

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ureaplasma species, including Ureaplasma urealyticum (UU) and Ureaplasma parvum (UP), are classified as small sized bacteria [12]. The simple genomic structures and limited metabolic activity impose a close and long-term parasitic interaction between the bacteria and the infected cells [12]. In Ureaplasma-related infections, clinical symptoms and signs are often mild or even asymptomatic, making it very difficult to characterize their pathogenicity. Similarly, their parasitic nature and indolent course in infected host cells suggest the possibility of Ureaplasma species as causal pathogens for enigmatic chronic genitourinary infections.
Chronic prostatitis (CP) is one of the most common urological disorders [3]. Some sexually transmitted infections (STIs) may contribute to the pathogenesis of CP [345]. For example, Chlamydia trachomatis that harbor similar genomic simplicity and clinical characteristics as Ureaplasma are found in prostate tissues in patients with idiopathic CP [4]. Through a case and control study, the chlamydial infected men reveal increased leukocyte counts in expressed prostatic secretion (EPS) and exacerbated CP-associated pain severity in men with CP. These findings clearly suggest the association of urinary chlamydia infections with CP and consider the possibility of Ureaplasma species associated CP [5].
Generally, urologists employ multiplex-nucleic acid amplification tests (NAAT) from voided urine samples to reveal pathogens for urethritis and CP in men [6]. Based on the results of these examinations, clinicians must determine the pathogenicity of these bacteria and whether antibiotics are to be prescribed.
While the presence of UU in EPS or in first voided urine sample from CP patients may support the association between Ureaplasma and CP [78], Ureaplasma microbes are not found in the perineal prostate biopsy tissues from idiopathic CP patients [4]. Furthermore, only a handful of case-control studies that estimate unique pathogenicity of Ureaplasma infections in the prostate are currently available [78910]. In addition, we could not find well designed case-control studies with strict diagnostic criteria in defining idiopathic CP [3]. To understand the specific role of Ureaplasma species in CP and to design a strict case-control study, we first excluded patients with gonococcal and chlamydia infections through a multiplex NAAT, as well as patients with cystitis or bacterial prostatitis based on a lower urinary localization test. We had also removed the effects of urethral inflammation form the overall data and re-analyzed the subtracted data to enhance statistical power for CP. Finally, we aimed to evaluate the potential role of Ureaplasma species as causal pathogens in men with CP and clinical features of Ureaplasma infected CP patients.
MATERIALS AND METHODS
1. Study design and ethics statement
Informed consents were obtained from all study participants, and the research protocol was reviewed and approved by the Institutional Review Board of the Dankook University Hospital (IRB No. 201303014). The study was performed in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki, 1964, and Declaration of Tokyo, 1975, as revised in 1983).
A total of 810 first voided urine samples were collected from men who visited Dankook University Hospital Urogenital Infection and Prostate Diseases Clinic from September 2009 to March 2015. During the visit, first voided urine samples were collected into 15 mL centrifuge tubes and were stored at −70℃ until NAAT was performed. The remaining samples were delivered to the central laboratory office to obtain white blood cell (WBC) counts.
The causes for the visit to the clinic included lower urinary tract symptoms, CP-like symptoms, symptoms with lower urinary tract infections, and annual prostate check-up. We excluded 49 cases of chronic bacterial prostatitis by ordinary aerobic prostatic culture methods [11] and 63 chlamydial infected cases by NAAT methods [5]. Other exclusion criteria prior to enrollment were as follows: presence of genitourinary cancer, urinary stone diseases, acute epididymitis, urinary culture-proven cystitis, traumatic urethral stricture, a history of prostate surgery within the past 3 months, and acute urinary retention [3]. Two combined cases of UU and UP were also excluded from the data analysis (Fig. 1).
Clinical information included the age of participants and the presence of CP-like symptoms according to the results from the Korean version of the National Institutes of Health-Chronic Prostatitis Symptom Index (NIH-CPSI) questionnaire. The results of WBC counts in the remaining first voided urine samples were reviewed and classified into the WBC count categories of 0–1, 2–4, and ≥5 per high-power field (HPF). We also reviewed the results of the WBC counts in the EPS from the digital rectal massage, which were also classified into three categories of 0–4, 5–14, and ≥15 WBCs per HPF [5].
Finally, the 696 participants were classified into the following groups according to the results of NIH-CPSI questionnaire and EPS evaluation: the non-CP group (control group), inflammatory CP group (≥15 WBCs per HPF in EPS), and non-inflammatory CP group (<15 WBCs per HPF in EPS) [5]. Here, CP group is defined as men with the presence of pelvic pain or discomfort conditions that had lasted at least 3 months [3]. Three hundred fifty men were categorized into the non-inflammatory CP group and 88 as patients with inflammatory CP. The non-CP group, which included 258 men, was defined as individuals who visited the clinic for annual prostate checkup. Participants in the control group did not report of symptoms of urethral discharge and pain or discomfort items of NIH-CPSI questionnaire.
2. In-house nucleic acid amplification tests
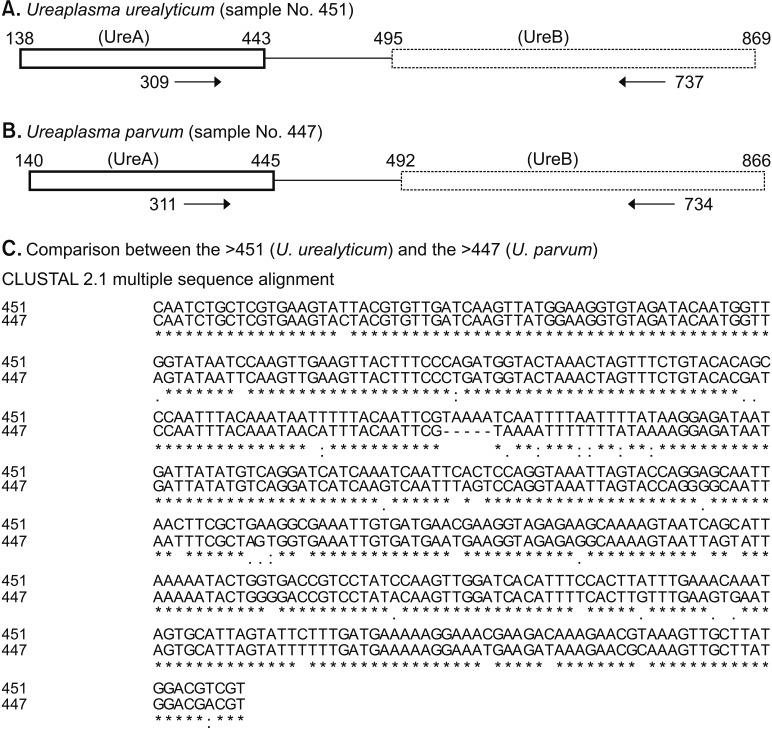
DNA was extracted from the stored urinary sample [5]. From the stored DNA samples, a urease complex area of Ureaplasma species were amplified with a set of consensus primers (forward; 5′-CAA TCT GCT CGT GAA GTA TTA C-3′, reversed 5′-ACG ACG TCC ATA AGC AAC T-3′). The biovars of DNA sequences were determined by the Sanger method (Solgent, Daejeon, Korea) [12]. The sequences were compared with the reference genotypes in the GenBank database (http://blast.ncbi.nlm.nih.gov/Blast.cgi).
3. Statistical methods
We used nonparametric Mann–Whitney U-test to evaluate the difference in the ordinal scores between each Ureaplasma infection and the non-UU/UP group. Pearson chi-square test and Fisher's exact tests were used to evaluate the difference in categorical data. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated with logistic regression analysis. Two-sided null hypotheses of no difference were rejected if p-values were less than 0.05. All analyses were performed using IBM SPSS ver. 23 software for Windows (IBM Corp., Armonk, NY, USA).
RESULTS
1. Sequencing results
We amplified a partial segment of UreA and UreB regions of Ureaplasma species (Fig. 2A, 2B). Because of the clear dissimilarity in DNA sequences between two amplified regions, we could easily distinguish UU infections from UP infections (Fig. 2C).
2. Infection rates of Ureaplasma urealyticum and Ureaplasma parvum in the nonchlamydial nongonococcal setting
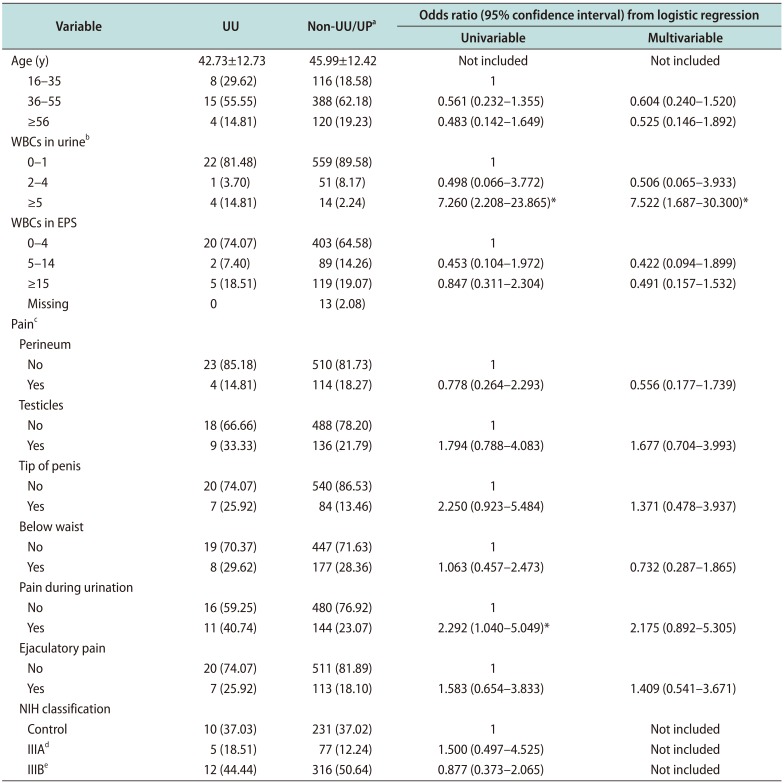
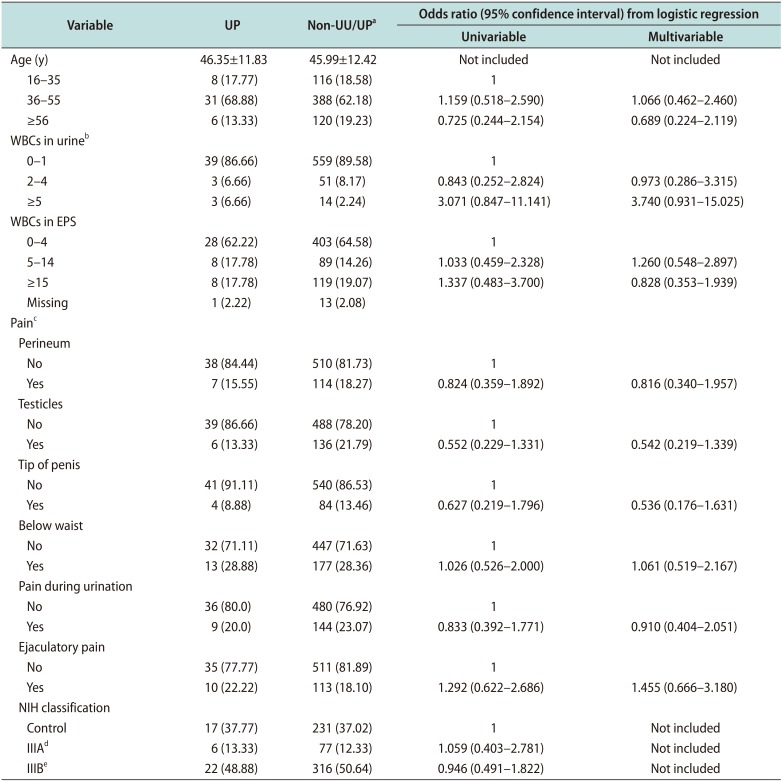
The infection rates of UU, UP, and non-UU/UP in nonchlamydial nongonococcal (NCNG) setting were 3.88% (27/696), 6.46% (45/696), and 89.66% (624/696), respectively (Table 1, 2). Furthermore, the mean age±standard deviation (range of patient age) of the UU, UP and non-UU/UP groups was 42.73±12.73 years (18–72 years), 46.35±11.83 years (19–81 years), 45.99±12.42 years (18–79 years) (p>0.05), respectively.
3. Urethral inflammation by Ureaplasma urealyticum and Ureaplasma parvum
Urinary WBC counts were significantly different among UU, UP, and non-UU/UP groups (p=0.002). Specifically, the rates of UU infection according to urinary WBC counts of 0–1, 2–4, and ≥5 HPF groups were 3.78% (22/581), 1.92% (1/52), and 22.22% (4/18) (p=0.001), respectively (Table 1). Compared to the non-UU/UP group, the UU infected group reported frequent dysuria or pain during urination (p=0.035) (Table 1). Based on multivariable analysis, patients with UU infections had significantly higher probability of ≥5 WBC counts/HPF in urine (adjusted OR [adjOR], 7.522; 95% CI, 1.687–30.300; p=0.005) in the NCNG clinical setting (Table 1). However, there were no significant differences in the symptoms and signs of urethritis between 45 men in the UP positive and 624 men in the non-UU/UP group (Table 2).
4. Chronic prostatitis by Ureaplasma urealyticum and Ureaplasma parvum
The overall infection rates in the control, inflammatory, and non-inflammatory CP groups were 4.15% (10/241), 6.10% (5/82), and 3.65% (12/328) in UU (p=0.612), and 6.85% (17/248), 7.22% (6/83), and 6.50% (22/338) in UP (p=0.968), respectively (Table 1, 2). To remove the effects of urethral inflammation by UU infection, we excluded 18 cases of ≥5 WBC counts /HPF in urine and re-analyzed the remaining 633 case to enhance statistical power. There were no clinical associations in clinical characteristics of pure idiopathic CP cases and the UU infections; the subtracted infection rates in the control, inflammatory, and non-inflammatory CP groups were 3.78% (9/238), 4.17% (3/72), 3.40% (11/323) in UU (p=0.941), respectively.
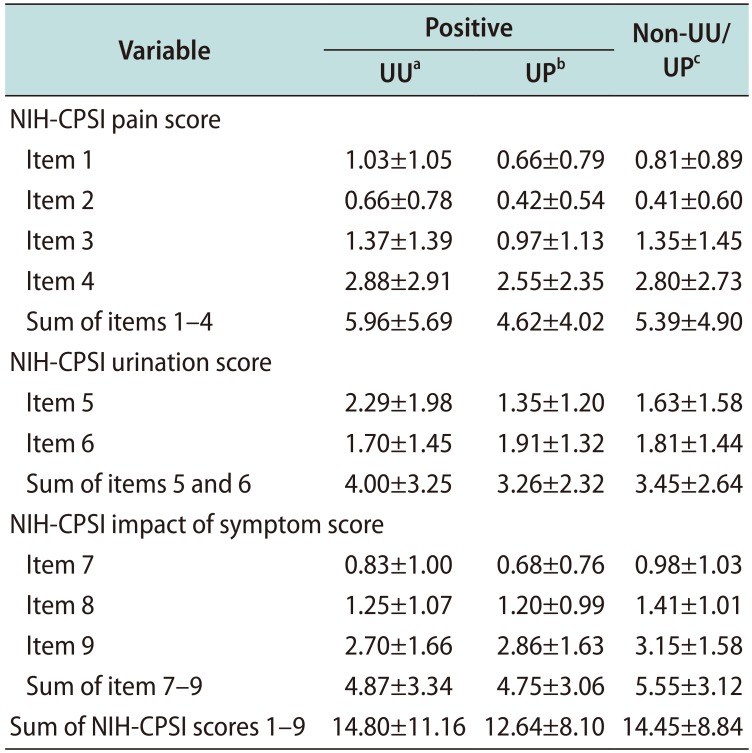
In addition, each UU and UP positive group had similar NIH-CPSI questionnaire profiles compared to the non-UU/UP group (Table 1, 2). Similarly, we could not find any significant difference between the UU or UP infected group and the non-UU/UP group in the pain scores, urination domain, and impact of symptom scores from the NIH-CPSI questionnaire according to nonparametric Mann–Whitney U-test (Table 3). WBC counts in EPS were not statistically associated with the Ureaplama infections (UU, p=0.549 and UP, p=0.778) (Table 1, 2).
DISCUSSION
STIs remain one of the major health issues, causing serious and adverse effects on reproductive health [13]. Recently developed multiplex NAAT methods for STIs can simultaneously detect multiple causative organisms [614]. Various scales of multiplex NAAT assays that range from detection of 2–3 to 7 or more STI pathogens have been developed, and the medical practices for executing multiplex NAAT assays have been financially supported by the Korean National Medical Insurance to suppress the spread of STIs [6]. Consequently, many microbes that are certainly undetected by conventional diagnostic tests have now become recognized by the public health systems.
The overall positive rates for various STIs with multiplex NAAT-based STI tests range from 30% to 50%, depending on study designs [614]. In particular, previous studies consistently report that the most prevalent microbe detected by such methods is UP and UU [614]. As Ureaplasma species are frequently found in coinfections with Neisseria gonorrhea or C. trachomatis in urine samples, combinations of these well-known STIs may alter the clinical characteristics of infected individuals and therefore must be ruled out to evaluate the unique characteristics of Ureaplasma species. Accordingly, cases of N. gonorrhea and C. trachomatis infections were excluded from this study. Our study revealed that the infection rate for Ureaplasma species in the sample population was close to 10%, and UP infections were more frequently found than UU in the NCNG settings.
N. gonorrhea and C. trachomatis microbes can induce male urethritis or CP, therefore they are eradicated by administering specific antimicrobials [5915]. However, urethral inflammatory response after Ureaplasma infections is significantly lower than that of Mycoplasma genitalium or C. trachomatis [16]. In other words, clinical symptoms or signs such as urethral discharge and increased WBC counts in voided urine samples are usually inconsistent following Ureaplasma infections [9]. Unfortunately, well designed case-controls studies that may differentiate the role of Ureaplasma species as causative or bystanders in genitourinary infections are currently not available. Although there is a controversy regarding the pathogenicity of Ureaplasma species in genitourinary tracts, some physicians conventionally prescribe antibiotics regardless [17]. Consequently, Ureaplasma species may be exposed to increased evolutional pressure induced by such frequent medications. Indeed, many Ureaplasma species harbor resistance to conventional antibiotics [1819]. Therefore, the clinical significance or pathogenicity of Ureaplasma infections in male genitourinary organs must be appropriately evaluated to avoid unnecessary treatments.
Ureaplasma species are genetically classified into UU and UP. Although conventional researches in genitourinary Ureaplasma infections have been based on NAAT methods, currently there are no Food and Drug Administration-approved clinical tests to differentiate UU from UP infection in the United States. Therefore, sequencing-based Ureaplasma detection and differentiation methods may be employed as a gold standard until properly-evaluated NAATs are established.
Our results suggest that UU may be associated with NCNG urethritis because UU infections increased the risk of higher WBC counts in urine (≥5 HPF) (adjOR, 7.522; 95% CI, 1.687–30.300). Furthermore, UU infected men had reported more frequently of dysuria or pain during urination than the non-UU/UP group (p=0.035). But, we found that UP was not a pathogen in male urethra. Therefore, UP infections were not justified with antibiotic treatments.
Intracellular incorporating pathogens can also gain a foothold in the genitourinary tract and act as a trigger for chronic inflammation or recurrent epithelial damage, ultimately aggravating chronic genitourinary pain or induce CP [12]. Prostate can harbor various microorganisms that are not detectable by traditional culture approaches but rather are confirmed by prokaryotic DNA amplification and cloning methods [420]. With the abilities of Ureaplasma species to elicit chronic infection in host cell, the possibility of Ureaplasma species-associated CP has been under debate over the last several decades [127810].
Although many urologists have been directed to find laboratory biomarkers for CP, we still lack definitive criteria for diagnosis of the disease [3]. Therefore, patients must be basically evaluated with the NIH-CPSI questionnaire and a lower urinary tract localization test with the Meares–Stamey 4 glass to define CP [3]. In addition, a proper diagnostic workup for CP must rule out other mimicking conditions, similar to our exclusion criteria. While many STI organisms can contribute to the pathogenesis of CP, typical cases of urethritis must be excluded in CP case-control study. Therefore, we removed the 18 cases of urethral inflammation and re-calculated clinical significances in the remaining 633 cases. Nevertheless, even after adjusting for cases of idiopathic CP, statistical significances between clinical characteristics of CP and the UU infections were not found. The frequencies of each item in the pain domain of NIH-CPSI questionnaire were not different between the adjusted UU infected men versus non-infected men.
It has been suggested that WBC counting in EPS is the most accurate method in evaluating prostatic inflammation. Therefore, the variations in EPS WBC concentration is a deciding factor for discriminating inflammatory CP from non-inflammatory CP cases. We found that the 4.73% (20/423) of those with WBC counts in their EPS in the range of 0–4 HPF, 2.19% (2/91) in 5–14 HPF group, and 4.03% (5/124) in ≥15 HPF group had UU infections (p=0.549). Even if the effects of urethral inflammation were excluded, the adjusted data analysis revealed the similar results; 4.31% (18/417) of those with WBC counts in EPS in the range of 0–4 HPF, 2.22% (2/90) in the 5–14 HPF, and 2.65% (3/113) in the ≥15 HPF group (p=0.512). Furthermore, we did not observe a significant difference in the response to the NIH-CPSI questionnaire between the UU/UP positive groups versus the non-UU/UP group. Therefore, we hypothesized that the presence of UU or UP in NAAT from CP patients is not related to the manifestations of CP. Additionally, urinary UU or UP may not be able to invade and trigger inflammation in the prostate because WBC counts in EPS were not statistically different [35]. Therefore, we advised against antibiotic treatment in UU or UP infections in patients with CP.
CONCLUSIONS
Based on the case-control study, our results suggest that urinary presences of UU or UP in patients with CP are not associated with its occurrence. Accordingly, treatment with antimicrobial agents is not reasonable in the cases of Ureaplasma species associated CP. UU is a pathogen because it is associated with male urethral infection, while UP is not a pathogen but a bystander in male urethra.

 XML Download
XML Download