

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
MATERIALS AND METHODS
1. Inclusion/exclusion criteria
1) Primary outcomes
2) Secondary outcomes
2. Search strategy
3. Study selection and data extraction
4. Assessment of methodological quality
5. Data analysis
RESULTS
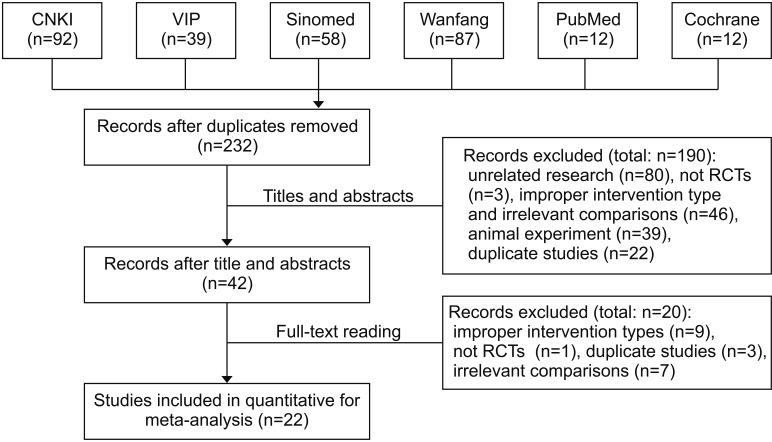
1. Study selection
2. Description of studies
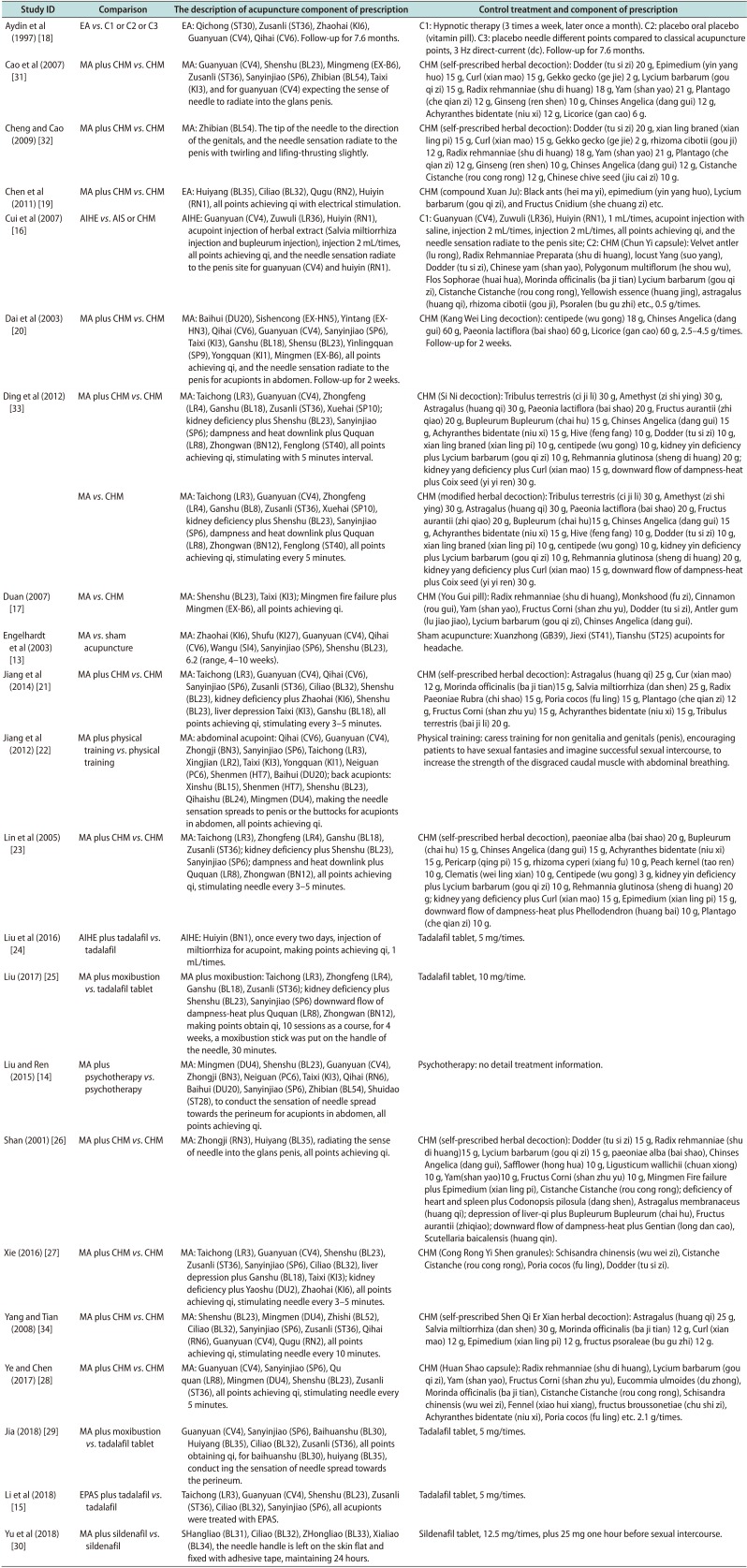
Table 1
Characteristics of 22 the included randomized trials

| Study ID | Samplea | Age (y)b | Type of ED | Intervention | Control | Duration of treatment (wk)c | Outcome measure |
|---|---|---|---|---|---|---|---|
| Aydin et al (1997) [18] | T: 15, C1: 15, C2: 15, C3: 15 | T: 36.75±10.43, C1: 38.4±10.75, C2: 35.1±10.46, C3: 37.1±11.32 | Psychogenic | EA, 3 Hz direct-current (dc), 20 minutes, twice a week | C1: hypnotic therapy, (3 times a week, later once a month) | T: 6, C1: 6, C2: 6, C3: 6 | Satisfaction of selfassessment rate, adverse effects |
| C2: oral placebo (vitamin pills) | |||||||
| C3: sham acupuncture (non-acupuncture points) 3 Hz dc, 20 minutes, twice a week | |||||||
| Cao et al (2007) [31] | T: 36, C: 18 | T: 25–58, C: 26–59 | NR | MA plus control, 30 minutes, once daily | CHM (self-prescribed herbal decoction), twice daily | 8 | Markedly improved on erectile function rate |
| Cheng and Cao (2009) [32] | T: 32, C: 32 | T: 20–56, C: 21–54 | NR | MA plus control, 30 minutes, once daily | CHM (self-prescribed herbal decoction), twice daily | 4 | Markedly improved on erectile function rate |
| Chen et al (2011) [19] | T: 61, C: 62 | T: 27.62, C: 27.58 | Psychogenic | EA plus control, with density wave, 30 minutes, once daily | CHM (compound Xuan Ju), 3 capsules, 3 times daily | 4 | Satisfaction of selfassessment rate, IIEF-5 scores |
| Cui et al (2007) [16] | T: 50, C1: 50, C2: 50 | T: 20–69, C1: 20–69, C2: 20–69 | Psychogenic or arterial supply insufficiency | Salvia miltiorrhiza injection and bupleurum injection once every 2 days | C1: acupoint injection with saline, once every 2 days | 3 | Markedly improved on erectile function rate, IIEF-5 scores |
| C2: CHM (Chun Yi capsule), 0.5 g/times, 3 times daily | |||||||
| Dai et al (2003) [20] | T: 44, C: 41 | T: 35.75±3.17, C: 36.24±4.12 | Psychogenic | MA plus control, 30 minutes, once daily | CHM (Kang Wei Ling decoction), 2.5–4.5 g/times, twice daily | 4 | Markedly improved on erectile function rate |
| Ding et al (2012) [33] | T1: 88, C: 44 | T: 41.3±8.1, C: 39.1±6.7 | Psychogenic | MA plus control, 30 minutes, once daily | CHM (Si Ni decoction), 3 times daily | 4–8 | Markedly improved on erectile function rate, penile erection angle |
| T2: 44, C: 44 | T: 38.3±7.4, C: 39.1±6.7 | Psychogenic | MA, 30 minutes, once daily | CHM (modified herbal decoction), 3 times daily | 4–8 | Markedly improved on erectile function rate, penile erection angle | |
| Duan (2007) [17] | T: 30, C: 30 | T: 27–55, C: 29–52 | Psychogenic or arterial supply insufficiency | MA, 30 minutes, once daily | CHM (You Gui pill), one pill, twice daily | 4 | Markedly improved on erectile function rate |
| Engelhardt et al (2003) [13] | T: 10, C: 11 | T: 38.9, C: 38.9 | Psychogenic | MA, 20 minutes, once or twice weekly | Sham acupuncture against headache acupoint, 20 minutes, once or twice weekly | 6.2 (4–10) | Satisfaction of selfassessment rate, IIEF scores, adverse effects |
| Jiang et al (2014) [21] | T: 64, C: 64 | T: 21–64, C: 22–65 | Psychogenic | MA plus control, 30 minutes, once daily | CHM (self-prescribed herbal decoction), twice daily | 3–5 | Cure rate, IIEF scores |
| Jiang et al (2012) [22] | T: 51, C: 51 | T: 28.73±3.27, C: 27.67±4.12 | Psychogenic | MA plus control, 30 minutes, once daily | Physical training, 5–15 minutes each time, 12 times from 15 days | 4 | Satisfaction of selfassessment rate |
| Lin et al (2005) [23] | T: 64, C: 32 | T: 38.3±8.1, C: 39.1±6.7 | Psychogenic | MA plus control, 30 minutes, once daily | CHM (self-prescribed herbal decoction), twice daily | 4–8 | Markedly improved on erectile function rate, penile erection angle |
| Liu et al (2016) [24] | T: 32, C: 30 | T: 32, C: 30 | Psychogenic | AIHE plus control, injection 1 mL/time, once every 2 day | Tadalafil tablet, 5 mg/times, once daily | 12 | Cure rate, IIEF scores |
| Liu (2017) [25] | T: 31, C: 31 | T: 42.68±2.35, C: 42.56±2.45 | Psychogenic | MA with moxibustion plus control, MA: 30 minutes, once daily | Tadalafil tablet, 10 mg/times, 3 times daily | 4 | Cure rate, adverse effects |
| Liu and Ren (2015) [14] | T: 30, C: 30 | T: 47.4±6.01, C: 47.8±6.51 | ED with type-2 diabetes | MA plus control, 20 minutes, once daily | Psychotherapy and exercise | 8 | Cure rate, IIEF scores |
| Shan (2001) [26] | T: 60, C: 30 | T: 43.6, C: 43.6 | NR | MA plus control, 20 minutes, once daily | CHM (self-prescribed herbal decoction), twice daily | 12 | Markedly improved on erectile function rate |
| Xie (2016) [27] | T: 40, C: 40 | T: 42.8±8.35, C: 43.19±8.07 | Psychogenic | MA plus control, 30 minutes, once daily | CHM (Cong Rong Yi Shen granules), twice daily | 16 | Cure rate, IIEF scores, adverse effects |
| Yang and Tian (2008) [34] | T: 20, C: 20 | T: 40, C: 40 | NR | MA plus control, 30 minutes, once daily | CHM (self-prescribed Shen Qi Er Xian herbal decoction), twice daily | 4–8 | Satisfaction of selfassessment rate |
| Ye and Chen (2017) [28] | T: 20, C: 20 | T: 34.15±6.43, C: 36.25±5.25 | Psychogenic | MA plus control, 30 minutes, once daily | CHM (Huan Shao capsule), 2.1 g/times, 3 times daily | 4 | Cure rate, IIEF scores |
| Jia (2018) [29] | T: 20, C: 20 | T: 40.15±1.68, C: 40.86±1.91 | Psychogenic | MA with moxibustion plus control, 30 minutes, once daily | Tadalafil tablet, 5 mg/times, once daily | 3 | Cure rate, IIEF scores, adverse effects |
| Li et al (2018) [15] | T: 45, C: 45 | T: 45.26±4.17, C: 46.14±4.51 | ED with type-2 diabetes | EPAS plus control, 4 min/time for one acupoint, total 24 minutes, once daily | Tadalafil tablet, 5 mg/times, once daily | 4 | Cure rate, IIEF scores, adverse effects |
| Yu et al (2018) [30] | T: 20, C: 20 | T: 34.15±6.43, C: 36.25±5.25 | Psychogenic | MA plus control, 30 minutes, once daily | Sildenafil tablet, 12.5 mg/times, twice daily | 6 | Cure rate, IIEF scores |
“Cured” refers to patients who reported that their clinical symptoms disappeared, they had no problem with sexual activity, and/or with International Index of Erectile Function (IIEF-5) score was ≥22 [31]. ‘Markedly improved on erectile function’ refers to that all the three below items were met: the self-report disappearance of clinical symptoms, the erection angle of penis is more than 90 degrees in sexual activity, and the success rate of sexual intercourse is over 75%.
ED: erectile dysfunction, T: treatment group, C: control group, NR: not reported, EA: electro acupuncture, MA: manual acupuncture, AIHE: acupoint injection of herbal extract, EPAS: moderate—frequency electrical pulse acupoint stimulation, CHM: Chinese herbal medicine.
aValues are presented as number only. bValues are presented as mean±standard deviation, range, or mean only. cValues are presented as mean only, range only, or median (range).
![]()
3. Description of therapeutic regimen
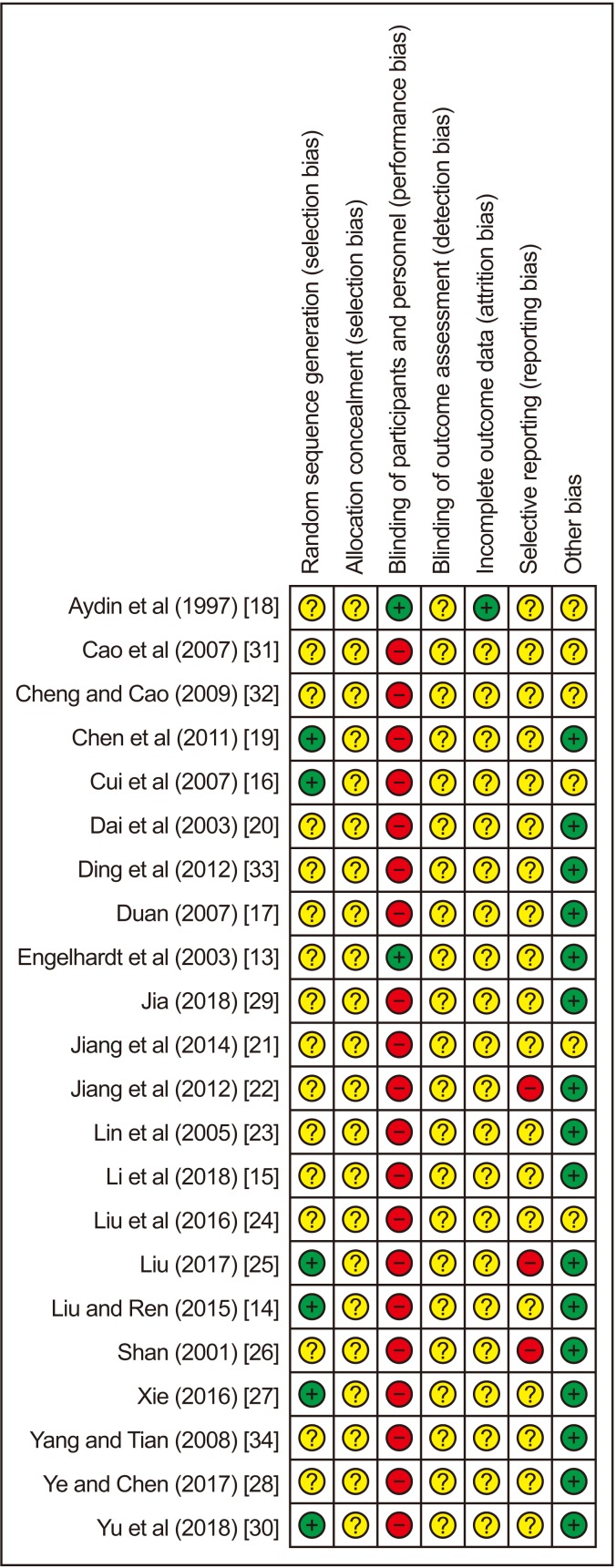
4. Assessment of risk of bias
5. Effect estimates
Table 2
Effect estimates of included 22 trials

| Outcome and comparison | Study | Participant | Effect estimate (95% CI) REM | p-value | Study ID |
|---|---|---|---|---|---|
| Electronic acupuncture versus sham acupuncture with electrical stimulation | |||||
| Satisfaction of self-assessment rate | 1 | 60 | RR 1.50 (0.71–3.16) | - | Aydin et al (1997) [18] |
| Manual acupuncture versus sham acupuncture | |||||
| Satisfaction of self-assessment rate | 1 | 60 | RR 7.53 (1.13–50.00) | - | Engelhardt et al (2003) [13] |
| Acupuncture plus tadalafil tablet versus tadalafil tablet | |||||
| Cure rate | 2 | 152 | RR 1.31 (1.00–1.71), I2=0% | 0.48 | Liu et al (2016) [24], Li et al (2018) [15] |
| IIEF-5 score | 2 | 152 | MD 5.38 (4.46–6.29), I2=0% | 0.04 | Liu et al (2016) [24], Li et al (2018) [15] |
| Acupuncture plus sildenafil tablet versus sildenafil tablet | |||||
| Cure rate | 1 | 70 | RR 3.00 (0.65–13.86) | - | Yu et al (2018) [30] |
| IIEF-5 score | 1 | 70 | MD 3.23 (2.12–4.34) | - | Yu et al (2018) [30] |
| Manual acupuncture plus moxibustion versus tadalafil tablet | |||||
| Cure rate | 2 | 102 | RR 1.40 (0.74–2.66), I2=0% | 0.3 | Liu (2017) [25], Jia (2018) [29] |
| IIEF-5 score | 1 | 40 | MD 1.15 (1.37–0.93) | - | Jia (2018) [29] |
| Acupuncture versus herb medicine | |||||
| Markedly improved on erectile function rate | 2 | 148 | RR 1.40 (0.42–4.69), I2=46%, | 0.18 | Ding et al (2012) [33], Duan (2007) [17] |
| IIEF-5 score | 1 | 100 | MD 4.00 (3.66–4.34) | - | Cui et al (2007) [16] |
| Acupuncture point injection of herbal extracts versus oral herbal medicine | |||||
| IIEF-5 score | 1 | 100 | MD 4.0 (3.66–4.34) | - | Cui et al (2007) [16] |
| Markedly improved on erectile function rate | 1 | 100 | RR 1.94 (0.69–5.43) | - | Cui et al (2007) [16] |
| Acupuncture plus herbal medicine versus herbal medicine alone | |||||
| Cure rate | 2 | 168 | RR 1.36 (1.12–1.65), I2=0% | 0.77 | Jiang et al (2014) [21], Ye and Chen (2017) [28] |
| Markedly improved on erectile function rate | 7 | 601 | RR 1.68 (1.31–2.15), I2=0% | 0.90 | Cao et al (2007) [31], Cheng and Cao (2009) [32], Dai et al (2003) [20], Ding et al (2012) [33], Lin et al (2005) [23], Shan (2001) [26], Xie (2016) [27] |
| Satisfaction of self-assessment rate | 2 | 163 | RR 1.67 (0.64–4.36), I2=75% | 0.3 | Chen et al (2011) [19], Yang and Tian (2008) [34] |
| IIEF-5 score | 3 | 331 | No pooled data of trials for I2=95% | <0.05 | Chen et al (2011) [19], Jiang et al (2014) [21], Xie (2016) [27] |
| Erectile angle | 2 | 228 | MD 6.73° (4.10–9.36), I2=0% | 0.94 | Ding et al (2012) [33], Lin et al (2005) [23] |
| Manual acupuncture plus physical therapy versus physical therapy | |||||
| Cure rate | 1 | 102 | RR 1.56 (0.99–2.43) | - | Jiang et al (2012) [22] |
| IIEF-5 score | 1 | 60 | MD 2.90 (2.59–3.21) | - | Liu and Ren (2015) [14] |
![]()
1) Acupuncture versus sham acupuncture
2) Acupuncture plus western medicine versus western medicine
3) Manual acupuncture plus moxibustion versus tadalafil tablet
4) Acupuncture versus herbal medicine
5) Acupuncture plus herbal medicine versus herbal medicine alone
6) Acupuncture plus psychological therapy versus psychological therapy
6. Adverse events
7. Overall quality of evidence by GRADE
Table 3
Summary of main findings of RCTs on acupuncture for erectile dysfunction

GRADE Working Group grades of evidence. High quality: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
RCT: randomized controlled trial, CI: confidence interval, IIEF: International Index of Erectile Function, RR: risk ratio, N/A: not applicable, MD: mean difference.
aRisk of bias: All the trials had high risk of performance bias for not blinding the participants. Methodological quality of these trials was graded as “high risk of bias,” due to the design of comparison (acupuncture therapy versus conventional medications) is difficult to blind personnel and participants. The trials also had unclear risk of performance bias for not reporting blinding the outcome assessor. bInconsistency; There is significantly statistical heterogeneity indicating by I2 value. cImprecision: For dichotomous outcomes, the total number of events is less than 300, for continuous outcomes, the total population size is less than 400 or pooled results included no effects. dIndirectness. For outcomes of satisfaction of self-assessment rate, markedly improved on erectile function rate, and erectile angle. This was not internationally applied outcome measures. ⊕: Very low quality of the evidence; ⊕⊕: Low quality of the evidence.
![]()
 XML Download
XML Download