

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
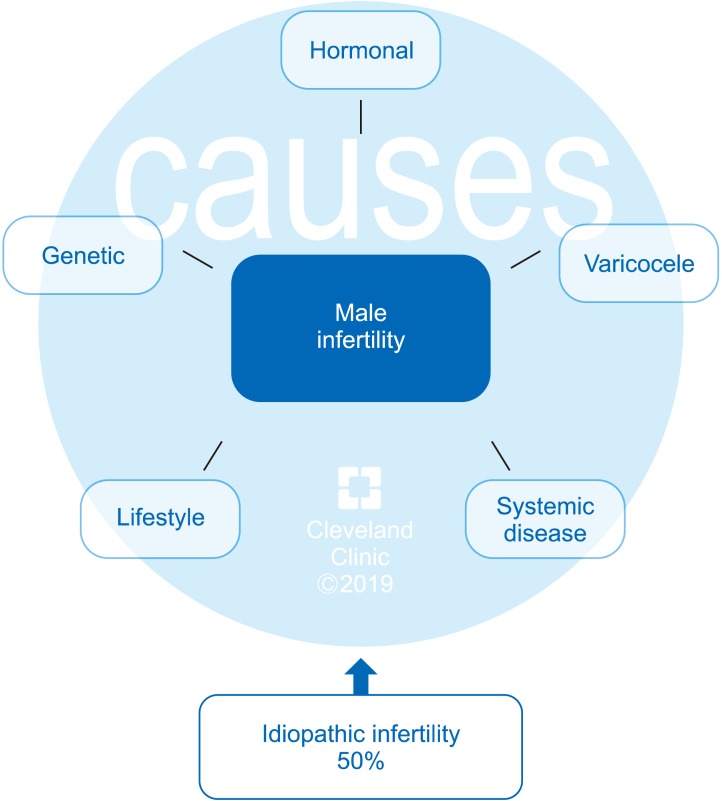
Natural conception is a complex process that is achieved in only 76% to 85% of couples within 12 months of regular unprotected intercourse [12345]. The International Committee for Monitoring Assisted Reproductive Technologies (ICMART) defines infertility as the inability to conceive after 1 year of regular, unprotected intercourse [67]. The World Health Organization estimates that nearly 190 million people struggle with infertility worldwide and the number of couples seeking medical assistance is steadily rising [89]. Among couples unable to conceive, infertility is partially or wholly attributable to a male factor in approximately 50% of cases (Fig. 1) [101112]. A variety of conditions can affect male reproductive potential to different extent and they often coexist (Fig. 2) [13141516171819]. Paradoxically, on routine assessment, the precise etiology of male factor infertility remains undefined in 30% to 50% of patients, who are subsequently classified as having idiopathic male infertility [202122]. Unlike unexplained male infertility with its normal semen parameters, idiopathic male infertility is diagnosed in the presence of altered semen characteristics without an identifiable cause and the absence of female factor infertility [23].
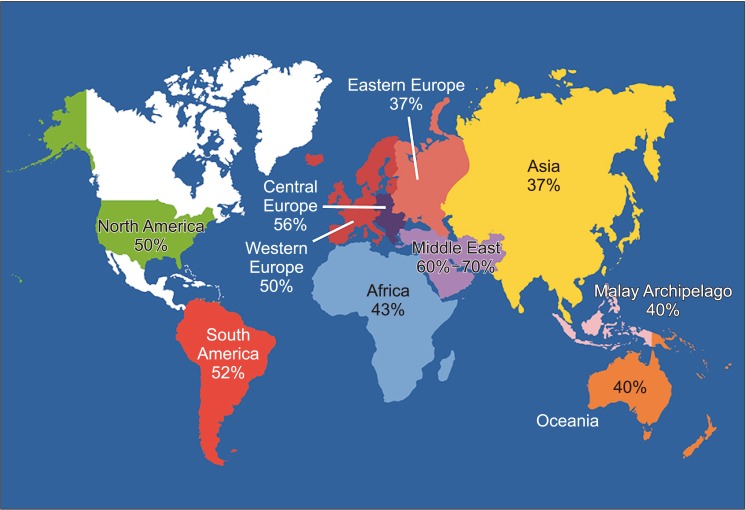 | Fig. 1World map containing percentages of infertility cases per region that are due to male factor involvement among regions studied. Asia includes all of Russia. Data from Agarwal et al (Reprod Biol Endocrinol 2015;13:37) [10].
|
Go to : 
THE CONCEPT OF MALE OXIDATIVE STRESS INFERTILITY (MOSI)
There is overwhelming evidence that oxidative stress (OS) plays a significant role in the etiology of male infertility [24252627282930]. Seminal reactive oxygen species (ROS) are produced mainly by leukocytes or abnormal and immature spermatozoa, and are a natural byproduct of oxidative metabolic pathways as well as cytosolic and plasma membrane oxidases [31323334]. ROS are also a natural byproduct of adenosine triphosphate production within sperm cell mitochondria [35]. Small quantities of ROS are required to ensure normal cellular physiological functions, including spermatogenesis and various sperm functions preceding fertilization, such as capacitation and acrosome reaction [32363738]. When ROS levels increase to a pathological level, the body uses dietary and endogenously produced antioxidants to bring the system back to homeostasis [39]. An imbalance between these two opposing forces, in which ROS outweigh antioxidants, can result in OS, which can negatively affect fertility via a number of pathways. OS interferes with capacitation and may cause sperm membrane and DNA damage, thereby affecting the sperm's potential to fertilize an egg and generate a healthy embryo [32404142434445]. Also, OS can trigger formation of genotoxic and mutagenic byproducts in the sperm that may increase the risk of disease in the offspring [46]. Depending on the assay methodology used, recent literature suggests that 30% to 80% of infertile men have elevated seminal ROS levels, a potentially treatable condition [28304447484950515253545556]. A similarly high incidence of OS was reported in a recent clinical trial, with 83.8% (124 of 148 cases) of idiopathic infertile men having positive seminal oxidation-reduction potential (ORP), a measure of ROS-antioxidant discrepancy [unpublished data].
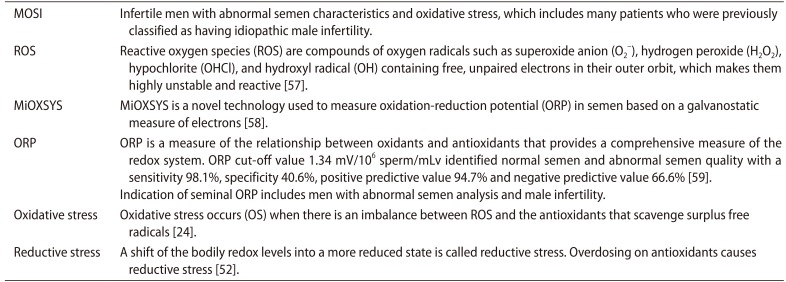
Male reproductive potential cannot be adequately assessed if seminal OS is overlooked. However, there is currently no consensus concerning either the preferred method to measure OS in the clinical setting nor the diagnostic terminology to define this condition. Therefore, we propose the term Male Oxidative Stress Infertility, or MOSI, as a novel descriptor for infertile men with abnormal semen characteristics and OS, which includes many patients who were previously classified as having idiopathic male infertility (Appendix) [2452575859]. Based on several epidemiologic studies, OS may be present in about 56 million males complaining of infertility, two-thirds of whom are considered to have MOSI (https://www.nichd.nih.gov/health/topics/menshealth/conditioninfo/infertility) (Fig. 3) [3060616263]. In men with normal semen characteristics who are part of couples experiencing unexplained infertility, the role of OS is not well defined. In our experience, 29.4% (10 of 34) of men in this group have leukocytospermia as opposed to 12.2% (77 of 629) in the general population of men with infertility [unpublished data].
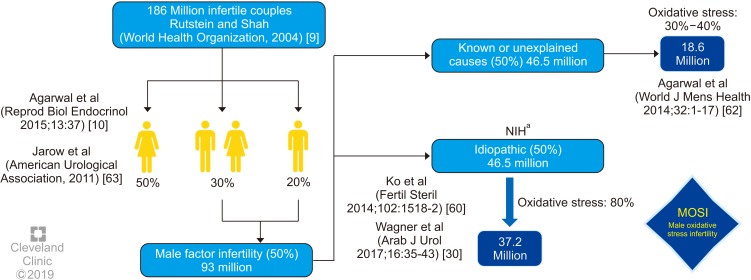 | Fig. 3Worldwide incidence of MOSI in infertile men. aNational Institutes of Health (NIH) (https://www.nichd.nih.gov/health/topics/menshealth/conditioninfo/infertility) [61], Agarwal et al (2014) [60], Jarow et al (2011) [63].
|
Go to :
DIAGNOSIS OF MALE OXIDATIVE STRESS INFERTILITY (MOSI)
Conventional semen analysis was introduced about a century ago and remains the most widely used test for measuring sperm production and quality. In recent years, it has become clear that conventional semen analysis alone is not an adequate surrogate measure of male fecundity [64], as it is plagued with critical shortcomings such as poor reproducibility, subjectivity, and poor prediction of fertility [65666768]. Given the limited clinical utility of conventional semen analysis and the pathological consequences and ubiquity of OS among the subfertile male population, we propose the incorporation of ORP as a useful clinical biomarker for MOSI in men with abnormal semen analysis and male infertility [5869707172]. ORP may be used to measure the levels of reductants (antioxidants) and oxidants in a variety of biological fluids [73] and could become an adjunct component of semen analysis due to its robust association with impaired sperm function. A number of assays are available to measure OS including chemiluminescence for ROS, total antioxidant capacity for antioxidants, and the malondialdehyde assay for post-hoc damage from lipid peroxidation [747576]. Though useful, these tests are difficult to incorporate into routine use because they are expensive, complex, and time-sensitive, and may also require complex instrumentation, large and neat sample volumes, and extensive technical training (Table 1) [76]. Additionally, assay results do not correlate with one another and provide only a single marker of OS-either oxidant levels, antioxidant levels, or post-hoc damage [77].
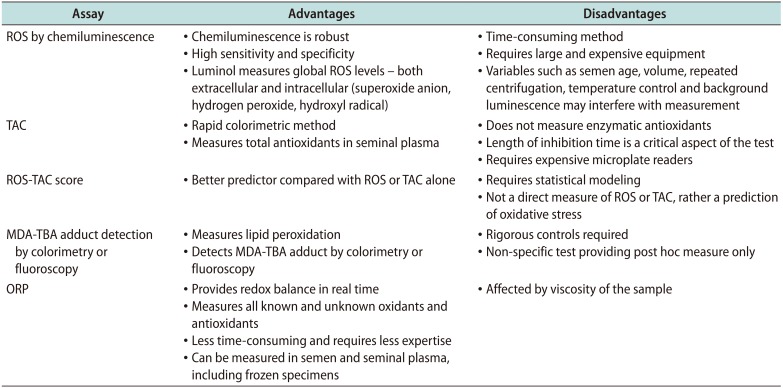
Table 1
Advantages and disadvantages of commonly used techniques to measure seminal oxidative stress
ROS: reactive oxygen species, TAC: total antioxidant capacity, MDA: malondialdehyde, TBA: thiobarbituric acid, ORP: oxidation-reduction potential. Data from Agarwal et al (Ther Adv Urol 2016;8:302-18) [76].
![]()
To date, measurement of ROS in semen is not often utilized as, depending on the method for ROS assessment, it may be prone to intra- and inter-laboratory variability, high turnaround time and high costs [586978]. The advent of new technologies that rapidly detect seminal OS through the assessment of ORP in a reproducible manner using a bench-top analyzer can allow for an accurate and cost-effective diagnosis of MOSI [767879]. The Male Infertility Oxidative System (MiOXSYS) is a recently developed assay for the assessment of ORP [69]. The ORP test is novel in the area of infertility and is based on a galvanostatic measure of electrons. MiOXSYS has been developed for easy and quick measurement of ORP in semen [80]. Several studies have validated the reproducibility and reliability of the MiOXSYS in measuring ORP levels in semen samples from patients being evaluated for male infertility [58697181]. More importantly, ORP levels have been shown to be significantly negatively correlated with sperm concentration, sperm motility, normal morphology and total motile count [72]. ORP levels are also significantly positively correlated with sperm DNA fragmentation (SDF) [727981], although normal levels of SDF do not exclude the presence of OS. At a cutoff value of 1.34 (mV/106 sperm/mL), ORP may be used to differentiate between normal and abnormal semen quality in infertile men with 98.1% sensitivity, 40.6% specificity, 94.7% positive predictive value, and 66.6% negative predictive value [585969] (Fig. 4).
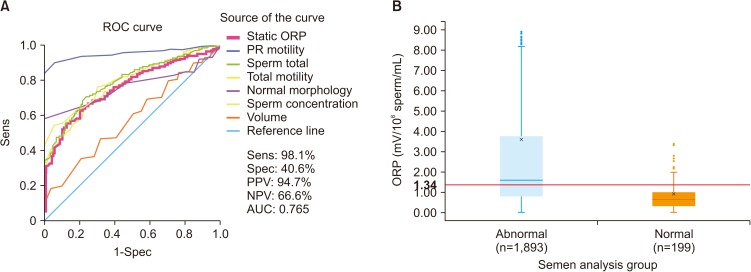 | Fig. 4(A) A receiver operating characteristic (ROC) curve was used to identify the oxidation-reduction potential (ORP) (mV/106 sperm/mL) cutoff that best predicted normal and abnormal semen parameters based on sensitivity (Sens), specificity (Spec), positive predictive value (PPV), negative predictive value (NPV), and area under the curve (AUC). (B) Distribution of ORP in patients with at least one abnormal semen parameter versus patients with normal semen parameters, showing the established cutoff value of 1.34 mV/106 sperm/mL. Data from Agarwal et al (Asian J Androl 2019 [in press]) [59].
|
Among infertile men, higher ORP levels are observed in cases with abnormal semen parameters versus normal parameters (Fig. 5A, 5B). Analysis of data of 3,966 patients at Hamad Medical Corporation, Doha, Qatar, revealed statistically significant negative correlations between ORP and normal sperm morphology (r=−0.529, p<0.0001), progressive motility (r=−0.463, p<0.0001), and sperm concentration (r=−0.844, p<0.0001). The difference in ORP between normozoospermic (mean: 1.14±0.97 mV/106 sperm/mL; median: 0.86 mV/106 sperm/mL) and non-normozoospermic (mean: 5.65±11.34 mV/106 sperm/mL; median: 2.04 mV/106 sperm/mL) patients was also significant (p<0.0001) (Fig. 5B). Fig. 5C depicts ORP values of asthenozoospermic (mean: 5.63±11.36 mV/106 sperm/mL; median: 2.03 mV/106 sperm/mL) versus non-asthenozoospermic patients (mean: 1.79±3.80 mV/106 sperm/mL; median: 0.92 mV/106 sperm/mL) [unpublished data].
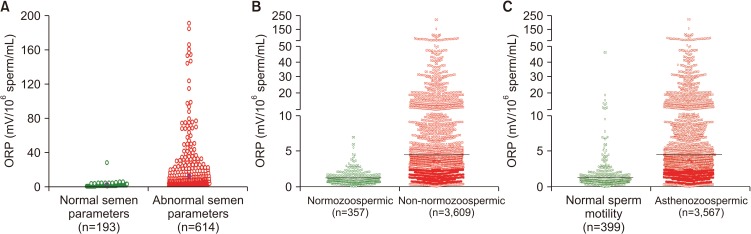 | Fig. 5Distribution of oxidation-reduction potential (ORP) values in the infertile men with normal and abnormal semen parameters. (A) Data from Cleveland Clinic, Cleveland OH, USA (n=807); (B) Data from Hamad Medical Corporation, Doha, Qatar (n=3,966); (C) Data of asthenozoospermic patients from Hamad Medical Corporation, Doha, Qatar (n=3,966).
|
Go to :
MANAGEMENT AND TREATMENT OF MALE OXIDATIVE STRESS INFERTILITY (MOSI)
Despite significant advances in the diagnosis and management of male infertility, there are no evidencebased treatment guidelines available for idiopathic male infertility. Understandably, it is difficult to develop an evidence-based approach for a condition with an unclear etiology. A survey among members of the American Urological Association (AUA) indicated that two-thirds of clinicians use empirical medical therapy (EMT) such as selective estrogen receptor modulators, aromatase inhibitors, and gonadotropins to treat idiopathic male factor infertility [82]. While the role of hormonal therapy in men with an identified abnormality such as hypogonadotropic hypogonadism is well-defined [83], endocrine imbalance is responsible for approximately 10% of all known causes of infertility [21]. The literature remains inconclusive and controversial regarding off-label EMTs for men with idiopathic infertility [208284858687], especially in light of their cost and side effects (Table 2). Although there are several small studies that provide support for pharmacological EMT to treat idiopathic male infertility, there is a lack of robust placebo-controlled trials demonstrating improved live birth outcomes [87888990].
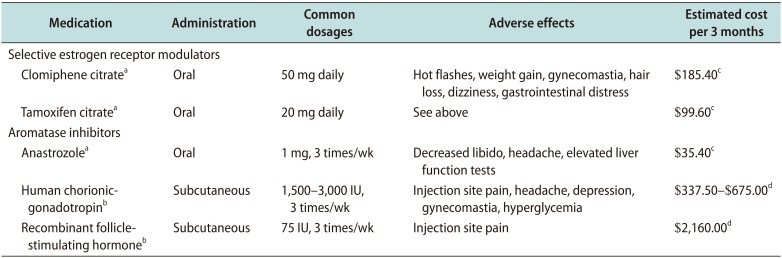
Table 2
Empiric medical treatment for idiopathic male infertility (ICD10 Code: Z31.41)
![]()
For the vast majority of infertile men with no underlying endocrine, bacterial, genetic or anatomical causes of infertility, an alternative approach may be to shift from administering EMTs to identifying potential sources of MOSI and mitigating the sequela. The human body produces endogenous antioxidants in an effort to prevent the damage caused by ROS [9192], but this response is not always adequate, resulting in OS. Several studies have shown that exogenous antioxidants have the capacity to counteract oxidative damage or OS, improving both sperm motility and DNA integrity for infertile men with OS (Table 3) [878889909193949596979899100101102103104105106107108109110111]. Indeed, many oral formulations of antioxidants are readily available in the market and are commonly used to treat men with infertility. However, there is growing awareness that the indiscriminate use of antioxidants may paradoxically exacerbate sperm cell damage in men without elevated MOSI by inducing a state of reductive stress [52112]. In order to prevent the inappropriate use of antioxidants, clinical guidelines outlining the effective diagnosis and treatment of MOSI are critical. Several clinical trials and systemic reviews involving the use of various combinations of antioxidants (L-carnitine, selenium, N-acetyl-cysteine, Coenzyme Q10, ubiquinol, vitamin E, vitamin C, and lycopene) in infertile men have reported beneficial effects of antioxidants on sperm concentration, motility, and DNA integrity (Table 4) [113114115116117118119120]. Preliminary results from a 2018 clinical trial involving 148 idiopathic infertile men indicated that intake of oral antioxidants for a period of three months significantly increased sperm concentration (36%, p<0.0001), progressive motility (100%, p<0.0001), and motility (12%, p=0.0033). Moreover, a significant decrease in ORP (39%, p<0.0001) and SDF (20%, p=0.0002) was observed post-treatment [unpublished data]. These beneficial changes in semen quality have been reported to improve the chance of natural conception in several but not all studies [53121]. This benefit could be augmented, and harm prevented, by directing therapy through measuring and monitoring seminal ORP [113114115116122123].

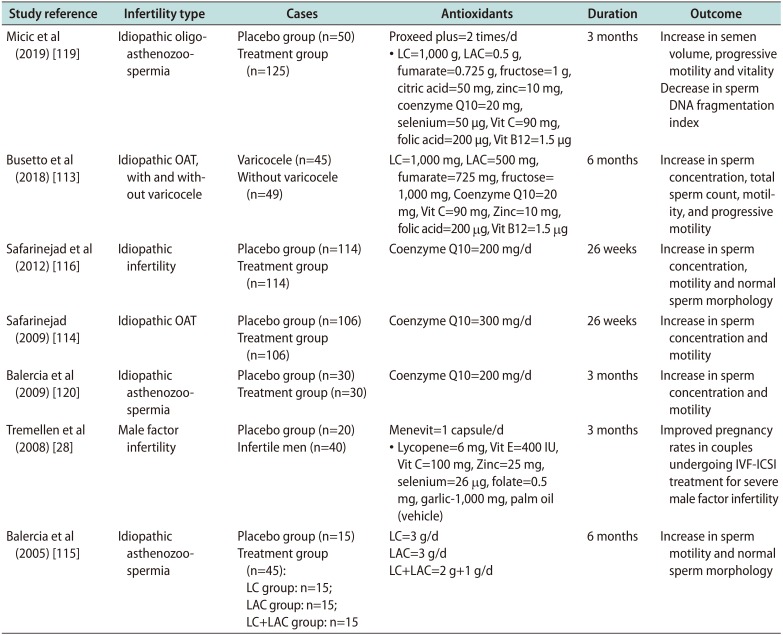
Table 3
Antioxidant classification in relation to its action on sperm characteristics
| Type | Function | References |
|---|---|---|
| Enzymatic: | ||
| Superoxide dismutase | First line defense antioxidants | [9495] |
| Catalase | First line defense antioxidants | [5496] |
| Glutathione peroxidase | Scavenges lipid peroxides and hydrogen peroxide | [9798] |
| Glutathione reductase | Scavenges lipid peroxides and hydrogen peroxide | [99] |
| Non enzymatic: | ||
| Vitamin C | Neutralizes free radicals | [100101] |
| Vitamin E | Neutralizes free radicals | [102103] |
| Ferritin and carnitines | Neutralizes free radicals and acts as an energy source | [126] |
| Coenzyme Q10 | In its reduced form, scavenges free radicals intermediate in mitochondrial electron transport system | [104] |
| Transferrin | Sperm vitality, DNA integrity and OS homeostasis | [105] |
| Zinc | Formation of free oxygen radicals and sperm chromatin stability | [106] |
| Selenium | Sperm motility and OS homeostasis | [107] |
| N-acetyl L-cysteine | Free radical scavenging activity | [108109] |
| L-arginine | Formation of free oxygen radicals | [110] |
| Folic acid | Sperm DNA integrity | [111] |
![]()
Table 4
Effect of antioxidants on male infertility: Double blind placebo controlled studiesa
| Study reference | Infertility type | Cases | Antioxidants | Duration | Outcome |
|---|---|---|---|---|---|
| Micic et al (2019) [119] | Idiopathic oligoasthenozoospermia | Placebo group (n=50) | Proxeed plus=2 times/d | 3 months | Increase in semen volume, progressive motility and vitality |
| Treatment group (n=125) | • LC=1,000 g, LAC=0.5 g, fumarate=0.725 g, fructose=1 g, citric acid=50 mg, zinc=10 mg, coenzyme Q10=20 mg, selenium=50 µg, Vit C=90 mg, folic acid=200 µg, Vit B12=1.5 µg | Decrease in sperm DNA fragmentation index | |||
| Busetto et al (2018) [113] | Idiopathic OAT, with and without varicocele | Varicocele (n=45) | LC=1,000 mg, LAC=500 mg, fumarate=725 mg, fructose= 1,000 mg, Coenzyme Q10=20 mg, Vit C=90 mg, Zinc=10 mg, folic acid=200 μg, Vit B12=1.5 μg | 6 months | Increase in sperm concentration, total sperm count, motility, and progressive motility |
| Without varicocele (n=49) | |||||
| Safarinejad et al (2012) [116] | Idiopathic infertility | Placebo group (n=114) | Coenzyme Q10=200 mg/d | 26 weeks | Increase in sperm concentration, motility and normal sperm morphology |
| Treatment group (n=114) | |||||
| Safarinejad (2009) [114] | Idiopathic OAT | Placebo group (n=106) | Coenzyme Q10=300 mg/d | 26 weeks | Increase in sperm concentration and motility |
| Treatment group (n=106) | |||||
| Balercia et al (2009) [120] | Idiopathic asthenozoospermia | Placebo group (n=30) Treatment group (n=30) | Coenzyme Q10=200 mg/d | 3 months | Increase in sperm concentration and motility |
| Tremellen et al (2008) [28] | Male factor infertility | Placebo group (n=20) | Menevit=1 capsule/d | 3 months | Improved pregnancy rates in couples undergoing IVF-ICSI treatment for severe male factor infertility |
| Infertile men (n=40) | • Lycopene=6 mg, Vit E=400 IU, Vit C=100 mg, Zinc=25 mg, selenium=26 μg, folate=0.5 mg, garlic-1,000 mg, palm oil (vehicle) | ||||
| Balercia et al (2005) [115] | Idiopathic asthenozoospermia | Placebo group (n=15) | LC=3 g/d | 6 months | Increase in sperm motility and normal sperm morphology |
| Treatment group (n=45): LC group: n=15; LAC group: n=15; LC+LAC group: n=15 | LAC=3 g/d | ||||
| LC+LAC=2 g+1 g/d |
OAT: oligoasthenoteratozoospermia, LC: L-carnitine, LAC: L-acetylcarnitine, Vit: vitamin, IVF-ICSI: in vitro fertilization/intracytoplasmic sperm injection. aOnly double blind placebo control studies on idiopathic male infertility patients were included. Except for three studies (94, 96, and 142), others used a combination of antioxidant supplements for a period of 3 to 6 months.
![]()
Identifying and treating MOSI in cases where the use of assisted reproductive technology (ART) is indicated is especially important, as many of the sperm preparation and handling methods used during ART may induce OS, further aggravating the negative impact of MOSI [124125]. In couples undergoing ART, diagnosis of MOSI and subsequent antioxidant therapy may improve ART success [122126127]. Additionally, there is emerging evidence that antioxidant therapy may improve pregnancy outcomes in couples with recurrent pregnancy loss [128]. Evidence-based guidelines should provide recommendations on ways to best manage other causes of OS, including lifestyle modifications (improved diet, smoking cessation, exercise, and weight loss), treatment of clinically relevant varicoceles, and treatment of male accessory gland infection (MAGI) as well as other inflammatory pathologies linked with MOSI (Fig. 3). The treatment of MAGI with antibiotics, and the decrease in the numbers of ROS-producing seminal leukocytes using anti-inflammatories are likely to add benefit in combination with neutralization of ROS by antioxidant therapy [129130131132]. Treatment success and adherence for the above conditions can be monitored by measuring seminal ORP, as well.
The diagnosis and management of idiopathic male infertility is an integral component of comprehensive sexual and reproductive health services. Idiopathic male infertility can be an emotional burden and financial strain for couples. Current treatment protocols for male infertility are not evidence-based and have the potential risk of complications and increased healthcare-related expenditures [2084]. MOSI provides clinicians and patients with a diagnostic classification to guide future research and treatment, while simultaneously reducing apprehension and uncertainty for many couples. A recent consensus guideline by the European Society for Human Reproduction & Embryology (ESHRE) concluded that there is currently insufficient evidence to support the use of antioxidants for male infertility due to lack of a standardized measure of OS and inconsistent selection of eligible patients across studies [133]. MOSI diagnosis combined with ORP monitoring may provide a more targeted, reliable approach for using antioxidant therapy in both research and practice.
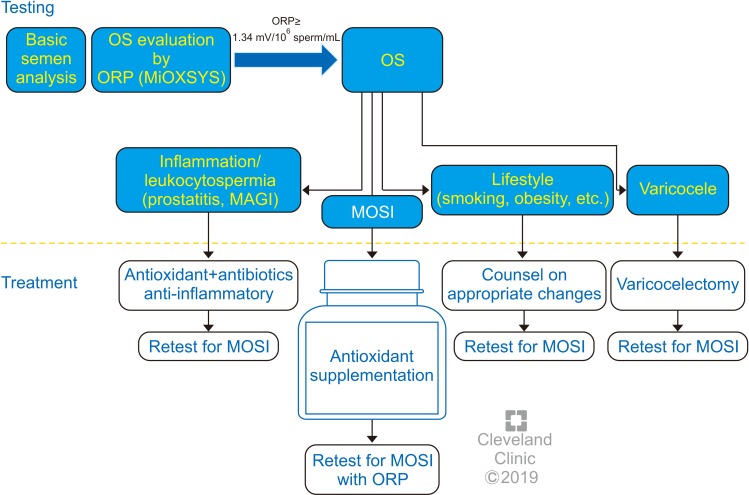
Compared with hormonal EMT and ART, antioxidants are relatively safe, inexpensive and widely available, with a growing body of data supporting their effectiveness at improving semen parameters and live birth rates [53]. Further clinical studies are indicated to directly compare live birth rates among men with MOSI assigned to receive antioxidants versus EMT and ART. Treatment guidelines providing individualized antioxidant therapy protocols based on ORP status for men with MOSI could provide a significant advancement in the management of male factor infertility and facilitate future investigations (Fig. 6) [134]. Guidelines are also necessary to avoid possible overuse of antioxidants leading to reductive stress, which can be as detrimental to sperm health as OS [52135136137] and has been associated with defects in embryogenesis [138]. Supra-physiologic levels of antioxidants may also scavenge the ROS necessary to induce sperm capacitation [3238], leading to infertility. Because antioxidants are readily available online or over-the-counter, they may appear to be a benign first-line treatment. Without clear guidelines for appropriate use, however, there is a risk of overuse in men without evidence of MOSI who may then experience delay accessing more effective therapies (e.g., ART or varicocele repair). Therefore, the oxidative status of male infertility patients should be evaluated before antioxidants are recommended and used only in those cases where MOSI is present.
Go to :
RECOMMENDATIONS AND FUTURE DIRECTIONS
Therefore, the authors recommend that men with idiopathic infertility should be screened for MOSI using an efficient, inexpensive, high sensitivity/specificity test for ORP such as MiOXSYS, which has practical advantages over alternative techniques (Table 1). Those men screening positive for MOSI should then undergo more extensive examination to identify treatable triggers and be counseled on appropriate steps to mitigate known causes of OS (e.g., smoking, alcohol consumption, lifestyle risk factors, radiation, toxins, etc.) [139140]. ORP testing should be repeated no less than 3 months following the appropriate management plan in infertile men with no explanation for MOSI. Ultimately, infertile men with MOSI should be advised to take antioxidants for a minimum of three months after other known causes of OS have been eliminated. Infertile men without MOSI should be advised against antioxidant therapy. Follow-up testing of ORP levels is recommended to confirm compliance and monitor the efficacy of antioxidant supplementation and continued lifestyle changes 6 to 8 weeks post treatment. We recommend that these approaches be tested in double blind randomized controlled trials to establish whether time to pregnancy and live birth rate is improved in couples where the man is undergoing antioxidant treatment.
With the increasing awareness and understanding of MOSI as a distinct male infertility diagnosis, the development of evidence-based guidelines that target the underlying causes, while balancing the risks and benefits of individual therapies, is imperative. The authors feel that measurement of ORP and stratification of male fertility/infertility on the basis of ORP will be an important tool in the management of infertile couples. The exact role will be defined in future trials and could validate a reclassification of male infertility that incorporates MOSI as a diagnostic category. A better understanding of the etiology of this diagnosis will help identify those men likely to benefit from antioxidant therapy while minimizing the harmful effects of antioxidant overdosing.
Go to :
 XML Download
XML Download