

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Case summary
A 33-year-old woman with a history of cleaning her contact lenses with tap water presented with decreased visual acuity for 1 day in the left eye. The patient showed diffuse corneal edema, stromal infiltration, and radial keratoneuritis, which were thought to be pathognomonic for Aeromonas keratitis. Based on the patient's clinical findings and past history, a diagnosis of Aeromonas keratitis was made and she was prescribed topical fortified cefazolin (50 mg/mL, 5%), tobramycin (3 mg/mL), and 0.02% chlorhexidine per hour. Culture results from the contact lens and contact lens solution confirmed infection by Aeromonas hydrophilia. Polymerase chain reaction results for Aeromonas were negative. After 8 days of treatment, the uncorrected visual acuity was 0.7/0.3 with improvement in her corneal findings.
Figures and Tables
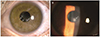
 | Figure 1Anterior segment photographs of the left eye at presentation. Small dense stromal infiltrates at the center (A, arrows) and radial keratoneuritis (B, arrow) were revealed at inferonasal area.
|
 | Figure 2UPGMA phylogenetic trees based on the rpoB sequence. The relationships with the strains of genus Aeromonas and other closely related bacterial strains were shown. Nucleotide sequence of clinical isolate from the patient was revealed as Aeromonas hydrophilia in this tree (highlighted with box). Aeromonas species and Pseudomonas species were closely related in the tree. UPGMA = Unweighted Pair Group Method with Arithmetic Mean.
|
References
1. Naginton J, Watson PG, Playfair TJ, et al. Amoebic infection of the eye. Lancet. 1974; 2:1537–1540.
2. Lorenzo-Morales J, Khan NA, Walochnik J. An update on Acanthamoeba keratitis: diagnosis, pathogenesis and treatment. Parasite. 2015; 22:10.
3. Moore MB, McCulley JP, Kaufman HE, Robin JB. Radial keratoneuritis as a presenting sign in Acanthamoeba keratitis. Ophthalmology. 1986; 93:1310–1315.
4. Feist RM, Sugar J, Tessler H. Radial keratoneuritis in Pseudomonas keratitis. Arch Ophthalmol. 1991; 109:774–775.

5. Mutoh T, Matsumoto Y, Chikuda M. A case of radial keratoneuritis in non-Acanthamoeba keratitis. Clin Ophthalmol. 2012; 6:1535–1538.
6. Shin HB, Yoon J, Lee Y, et al. Comparison of MALDI-TOF MS, housekeeping gene sequencing, and 16S rRNA gene sequencing for identification of Aeromonas clinical isolates. Yonsei Med J. 2015; 56:550–555.
7. Tamura K, Peterson D, Peterson N, et al. MEGA5: molecular evolutionary genetics analysis using maximum likelihood, evolutionary distance, and maximum parsimony methods. Mol Biol Evol. 2011; 28:2731–2739.
8. Lehmann OJ, Green SM, Morlet N, et al. Polymerase chain reaction analysis of corneal epithelial and tear samples in the diagnosis of Acanthamoeba keratitis. Invest Ophthalmol Vis Sci. 1998; 39:1261–1265.
9. Kim YJ, Kim BS, Yoo WS, et al. A case of serratia marcescens keratitis presenting as radial keratoneuritis. J Korean Ophthalmol Soc. 2014; 55:1380–1383.
10. Shilkin KB, Annear DI, Rowett LR, Laurence BH. Infection due to Aeromonas hydrophila. Med J Aust. 1968; 1:351–353.
11. Feaster FT, Nisbet RM, Barber JC. Aeromonas hydrophila corneal ulcer. Am J Ophthalmol. 1978; 85:114–117.
12. Pinna A, Sechi LA, Zanetti S, et al. Aeromonas caviae keratitis associated with contact lens wear. Ophthalmology. 2004; 111:348–351.
13. Motukupally SR, Singh A, Garg P, Sharma S. Microbial keratitis due to aeromonas species at a tertiary eye care center in Southern India. Asia Pac J Ophthalmol (Phila). 2014; 3:294–298.
14. Persson S, Al-Shuweli S, Yapici S, et al. Identification of clinical aeromonas species by rpoB and gyrB sequencing and development of a multiplex PCR method for detection of Aeromonas hydrophila, A. caviae, A. veronii, and A. media. J Clin Microbiol. 2015; 53:653–656.
15. Roels D, De Craene S, Kestelyn P. Keratoneuritis is not pathognomonic of Acanthamoeba keratitis: a case report of Pseudomonas keratitis. Int Ophthalmol. 2017; 37:257–258.
 XML Download
XML Download