed only a high CA125 level. Four patients showed CA125 and HE4 levels below the reference range. Among the two patients showing high CA72-4 level, one patient showed high CA125 and HE4 levels, and one patient showed CA125 and HE4 levels below the reference range.
Sensitivity, specificity, and AUC values for distinguishing between malignant/borderline and benign groups and between malignant and borderline/benign groups are shown in Table 3. ROMA value showed the highest sensitivity among all markers, and CA125 showed the highest sensitivity as a single marker. HE4 and CA72-4 showed higher specificity than CA125 and ROMA value. The sensitivities of all markers were higher in postmenopausal than in premenopausal patients. The combination of HE4 or CA72-4 with CA125 showed higher sensitivity than CA125 alone in premenopausal patients. The combination of CA125, HE4, and CA72-4 did not improve sensitivity and specificity compared with the combination of HE4 or CA72-4 with CA125.
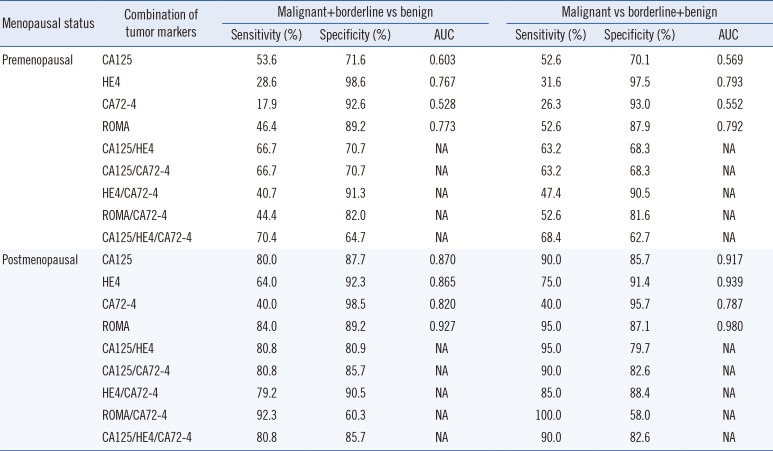
Table 3
Sensitivity and specificity of combinations of tumor markers in predicting malignant tumor/borderline tumor and malignant tumor only
![]()
Effect of endometriosis on tumor markers
Among premenopausal patients, 53 (35.6%) had endometriosis (confirmed by histological examination), and among postmenopausal patients, six (9.5%) had endometriosis. In total, 42.3% (25/59) of the patients with endometriosis had high CA125 levels, whereas only one (1.7%) and two (3.4%) had high HE4 and CA72-4 levels, respectively. Six premenopausal patients (11.3%) with endometriosis had a high ROMA value (≥11.4%), whereas no postmenopausal patient with endometriosis had a high ROMA value (≥29.9%).
As shown in Fig. 1, in the benign group, the CA125 level (median 32.4 U/mL, IQR 20.2–60.6 U/mL) was higher in patients with endometriosis than in those without endometriosis (median 15.3 U/mL, IQR 11.2–25.9 U/mL) (P<0.001); HE4 and CA72-4 levels were not affected by endometriosis. For HE4 and CA72-4, median values of 45.6 pmol/L (IQR 39.3–51.7 pmol/L) and 1.4 U/mL (IQR 1.0–2.3 U/mL) were observed in patients with endometriosis, and median values of 46.9 pmol/L (IQR 40.2–57.3 pmol/L) and 1.2 U/mL (IQR 0.9–2.6 U/mL) were observed in patients without endometriosis (P=0.128 and 0.271). The ROMA (postmenopausal) value was higher in patients with endometriosis (median 16.5% [IQR 13.6–26.0%]) than in patients without endometriosis (median 12.1% [IQR 8.9–17.3%]; P<0.001), whereas the ROMA (premenopausal) value did not differ (median 6.2% [IQR 4.5–8.6%] vs 6.6% [4.6–10.0%]) between the patients with and without endometriosis (P=0.312).
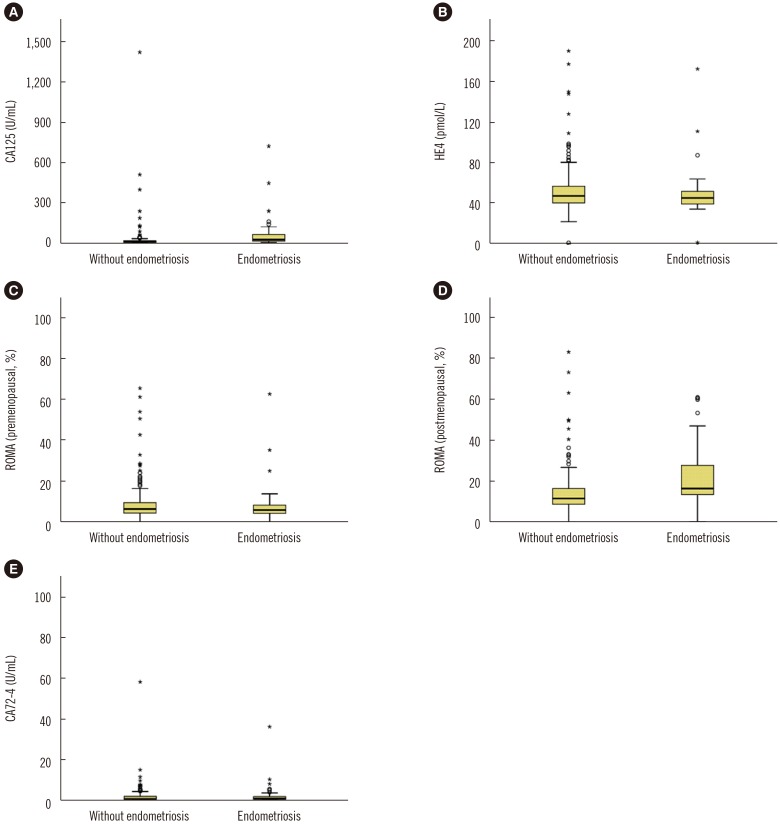 | Fig. 1Serum marker levels and ROMA values according to the presence and absence of endometriosis in the benign group. (A) CA125, (B) HE4, (C) ROMA (premenopausal) value, (D) ROMA (postmenopausal) value, and (E) CA72-4 levels. The whiskers show the maximum and minimum values, with the exception of outliers (circles) and extremes (asterisks).Abbreviations: CA, cancer antigen; HE4, human epididymis 4; ROMA, Risk of Ovarian Malignancy Algorithm.
|
Go to :
DISCUSSION
The present study evaluated the clinical usefulness of CA125, HE4, and CA72-4 levels and ROMA values for differential diagnosis of malignant and borderline tumors among suspected ovarian tumors. CA125 showed the highest sensitivity, and HE4 showed higher specificity for diagnosing malignant tumor using the recommended cut-off in premenopausal and postmenopausal patients. CA125 has a high sensitivity, but poor specificity, which often does not exceed 40% [13]. A meta-analysis of 16 datasets covering 1,342 ovarian cancer patients and 2,516 controls revealed an overall sensitivity of 79% and specificity of 93% for HE4 and overall sensitivity of 79% and specificity of 78% for CA125 [16]. Another meta-analysis based on 28 studies indicated that the sensitivity of CA125 and HE4 levels and DROMA values for diagnosing ovarian cancer was 76.3%, 79.2%, and 85.3%, respectively, and the specificity was 96.6%, 82.1%, and 82.4%, respectively [17]. The significantly higher specificity of HE4 than that of CA125 indicates that HE4 is less likely to be affected by factors other than the malignancy itself. Moreover, HE4 showed better results than CA125 for monitoring ovarian cancer [18]. Numerous reports indicated that combining CA125 with other laboratory and imaging results significantly improved specificity [1519202122].
HE4 has been shown to be the most useful marker for differential diagnosis of ovarian cancer and endometriosis [2324]. In our study, only 1.7% and 3.4% of patients with endometriosis showed increased HE4 and CA72-4 levels, respectively. In previous studies, 42.3% of women with endometriosis had high CA125 levels, confirming the low specificity of this marker [2526]. In our study, CA125 level was higher in patients with endometriosis than in patients without endometriosis, whereas HE4 and CA72-4 levels were not influenced by endometriosis. The role of CA72-4 in differential diagnosis of benign and malignant ovarian tumors is controversial. CA72-4 levels differed between women with ovarian cancer and those with endometriosis [25]. CA72-4 level was elevated in ovarian cancer with limited sensitivity as a single marker; however, when CA72-4 was combined with CA125 and HE4, the sensitivity of the triple marker assay increased by 2.4% compared with that of the dual marker combination of CA125 and HE4 [26]. In our study, of the 53 patients with malignant and borderline tumors, two patients had only high CA72-4 levels. Furthermore, high CA72-4 levels were found in two among the 59 patients with endometriosis and in 10 among the 154 patients with benign tumor without endometriosis.
ROMA value showed a better AUC value and sensitivity than CA125, HE4, and CA72-4 levels in pre- and postmenopausal patients in the present study. A previous study reported that ROMA value showed better performance than CA125 alone or HE4 alone [13]. However, other reports contradicted this finding [272829]. Chan, et al. [28] and Kadija, et al. [29] demonstrated that assessment of ROMA value might be important for improving diagnostic performance in premenopausal patients, as it differentiates malignant tumors from endometrial cysts in premenopausal women.
A limitation of this study is the insufficient number of malignant and borderline tumors. Consequently, it was not possible to analyze diagnostic performance of each marker for differential diagnosis of malignant and borderline ovarian tumor according to various histologic subtypes. Because ovarian tumor has multiple histologic subtypes and the effect of each marker is different, multicenter studies are needed to clarify the histologic subtype correlated with the change in each marker for diagnosis, treatment, and prognosis of ovarian tumors.
In conclusion, ROMA value was the best marker to distinguish malignant and borderline tumors from benign tumors in both pre- and postmenopausal patients. HE4 and CA72-4 can be used in combination with CA125 to increase the diagnostic sensitivity in premenopausal patients. HE4 and CA72-4 provide information on the possibility of CA125 elevation by endometriosis.
Go to :
 XML Download
XML Download