

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Farming as an occupation requires tremendous physical labor. Farmers sometimes must continue working in awkward postures for hours at a time, such that musculoskeletal (MSK) disorders are common.1 Across all body sites, 60% to 92% of farmers have at least one MSK disorder.2 MSK disorders of the upper extremities are common among farmers, with 1-year prevalences of 24% to 75%.34 However, these have been understudied, compared with other MSK disorders.2
In a systematic review, heavy physical, repetitive, prolonged, and monotonous work and awkward postures were identified as work-related risk factors for upper extremity MSK disorders.5 Due to the nature of farm work, fruit tree farmers are at risk of developing upper extremity MSK disorders.6 Fruit tree farmers usually work in a static position with their arms and shoulders raised. In addition, they move their hands repeatedly when they wrap and harvest fruits. Despite the high risk of upper extremity MSK disorders among fruit farmers, no studies have sought to examine the prevalence of upper extremity MSK disorders and disability among fruit tree farmers in Korea.
To address work-related upper extremity MSK diseases among farmers, the Center for Farmers' Safety and Health at Gyeongsang National University Hospital conducted the Namgaram study, which examined upper extremity MSK diseases among farmers. The objectives of the Namgaram cohort study were to (1) examine the prevalence of upper extremity MSK diseases using clinical evaluation [e.g., physical assessment, plain radiography, nerve conduction examination, and magnetic resonance imaging (MRI)] and to identify characteristics of these diseases; (2) to explore the relationship between upper extremity MSK diseases and work-related factors; (3) to establish a regional integrated management system for upper extremity MSK diseases in farmers; and (4) to provide upper extremity MSK disease prevention education to farmers. The study took place from March 2013 to December 2015. In the results of the interim Namgaram study, the prevalences of upper extremity diseases, such as rotator cuff tear, hand osteoarthritis, lateral epicondylitis, and medial epicondylitis, ranged from 21.5% to 61.9% among overhead working farmers, while non-overhead working farmers showed prevalences of 11.0% to 54.1% for the same diseases.7
Farmers with MSK diseases may continue to work with pain that affects their ability to work. According to one study, the mean number of days for which MSK pain affected their ability to work during the previous two weeks was 3.1 days for neck/shoulder pain and 2.6 days for elbow/wrist/hand pain.8 Some farmers need to modify their work habits due to MSK pain.6 Thus, MSK diseases may lead to disability in farmers.9 However, the impact of MSK diseases on disability is not well-documented. Our objectives were to (1) examine the prevalence of upper extremity MSK diseases, (2) to assess disability, (3) to examine relationships between disability and MSK diseases, and (4) to identify factors influencing disability among fruit tree farmers.
Go to : 
MATERIALS AND METHODS
Selection of subjects
This study was conducted as a part of the Namgaram study. The participants in the Namgaram study were enrolled among adults in the general population over 40 years of age in Gyeongsangnam-do, South Korea. Researchers visited the region and informed residents about the purposes of the study and the subsubjects. Then, those who agreed to participate were described the procedure of the study. Specific inclusion criteria of the Namgaram study were as follows: a person must (1) be literate and able to fill out a questionnaire; (2) have no disabilities in activities of daily living; (3) be socially active; and (4) not have been given medical service for upper extremity MSK diseases within the prior 12 months. In result, a total of 1150 residents were enrolled in the Namgaram study. Among 1150 participants of the Namgaram study, 460 participants were selected for this study according to the following criteria: (1) full-time farmers who (2) cultivated fruit trees, such as sweet persimmons, pears, apples, and grapes.
Written informed consent was obtained from all participants prior to inclusion in the study. Each participant received a questionnaire, physical examinations, laboratory tests, simple radiographic bilateral upper extremity evaluations, and bilateral shoulder MRI studies. Three research nurses trained in the purpose of this study and the data collection procedures interviewed the participants using the questionnaire. The study was approved by the Institutional Review Board of Gyeongsang National University (IRB No. GNUH 2015-02-001).
Measures
Demographics and health-related characteristics
Demographic information included sex; age; marital status, dichotomized as “yes” or “no”; educational level, categorized as “less than or equal to elementary,” “middle school,” or “high school or more than high school”; period (years) engaged in agriculture; and working hours per day (hours/day). Health-related characteristics included smoking, regular exercise, hypertension, diabetes mellitus, waist circumstance (cm), cholesterol, and depression. Depression was measured with the Patient Health Questionnaire-2 (PHQ-2): The PHQ-2 is a two-item questionnaire measured using a four-point scale [‘not at all (0)’ to ‘nearly every day (3)’].10 Higher scores indicate greater depression. Subjects were asked about their history of injuries to the upper extremities, including hands, arms, and shoulders, with responses dichotomized as “yes” or “no.”
Clinical evaluation
For diagnosis of epicondylitis, an orthopedic surgeon and a rheumatologist with more than 10 years of experience performed inquiries and physical examinations. Epicondylitis was diagnosed with self-reported pain at either of the epicondyle areas on 2 or more days in the previous month and one of the following clinical signs during the exam: Two physicians assessed any pain in the lateral humeral epicondylar region upon resisted wrist extension or tenderness on palpation of the lateral epicondyle, and any pain at the medial epicondylar region upon resisted wrist flexion or tenderness on palpation of the medial epicondyle.11 A positive case was defined as positive symptoms at the elbow or forearm based on the structured interview, plus a corresponding positive physical examination on the symptomatic side. Only dominant side cases were considered in these analyses.
For diagnosis of hand osteoarthritis, anterior-posterior plain radiographs of both hands were obtained from all participants. The second to fifth distal interphalangeal, proximal interphalangeal, first to fifth metacarpophalangeal, thumb interphalangeal, and first carpometacarpal joints for each hand were graded for osteoarthritis using the modified Kellgren-Lawrence scale to assess the existence and severity of osteophytes, joint space narrowing, sclerosis, and erosion. The modified Kellgren-Lawrence scale was graded from 0 to 4, where 0 is no osteoarthritis; 1 is questionable osteophytes and/or joint space narrowing; 2 is definite small osteophytes and/or mild joint space narrowing; 3 is moderate osteophytes and/or moderate joint space narrowing, sclerosis, and possible presence of erosion; and 4 is large osteophytes and/or severe joint space narrowing, sclerosis, and possible presence of erosion.12 Radiological hand osteoarthritis was defined as a case wherein the results of plain radiography were determined to be higher than Kellgren-Lawrence grade 2 for at least one joint.13 The interpretation of these radiographs was performed by a radiologist with 20 years of experience in MSK radiographic evaluation and a rheumatologist with 10 years of experience in radiographic evaluation. Both readers were blinded to the patients’ health history.
For diagnosis of rotator cuff tears, including partial and full thickness tears, a 3.0 Tesla MRI system (Ingenia; Philips Medical Systems, Eindhoven, the Netherlands) was used to obtain MRI images. The MRI images included axial, sagittal, and coronal T2-weighted images (TR/TE=2800/60), coronal T1-weighted images (TR/TE=500/20), and coronal fat-saturated fat spin-echo images. The field of view was 16 cm; the data matrix size was 448×448; and the slice thickness was 3 mm without gaps. MRI images were interpreted by a radiologist with 20 years of experience and an orthopedic surgeon with 15 years of experience. Both physicians performed blinded evaluation without any information about subjects’ health history.
Outcomes: disability
Disability was assessed using the Disabilities of the Arm, Shoulder, and Hand questionnaire (DASH), which was designed to address the impact on function for a variety of MSK diseases and injuries in the upper extremities.14 We used the Korean version of the DASH (K-DASH) with validity and reliability.15 It is a 30-item questionnaire (21 physical function items, six symptom items, and three social/role function items). Each item is rated on a five-point Likert scale (1=least disability to 5=most disability). All 30 response scores are added together, producing a raw score, which is then transformed into a score with a maximum of 100. Higher scores indicate greater disability. The Cronbach's alphas of the K-DASH were 0.94–0.96, while the alpha was 0.95 in this study.
Data analysis
SPSS, version 24.0 for Windows (IBM, Armonk, NY, USA) was used to analyze the data. Descriptive statistics were used to analyze means and frequency of variables. Univariate regression analyses were used to identify the potential explanatory factors of disability. Statistically significant variables in the univariate analysis were included in a stepwise multivariate linear regression model with disability. Multi-collinearity was tested with variance inflation factor (VIF; acceptable level=less than 10) and tolerance (acceptable level=more than 0.1).
Go to :
RESULTS
Demographics and health-related characteristics
Demographics and health-related characteristics of the fruit tree farmers are shown in Table 1. Participants comprised a mean age of 59.67 years (range 40 to 79 years), an average of 31.36 years of agriculture engagement period (range 2 to 65 years), and an average of 7.35 hours per a day (range 2 to 15 hours/day) of working hours.
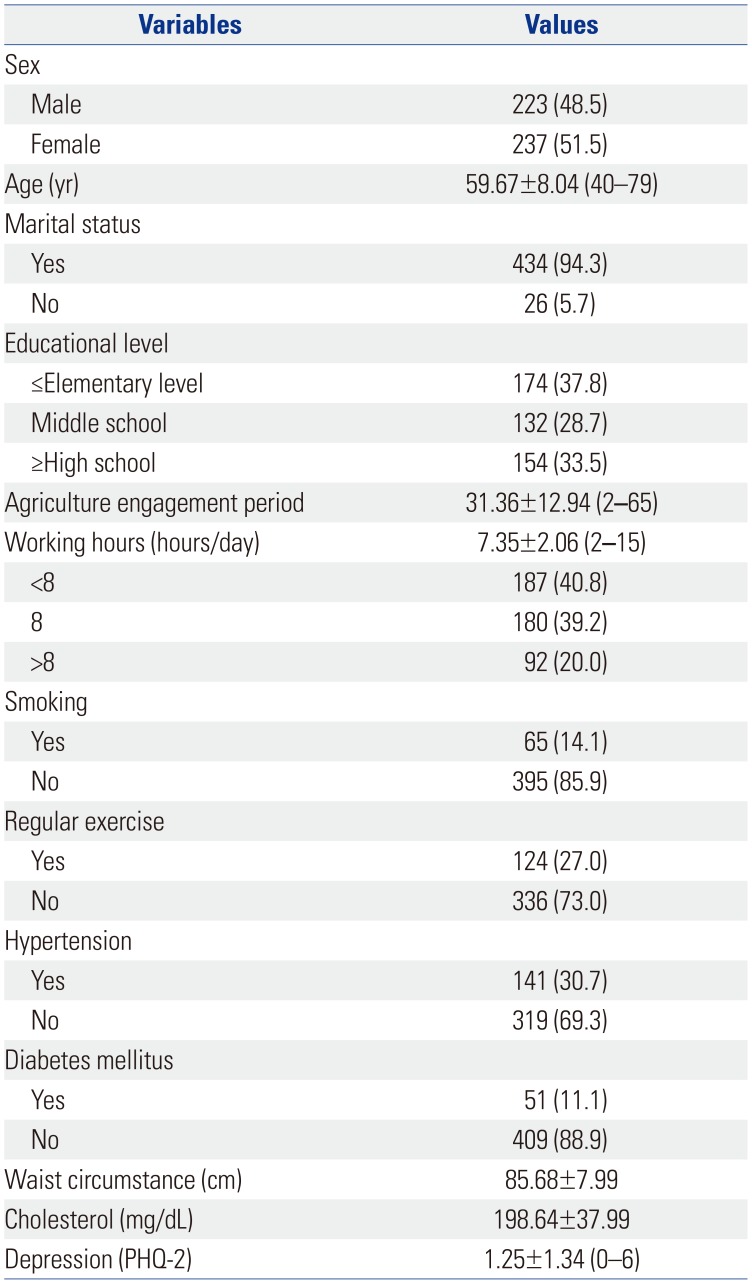
Table 1
Demographics and Health-Related Characteristics of the Study Population (n=460)
![]()
The majority of participants were non-smokers (85.9%) and did not engage in regular exercise (73.0%). Around 31% of participants had hypertension, while the prevalence of diabetes mellitus was only 11.1%. Subjects had an average waist circumference of 85.68 cm and an average cholesterol level of 198.64 mg/dL. The mean of the PHQ-2 score was 1.25 (range 0 to 6).
Disability and results of clinical assessment regarding MSK disease
Disability and the results of the clinical assessment regarding MSK diseases are shown in Table 2. The mean DASH score in fruit farmers was 14.58 (range 0 to 81.67). Some farmers had experiences of injuries to the hands (8.7%), arms (5.7%), and shoulders (11.5%). About 89.6% of participants had at least one MSK disease. More specifically, the prevalences of various upper extremity MSK diseases were as follows: 60.4% for rotator cuff tear, 20.9% for golf elbow, 40.9% for tennis elbow, and 58.0% for hand osteoarthritis.
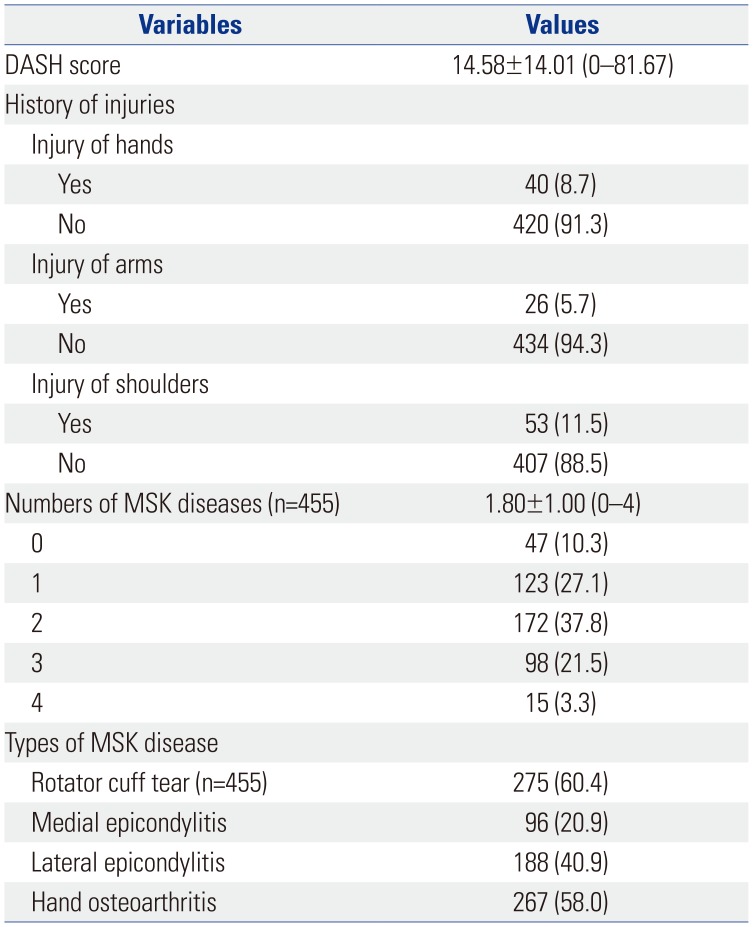
Table 2
Disability and Results of Clinical Assessment Regarding Musculoskeletal Diseases (n=460)
![]()
Results of simple regression analyses
To explore the relationships between DASH scores and each variable, univariate regression analyses were performed (Table 3). As a result, sex (B=−7.22), smoking (B=−6.95), waist circumstance (B=−0.17), depression (B=3.49), working hours (B=1.15), injuries of the arms (B=14.16) and shoulders (B=7.99), and number of upper extremity MSK diseases (B=2.43) were associated with disability.
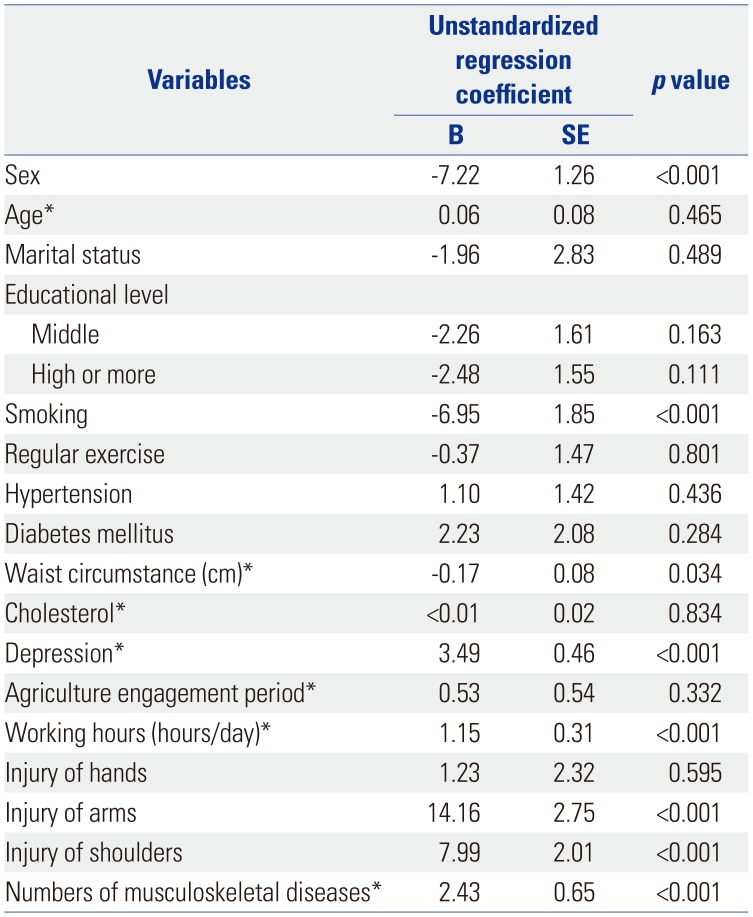
Table 3
Univariate Regression Analysis to Explore Potential Factors Affecting Disability in Fruit Farmers (n=460)
![]()
Factors influencing disability among fruit farmers
We conducted multivariate regression analyses with variables identified as having significant relationships with disability in univariate regression analyses (Table 4). Tests for multi-collinearity indicated that a very low level of multi-collinearity was present (VIF 1.02–1.24; tolerance 0.80–0.98). Disability in fruit farmers was associated with female sex (B=−4.47, p<0.001), smoking (B=−4.00, p=0.026), depression (B=2.83, p<0.001), working hours (B=0.96, p=0.001), injuries of the arms (B=10.78, p<0.001) and shoulders (B=6.75, p<0.001), and numbers of upper extremity MSK diseases (B=2.02, p=0.001), with 26.5% of the variance explained (R2=0.265, Durbin-Watson test=1.81, p<0.001).
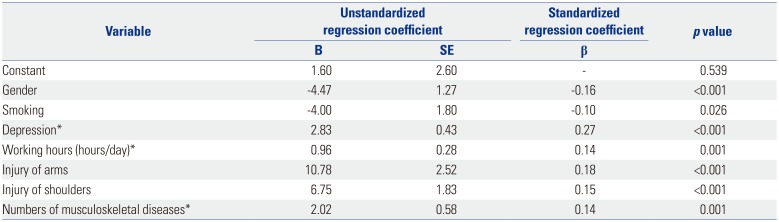
Table 4
Multivariate Regression Analysis to Explore the Factors of Disability in Fruit Farmers (n=460)
![]()
Go to :
DISCUSSION
This study aimed to examine the prevalence of upper extremity MSK diseases and to identify factors influencing disability in fruit tree farmers who participated in the Namgaram project. The result from this study indicate that the majority of fruit tree farmers (89.7%) have suffered from at least one upper extremity MSK disease, which is consistent with that of another Korean study reporting a 91.0% prevalence of upper extremity MSK symptoms among fruit tree farmers.16 The common upper extremity MSK diseases in fruit tree farmers were rotator cuff tear (60.4%) and hand osteoarthritis (58.0%) in our study. Although the physical burden of modern farming has decreased due to the mechanization of agriculture, fruit tree farmers still perform packing and sorting operations in an uncomfortable working posture and must perform repeated heavy lifting. As a result, MSK symptoms in fruit tree farmers are more likely to occur in the upper body.16
The mean score of disability in fruit tree farmers was 14.58±14.01 in this study, while it was 10.03±10.85 in the non-farmer group in the Namgaram study7 and 12.5±10.8 in dairy farmers.4 In addition, poorer disability was associated with a larger number of upper MSK diseases and a history of injuries of the arms and shoulders in this study, which is consistent with a previous study.79 Despite poor disability and a high prevalence of upper extremity MSK diseases in our study, many fruit free farmers (59.2%) worked eight hours or more per day; some farmers worked for up to 15 hours per day. This is consistent with previous studies reporting long working hours of farmers.36 This is because there is no the closing time for the farmers. As mentioned before, farmers with MSK diseases work with pain that affects their ability to work.8 Returning to work with MSK diseases may aggravate and further exacerbate MSK diseases of farmers. To improve disability among fruit tree farmers, it is necessary to develop a strategy for prevention and treatment of upper MSK diseases that is easy to implement and provides well-designed healthcare for farmers.
Workload is known to be a risk factor for MSK disorders.35 Working hours per day was a significant factor for disability in fruit tree farmers in our study. Herein, fruit farmers were an average of 59.67 years old and had an average of 31.36 years of farming experience. According to a Korean study exploring working hours of farmer couples, working hours of farmers during farming season are extremely high, sometimes twice the average working hours of workers nationwide.17 As the industry has developed, the mechanization of agriculture has allowed many farmers to use farming machinery. However, fruit tree farmers still need to use their bodies intensely for many agricultural tasks and work in awkward postures for long periods of time.
In terms of sex differences, female farmers were more likely to have poorer disability, compared to males, in this study. Similarly, in previous studies, women complained of more frequent and severe MSK pain than men.31819 Farmers who conduct harvesting and paving work are typically older adults or female farmers in Korea.20 In a previous study, male fruit tree farmers worked an average of 10.2 hours per day during the farming season and 5.2 hours per day during the non-farming season, while female fruit tree farmers worked an average of 10.6 hours per day during the farming season and 5.5 hours per day during the non-farming season.16 In addition, despite the physical vulnerability of women, female farmers living in rural areas tend to uphold traditional gender roles adding on the burden of housework.1718 As a result, female farmers are exposed to the risk of developing more severe MSK diseases and lower function because there is not enough time to rest and take care of their own health before returning to work.
This study has several limitations. The retrospective collection of work-related characteristics and self-reported health outcomes can produce recall bias since farmers may not remember or may recall inaccurately. In addition, the sample of farmers who were asked to participate in the current study represent a homogenous group of farmers cultivating fruit trees. Therefore, the results may not be generalizable to farmers cultivating other crops. However, this study is significant for examining the prevalence of not only MSK pain, but also MSK diseases, by using clinical evaluations. In addition, few previous studies have been conducted on upper extremity MSK diseases and disability in fruit tree farmers who predominantly use their upper extremities in their work. Further research is necessary to examine specific MSK diseases and disability among farmers according to the types of crops they grow.
Most fruit tree farmers have experienced upper extremity MSK diseases, which are associated with poorer disability. Furthermore, a history of injuries of the arms and shoulders and long work hours were associated with disability. These results suggest that fruit tree farmers should be educated about workrelated MSK diseases and prevention strategies. There is a need for fruit tree farmers to reduce working time and schedule regular health checkups. Therefore, at the government level, it is necessary to develop effective management strategies for agricultural work-related MSK diseases and surveillance systems for health problems, with efforts to improve the work environment in agriculture.
Go to :
 XML Download
XML Download