

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Male infertility depends on a variety of conditions, ranging from hormonal disorders to physical problems; however, the aetiology and pathogenesis of male infertility still remain unknown in about 30% of cases [1]. Inflammatory pathologies are among the well-known reasons for male infertility, accounting for 15% of cases [2]. These systemic inflammatory diseases and inflammatory processes may alter sperm function through the production of elevated reactive oxygen species (ROS), determining injuries on sperm DNA, and apoptosis [34].
Since analysing some acute phase reactors, such as serum amyloid A protein, C-reactive protein, interleukins, or interferon-gamma, is not part of routine clinical practise, because of technical difficulties and costs, other inflammation-based prognostic scores, such as the neutrophil-to-lymphocyte ratio (NLR), the monocyte-to-eosinophil ratio (MER), and the platelet-to-lymphocyte ratio (PLR), obtained from a differential white blood cell count (WBC), can be used, thanks to their rapidity and inexpensiveness. The NLR, MER, and PLR have already been reported to play a key role in inflammatory diseases [56789]. The relationship between male systemic inflammation and fertility seems intriguing, but no data about its impact on the assisted reproductive technology (ART) outcomes has been reported. Here, we aimed to evaluate the prognostic role of male systemic inflammatory parameters in intracytoplasmic sperm injection (ICSI) outcomes prediction, in couples undergoing an ovum donation program.
Go to : 
MATERIALS AND METHODS
1. Study schedule
From January 2016 to December 2017, all couples presented to our ARTs Centre were retrospectively considered for this cross-sectional study.
2. Study population
All the recruited couples had a severe female infertility factor (i.e., premature ovarian failure, poor response to controlled ovarian stimulation, previous unsuccessful in vitro fertilization technique), that needed an ovum donation program from donor egg bank with ICSI cycle. We considered for this study all infertile couples from almost one year, whose male spouse presented normal or sub-fertile seminal parameters in almost two seminal analyses [4]. We did not consider for this study male spouse with presentation of azoospermia, ejaculatory ducts obstructions, endocrine hypogonadism, infections, varicocele, retractile testes or history of testicular torsion, previous chemotherapy or radiotherapy, hematologic disorders, chronic inflammatory diseases, and drug therapy. After the initial screening, data were collected from all participants.
3. Patients assessment, andrological visit and laboratory
Baseline characteristics of male patients were recovered from each patient's medical records, including age, height, and weight with body mass index count, smoking and drinking status, use of anabolic steroids, previous diseases or surgery, history of cryptorchidism, medication, and comorbidities. Hormone measurements, including follicle stimulating hormone, luteinizing hormone, total testosterone, aestradiol, and prolactin were collected. Genetic studies were performed, including the karyotype with the examination of microdeletions for chromosome Y and mutation of Cystic Fibrosis Transmembrane Conductance Regulator genes. The complete blood count of all male patients was monitored routinely and collected before performing the ART treatment. All of the blood samples were collected from the antecubital vein, after at least 8 hours of fasting. The hematologic parameters were determined with Coulter LH-780 (Beckman Coulter s.r.l., Milan, Italy) hematologic blood analyser. The NLR, MER, and PLR (expressed in 103/µL) were calculated, by dividing the neutrophil count by the lymphocyte count, the monocyte count by the eosinophil count and the platelet count by the lymphocyte count, respectively. All male patients performed a urine analyses to detect urine tract infections. Fresh seminal fluid for ICSI cycle was obtained by masturbation after 3 to 5 days of sexual abstinence. We collected data of the seminal parameters, as below: abstinence time, sperm volume, semen pH, viscosity, total sperm count, total sperm motility (progressive motility and non-progressive motility), total sperm motility after capacitation and normal sperm morphology. Spermatozoa obtained by ejaculate underwent in-vitro capacitation before ICSI, with the purpose to select spermatozoa with good morphology and motility and to remove the seminal plasma. The serological tests for diagnosis of human immunodeficiency virus, hepatitis B virus, hepatitis C virus, Cytomegalovirus, Treponema pallidum haemagglutination, and rapid plasma reagin (RPR) tests were done. NLR, MER, PLR, and seminal parameters were collected. All parameters were compared with ARTs outcomes: fertilization rate (FR), cleavage rate (CR), and pregnancy rate (PR). Male patients were arbitrarily divided into two groups (A and B) according to the percentage of FR. Group A consisted of patients with FR ≤70% and Group B comprised those with FR >70%.
4. Intracytoplasmic sperm injection technique and embryological evaluation
All oocytes retrieved were submitted to ICSI procedure. Injected oocytes were incubated in 20 µL drops. Embryo morphology was assessed 16 to 18 hours after ICSI, on days 2, 3, and 5 of development when embryo-transfer (ET) was performed, using an inverted microscope with a Hoffmann modulation contrast system. To evaluate the cleavage-stage morphology, the following parameters were recorded: number of blastomeres, percentage of fragmentation, variation in blastomere symmetry, presence of multinucleation, and defects in the zona pellucida and cytoplasm. High-quality cleavage-stage embryos were defined as those with all of the following characteristics: four cells on day 2 or 8 to 10 cells on day 3, <15% fragmentation, symmetric blastomeres, absence of multinucleation, colourless cytoplasm with moderate granulation and no inclusions, absence of perivitelline space granularity, and absence of zona pellucida dysmorphism (classified with the score A). Embryos lacking any of these characteristics were considered to be of low quality (score B and C). To evaluate blastocyst formation, embryos were given a numerical score from 1 to 4 according to their degree of expansion and hatching status, as follows: 1, an early blastocyst with a blastocoel that was less than half of the embryonal volume; 2, a blastocyst with a blastocoel that was greater than half of the embryonal volume; 3, an expanded blastocyst with a blastocoel that completely filled the embryo; 4, a hatching blastocyst. Expanded and hatching blastocysts were classified as complete blastocysts. Thereafter, we evaluated the reproductive outcomes: FR, CR, and PR. The total and normal oocyte FR was calculated by total number of fertilized oocytes and ‘two pronuclear’ fertilized oocytes by the number of injected oocytes, respectively. The CR was calculated by the number of embryos obtained by the number of normal fertilized oocytes. Embryos were transferred into the uterine cavity 48 to 72 or 120 hours after ICSI procedure. Supernumerary embryos were frozen. After 14 days from ET, human chorionic gonadotropin test was performed and we considered clinical pregnancy as the presence of a gestational sac with foetal hearth beat, that can be visualized by ultrasound 5 to 6 weeks after ET.
5. Ethical and statistical considerations
All the patients gave a written informed consent to agree on having their data included into the study. The work was conducted in accordance with the declaration of Helsinki. The present study protocol was reviewed and approved by the institutional review board of University of Florence, Careggi Hospital (2018-017 CINECA 10189). The study did not require any exam in addition to the normal clinical practice. The categorical variables were described using frequency and percentage, and the numerical variables were described using median and interquartile range (IQR) value. Continuous variables are presented as median and IQR and differences between groups were assessed by the Student independent t-test or the Mann–Whitney U-test on the basis of their normal or not-normal distribution, respectively (normality of variables' distribution was tested by the Kolmogorov–Smirnov test). Age-adjusted linear regression analysis was performed to determine the relationship between numeric dependent and independent parameters, and logistic regression analysis was employed to determine significant predictors of pregnancy, FR >70% and cleavage using NLR, PLR, and MER. The study was conducted at a confidence level of 95%. All statistical analyses were completed using Stata software ver. 14 (StataCorp., College Station, TX, USA). For all statistical comparisons, significance was considered as p<0.05.
Go to :
RESULTS
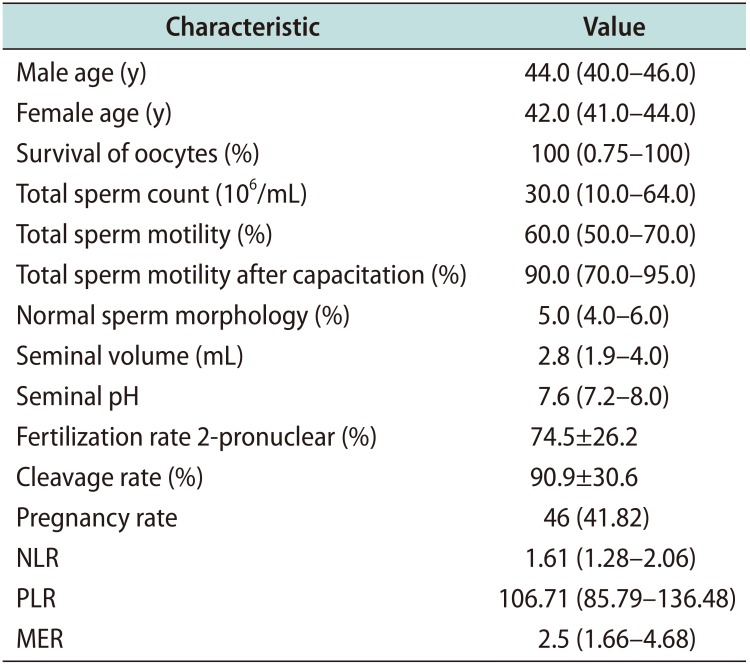
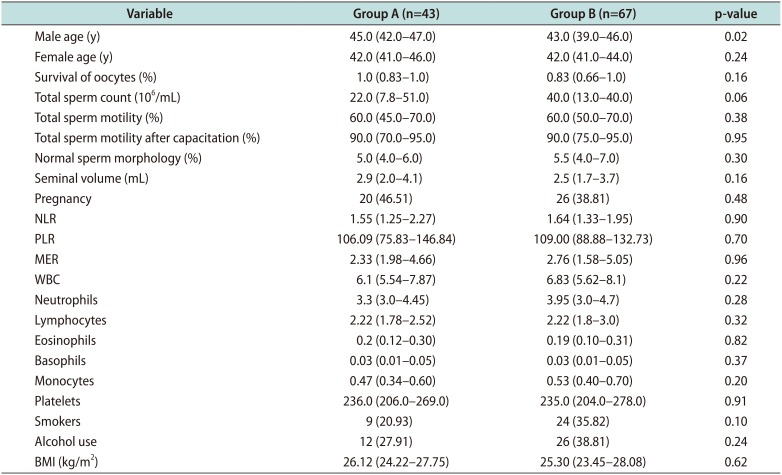
A total of 110 infertile couples were included in the study. This analysis included 694 frozen oocytes by Spanish donor banks. After warming, 590 oocytes survived, resulting viable and mature. A total of 110 fresh ICSI cycles were performed. The baseline characteristics of the study population are shown in Table 1. Overall, 43 patients were included in Group A and 67 patients in Group B (Table 2). We reported pregnancy in 46 cycles (overall PR per cycle of 41.8%). FR was 74.5% and CR was 90.9%. The paternal age seemed to be significantly higher in group A: The median male ages of the group A and the group B were 45.0 years (IQR, 42.0–47.0 years) and 43.0 years (IQR, 39.0–46.0 years), respectively (p=0.02). Median NLR was 1.55 (IQR, 1.25–2.27) in the Group A and 1.64 (IQR, 1.33–1.95) in the Group B (Fig. 1). Median PLR was 106.09 (IQR, 75.83–146.84) in the Group A and 109.00 (IQR, 88.88–132.73) in the Group B (Fig. 2). Median MER was 2.33 (IQR, 1.98–4.66) in the Group A and 2.76 (IQR, 1.58–5.05) in the Group B (Fig. 3). We found no statistically differences between the two groups with respect to NLR, PLR, and MER (p=0.90, p=0.70, p=0.96, respectively). Likewise, no significant differences were found in hematologic parameters, including platelet count, WBC count, neutrophil count, lymphocyte count, platelet count, monocyte count, eosinophil count, and basophil count (p>0.05). Equally, there were no significant differences between the two groups with respect to BMI and current smoking or drinking status (p>0.05).
 | Fig. 1Distribution of neutrophil-to-lymphocyte ratio (NLR) in the two groups. Group A: fertilization rate ≤70%, Group B: fertilization rate >70%.
|
 | Fig. 2Distribution of platelet-to-lymphocyte ratio (PLR) in the two groups. Group A: fertilization rate ≤70%, Group B: fertilization rate >70%.
|
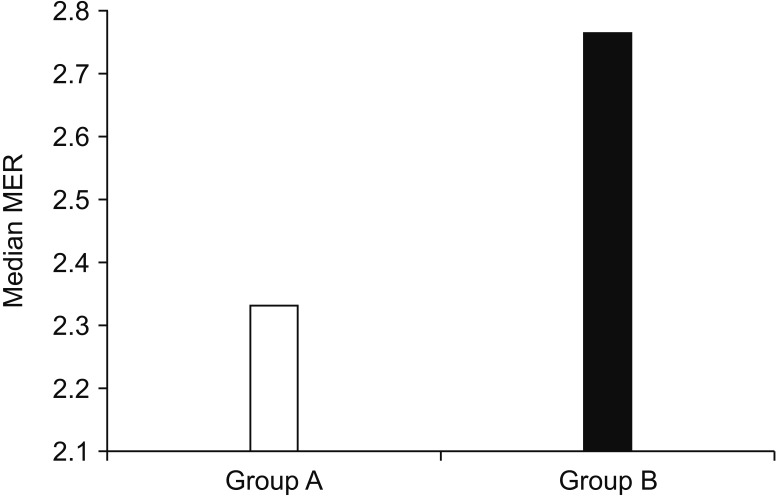 | Fig. 3Distribution of monocyte-to-eosinophil ratio (MER) in the two groups. Group A: fertilization rate ≤70%, Group B: fertilization rate >70%.
|
Table 1
Baseline characteristics of the study cohort (n=110)
![]()
Table 2
Comparison of clinical variables according to fertilization rate
![]()
1. Relationship between neutrophil-to-lymphocyte ratio, monocyte-to-eosinophil ratio, platelet-to-lymphocyte ratio, and seminal parameters
Table 3 showed the age-adjusted linear regression analysis of seminal parameters compared to NLR, MER, and PLR, demonstrating no significant associations with total sperm count, total sperm motility after capacitation, normal sperm morphology, and semen volume. Only total sperm motility was related to NLR with statistic significance (r=−0.02; p<0.05). Moreover, using the univariate logistic regression analysis, we found no associations between NRL, PLR, MER, and the ICSI outcomes, as regard the fertilization, cleavage, and PRs.
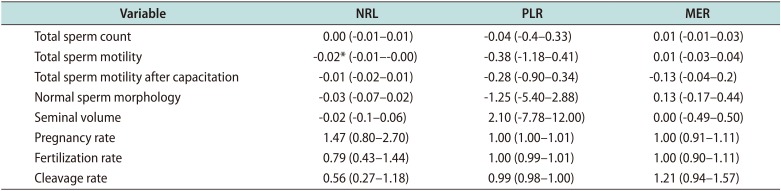
Table 3
Age-adjusted linear regression analysis between NLR, PLR, MER, seminal parameters and ICSI outcomes
![]()
Go to :
DISCUSSION
1. Main findings
Only a previous study explored the association between seminal parameters and NLR and PLR, showing how these inflammatory markers are not suitable to identify patients with abnormal seminal panel [10]. Our study, analysing also MER in addition to the common used NLR and PLR, confirmed that these scores are not significantly related with total sperm count, total sperm motility after capacitation and normal sperm morphology. Although weak, we have found an association between NLR and total sperm motility, with statistical significance (p<0.05).
2. Results in the context of previous studies
This data can be explained by previous studies, showing that systemic inflammation processes are associated with significant alteration in the seminal plasma [11]. In particular, Zhang et al [12] demonstrated that the inflammatory cytokines tumor necrosis factor (TNF)-alpha and interleukin-6 are able to disrupt the blood-testis barrier, reducing significantly sperm motility. Moreover, another study highlighted TNF-alpha as an influential factor of sperm count, sperm motility and normal sperm morphology among infertile male [13]. Additionally, in another trial, the serum amyloid A levels in peripheral blood were compared to sperm numbers, not finding a correlation [14]. Unfortunately, the technical difficulties and costs associated with these inflammation markers widely limit their use in routine clinical practice. In this respect, NLR, MER, and PLR count can be determined rapidly and inexpensively.
In the past years, NLR, MER, and PLR have been used in many fields to find inflammation status, such as in inflammatory diseases, cardiovascular diseases, infectious diseases, and various types of malignancies [1516171819]. Furthermore, a recent study explored the role of NLR and PLR in patients with dry eye disease, founding values higher in patients with dry eye than healthy subjects [20]. However, these inflammatory markers have been used very little in male infertility field. Only one study compared the NLR, MER, and PLR scores to the prediction of sperm retrieval in patients undergoing TESE, showing that these scores may be useful in the clinical practise [21]. However, the exact role of the inflammation systemic factors in the male seminal pathways remain actually uncertain.
The starting point of our research was the knowledge that oxidative mechanisms, resulting in the production of ROS, as well as the formation of neutrophil extracellular traps, can cause a serious damage on seminal plasma. The primary molecules that regulate and direct the inflammatory response are leukocytes. When the testicular tissue of patients with idiopathic male infertility with idiopathic infertility were examined, leukocyte infiltration was detected in more than 50% of patients [22]. There are several pathologies in the male reproductive tract that cause inflammation, such as ejaculatory duct obstruction, infections, testicular torsion, varicocele, and drug therapy. For these reasons, patients with these pathologies were excluded from the study. Additionally, the hypothalamic-pituitary-testis axis can be regulated by an increase of serum cytokines, that influence negatively the gonadal function and fertility [23]. Accordingly, we included in the study only participants with a normal hormonal serum values and without a clinical presentation of hypogonadism. Previous studies evaluated the impact of paternal age on the ARTs outcomes, but in the majority of them no statistically significant correlation was shown between FRs and advanced male age. Only two studies noted a negative influence in specific subgroups: Duran et al [24], comparing three male age groups, reported a statistically significant reduced FR with advancing paternal age only in ICSI cases. Luna et al [25] found a statistically significantly lower rate of fertilization by conventional insemination for male patients older than 50 years. In accordance with these data, also in our study a significantly correlation emerged between advanced paternal age and Group A (FR<70%; p=0.02). One hypothesis to explain the influence of male age on severe infertility and sperm fertilizing potential might be the extent of DNA damage beyond the point that could be repaired by the young oocyte [26]; however, the specifics of this mechanism have yet to be identified.
Moreover, it was demonstrated that systemic inflammation proved to affect male and female as well as woman fertility. Yldrm et al [27] investigated the relationship between primary ovarian failure and some systemic inflammation scores in female and found that NLR ratio in female with primary ovarian failure was statistically significantly lower than healthy subjects.
In our study, we analysed all couples in which the heterologous oocyte donation was necessary, in order to standardize the baseline female characteristics and to remove the possible confounding factors. Indeed, donor oocytes were obtained from young, healthy, and fertile female. In this way, no bias related to the female were present. Nevertheless, we also compared NLR, MER, and PLR to the overall PR, not showing any significant correlation, how expected, since this outcome may be influenced by multiple factors, like the increased age and the endometrial factor of the recipients. For this reason, we could not consider PR as the primary outcome.
3. Strengths and limitations
One limitation of this work, although it is the only in literature about this issue, is the retrospective single-centre design. A potential limitation was the lack of serum inflammation markers, such as C-reactive protein level, amyloid A protein level, or erythrocyte sedimentation rate, due to not being routinely investigated. Moreover, this study might be clinically important, but the low number of patients could explain the significant differences not founded. Nevertheless, further multicentre researches on the useful of different markers in the male infertility issue is required to confirm the results of our study.
4. Clinical applicability
Our aim was to evaluate if these inflammation scores can help the clinician to predict the success of the ART treatment. FR was usually defined as the number of fertilized oocytes (with two distinct pronuclei and two polar bodies after 17±1 hours after insemination) divided by the total number of oocytes retrieved. We took as a reference the key performance indicators established in Vienna Consensus [28] and in the previous Alpha Consensus meeting [29]. Therefore, FR greater or equal to 70% was considered optimal, and the less than 70% was suboptimal. However, we did not find any statistically significant differences between the FR, CR, PRs and these systemic inflammation-base prognostic scores.
On the other hand, there are many factors that can influence the inflammation status of patients. Although the peripheral blood sample was made in absence of concomitant baseline pathologies, it may exist many confounding factors. Moreover, the reproductive potential of male depends by many aspects, not alone by routine seminal parameters. Thus, systemic inflammation can be one cause and may have a key role in male infertility, yet throughout unknown mechanisms. For these reasons, we may suggest to improve current research on identify other useful inflammation markers that could be related to infertility or even with ICSI success.
Go to :
 XML Download
XML Download