

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ho-Seung Jeon, M.D. , Seok-Ha Hwang, M.D., Seung-Pyo Suh, M.D., Jae-Nam Kim, M.D.
, Seok-Ha Hwang, M.D., Seung-Pyo Suh, M.D., Jae-Nam Kim, M.D.
, Seok-Ha Hwang, M.D., Seung-Pyo Suh, M.D., Jae-Nam Kim, M.D.
Abstract
Spinal adhesive arachnoiditis is an inflammation and fibrosis of the subarachnoid space and pia mater caused by infection, trauma, spinal vascular anomalies, and iatrogenic (surgery and/or puncture). Adhesive arachnoiditis develops various symptoms and signs (gait disturbances, radiating pain, paralysis, and incontinence). On the other hand, adhesive arachnoiditis associated with cauda equina syndrome has not been reported in Korea until now. The authors experienced cauda equina syndrome caused by adhesive arachnoiditis of the lumbar spine with satisfactory results following decompression. We report this case with a review of the relevant literature.
Figures and Tables
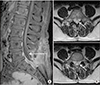
 | Figure 1Preoperative magnetic resonance imagings (MRIs) show adhesive arachnoiditis. (A) Gadolinium-enhanced T1-weighted sagittal MRI shows dural enhancement from the L4–5 disc space level to the S2 level (arrow). (B) T2-weighted axial MRIs show clumping of the nerve roots (arrows).
|
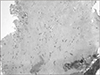
 | Figure 2Intraoperative photographs. (A) Fibrous tissue fragments removed from adhesive arachnoiditis. (B) Severe adhesion of the soft tissue and pale dura were resolved after decompression and laminectomy at the L5/S1/2 level.
|
References
1. Whetstone KE, Crane DA. Cauda equina syndrome resulting from lumbar arachnoiditis after intracranial subarachnoid hemorrhage: a case report. PM R. 2013; 5:539–541.

2. Augustijn P, Vanneste J, Davies G. Chronic spinal arachnoiditis following intracranial subarachnoid haemorrhage. Clin Neurol Neurosurg. 1989; 91:347–350.
3. Faure A, Khalfallah M, Perrouin-Verbe B, et al. Arachnoiditis ossificans of the cauda equina. Case report and review of the literature. J Neurosurg. 2002; 97:239–243.
4. Quiles M, Marchisello PJ, Tsairis P. Lumbar adhesive arachnoiditis. Etiologic and pathologic aspects. Spine (Phila Pa 1976). 1978; 3:45–50.
5. Bourne IH. Lumbo-sacral adhesive arachnoiditis: a review. J R Soc Med. 1990; 83:262–265.
6. Bilgen IG, Yunten N, Ustun EE, Oksel F, Gumusdis G. Adhesive arachnoiditis causing cauda equina syndrome in ankylosing spondylitis: CT and MRI demonstration of dural calcification and a dorsal dural diverticulum. Neuroradiology. 1999; 41:508–511.
7. Delamarter RB, Ross JS, Masaryk TJ, Modic MT, Bohlman HH. Diagnosis of lumbar arachnoiditis by magnetic resonance imaging. Spine (Phila Pa 1976). 1990; 15:304–310.
8. Petty PG, Hudgson P, Hare WS. Symptomatic lumbar spinal arachnoiditis: fact or fallacy? J Clin Neurosci. 2000; 7:395–399.
 XML Download
XML Download