

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Inflammatory bowel diseases (IBDs), such as Crohn's disease (CD) and ulcerative colitis (UC), are chronic inflammatory diseases that involve the gastrointestinal tract.1 Although the pathogenesis and etiology of IBD are not well understood, it has been hypothesized that its pathogenesis involves environmental and genetic factors.2 Impaired immunity in response to the intestinal flora and antigens are thought to cause chronic inflammation in the alimentary tracts.23
Malnutrition is found in up to 85% of patients with IBD, in the active and remission phases. Micronutrient deficiencies are present in more than half of patients with IBD. The deficiencies are more frequent in CD than in UC and in active disease than in remission.4 The most common micronutrients deficiencies in IBD are vitamin B12, folate, iron, and especially vitamin D.
Vitamin D is known as the most important regulator of calcium (Ca) and phosphorus (P) metabolism related to bone health but studies suggest the new role of vitamin D in immunomodulation recently,5 and Vitamin D is even proposed as a treatment for autoimmune diseases such as multiple sclerosis,6 systemic lupus erythematous,7 and IBD.8 Furthermore Ananthakrishnan et al.9 has reported that vitamin D deficiency may play a role in the increased risk of malignancies in IBD. However, limited studies have been conducted about the relationship between vitamin D and disease activity in IBD over a multi-year period, especially in pediatric patients so far.
Therefore, we aimed to investigate the association of vitamin D with disease activity and clinical course in pediatric patients with IBD.
METHODS
Patients
Our study was performed in the Pediatric Gastroenterology, Hepatology and Nutrition Clinic of Severance Children's Hospital for patients diagnosed with UC or CD from September 2012 to April 2018.
Patients younger than 19 years of age who were diagnosed with CD or UC according to the Revised Porto Criteria and underwent regular follow-up were included in this study. Patients diagnosed with IBD unclassified, patients who did not undergo blood tests including vitamin D during the active and remission phases, patients with insufficient medical records, and patients with vitamin D supplementation were excluded.
Data collection
The medical records of the enrolled patients were retrospectively analyzed. Clinical records and laboratory test results during the active and remission phases were collected for each patient. We recorded the highest disease activity score and longest duration of remission in cases when there were multiple active phases or remission phases in one patient. In this study, the active phase was defined as when the disease activity score (Pediatric Crohn's Disease Activity Index [PCDAI] or Pediatric Ulcerative Colitis Activity Index [PUCAI]) was 10 or more. The remission phase was defined as the period when the patient's clinical symptoms were relieved and the disease active score remained below 10 points for more than 3 months without the use of steroids.
Biochemical assessment
Our registry includes demographic, laboratory, clinical, endoscopic, radiological, and pathological data of the enrolled patients, and it is updated routinely. Clinical records and disease activity scores documented at 2 to 6-month intervals were collected for each patient. Serologic markers of inflammation, including the C-reactive protein (CRP) level, erythrocyte sedimentation rate (ESR), and white blood cell (WBC), as well as levels of serum Ca/P, folate, vitamin B12, zinc, albumin, pre-albumin, and vitamin D were collected. To evaluate patients' vitamin D status, the serum level of 25-hydroxyvitamin D 25[OH]D was measured using the liquid chromatography-tandem mass spectrometry in the clinical laboratory.
Statistical analysis
Laboratory data for CD and UC, and laboratory data for active and remission phases were analyzed using the Mann-Whitney U test. The changes of active and remission phases in each patient were analyzed using the paired t-test. We compared the vitamin D levels of an age-matched healthy control group from the Korea National Health and Nutrition Examination Survey and those of our study patients with IBD by using the Student's t-test. Vitamin D levels in the active and remission phases were compared using the Kruskal-Wallis test for each season (spring, summer, fall, and winter).
All statistical analyses were performed using the SPSS software (version 23.0; IBM Corp., Armonk, NY, USA). The 95% confidence interval is reported where relevant. Two-sided P values of < 0.05 were considered statistically significant.
Ethics statement
The protocol of this study was approved by the Institutional Review Board (IRB) of Severance Hospital (IRB approval No. 4-2018-1044). Because this was an observational study without intervention and without the presentation of any identifying data, the committee ruled that informed consent was unnecessary.
RESULTS
Ninety-six patients with IBD (72 patients with CD, 24 patients with UC) formed the study population. Table 1 shows the study population's basic demographics, clinical characteristics, and data on vitamins. There was a significant difference in gender between the patients with CD and those with UC. A higher percentage of man patients had CD, whereas a higher proportion of woman patients had UC.
Table 1
Demographic data and characteristics of patient

Values are presented as No. (%) or median (interquartile range). Disease activity score was based on Pediatric Crohn's Disease Activity Index and Pediatric Ulcerative Colitis Activity Index scores.
CD = Crohn's disease, UC = ulcerative colitis, NA = not applicable.
![]()
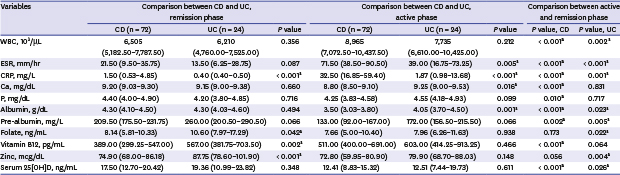
As shown in Table 2, there was no significant difference between CD and UC for serum 25[OH]D. The inflammatory markers were elevated in patients with UC and CD during the active phase compared to those during the remission phase. Additionally, the inflammatory markers were higher in patients with CD than in those with UC during both phases.
Table 2
Laboratory findings in inflammatory bowel disease patients in active phase and remission phase

Values are presented as median (interquartile range).
CD = Crohn's disease, UC = ulcerative colitis, WBC = white blood cell, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, Ca = calcium, P = phosphorus.
aP value < 0.05, statistically significant.
![]()
Ca, P, and albumin levels remained relatively unaffected by disease activity in patients with UC. These micronutrients were lower in the active phase and showed a tendency to recover well during the remission phase in patients with CD.
In patients with UC and CD, folate and zinc levels showed a tendency to be dependent on disease activity, as they decreased in the active phase and increased in the remission phase. These micronutrients tended to recover well during the remission phase in patients with UC, but less recovery was shown in patients with CD. Specifically, vitamin B12 was higher in the active phase than in the remission phase.
Vitamin D in patients with UC and CD showed a significant difference according to disease activity. In particular, the vitamin D level was higher in the remission phase than in the active phase, but it remained in “insufficiency” status.
Except for vitamin B12, the other micronutrients showed a tendency to increase significantly in the remission phase than in the active phase according to the paired t-test. Vitamin D showed a larger difference in remission and active phases than other micronutrients when evaluated using fold-change measurements (Fig. 1).
 | Fig. 1Comparison of vitamin D and micronutrients (combined standard). Vitamin D showed a larger difference in remission and active phases than other micronutrients when evaluated using fold-change measurements.
|
IBD patients in the active phase showed a lower mean vitamin D level than the healthy control group and remission phase group. Vitamin D levels of the remission phase group and control group based on youth in the Korea National Health and Nutrition Examination Survey of 2015 were similar (Fig. 2).
 | Fig. 2Comparison of vitamin D difference in active, remission and control group. Inflammatory bowel disease patients in the active phase showed a lower mean vitamin D level than the healthy control group and remission phase group. Vitamin D levels of the remission phase group and control group based on youth in the Korea National Health and Nutrition Examination Survey of 2015 were similar.
|
However, there was no statistically significant difference in the vitamin D level during the active phase whether or not IBD involved the ileum (12.45 ng/mL and 11.91 ng/mL, respectively).
Finally, measured vitamin D levels in active phase and remission phase were sub-grouped according to the measured season. There were seasonal variations in the active phase, but there was no significant difference by season in the remission phase (Fig. 3).

DISCUSSION
Many studies have been conducted on malnutrition and micronutrient deficiencies due to the reduction of oral intake and increased gastrointestinal losses of nutrients in patients with IBD.13 Several studies have reported micronutrient deficiency in IBD and analyzed the relationship between nutritional deficiency and body mass index or body fat in IBD patients.1415
Especially many studies have conducted regarding vitamin D in IBD and some reports suggested that vitamin D regulates the secretion and inhibition of cytokines involved in the inflammatory response in immune systems as well as Ca homeostasis.161718 Therefore, it is important to supplement vitamin D and micronutrients in the treatment of IBD.1920 However, these malnutrition and micronutrient deficiencies have not been studied in pediatric patients with IBD, even though these patients should be treated immediately to prevent adverse effects on their growth and development.
Our study showed that inflammatory markers, e.g., WBC, ESR, and CRP, are more elevated in CD than in UC, and this tendency was observed in the active and remission phases.
Ca, P, and albumin were not significantly affected by disease activity in UC, whereas they remained significantly lower in the active phase than in the remission phase of CD and recovered well at the time of remission. In patients with UC and CD, folate and zinc levels showed a correlation with disease activity. They decreased in the active phase and increased in the remission phase. It is thought that IBD, especially CD, involving the small intestine, which is the site of folate and zinc absorption, affects the terminal ileum and increases folate and zinc deficiencies.212223
Interestingly, our study showed that vitamin B12 was higher in the active phase than in the remission phase. This finding is different from results of other studies in which micronutrients were found to be lower in the active phase and in CD.24 However for the accurate assessment of vitamin B12 deficiency, functional studies of homocysteine (low level) or methylmalonic acid (high level) are necessary.25 Although additional functional studies should have been performed in our study, we think that vitamin B12 is less affected by inflammatory activity than other micronutrients.
Our results confirmed the findings of previous studies that reported a high prevalence of vitamin D deficiency in IBD.2627 Although the mechanism is still unclear, vitamin D deficiency may be associated with an increased IBD activity score, lower sun exposure, and decreased absorption from inflammatory mucosa.182829 In our study, the vitamin D level was higher in the remission phase than in the active phase in UC and CD. The reason for the increased vitamin D level in the remission is unclear, but is probably a result of a combination of increased nutritional intake, increased outdoor activity and reduced need for steroid therapy.2830 Because previous studies have suggested that steroids may enhance inactivation of 25[OH]D by promoting 24-hydroxylase activity.31 Also, as the disease improves, increased level of vitamin D will help the inducing or maintaining of remission by improving anti-inflammatory and immune-mediated regulation. Indeed, our study show that vitamin D level was similar in those who did and did not have ileocecal valve resection. Bile acid, which is known to be involved in lipid-soluble vitamin absorption, is reabsorbed through ileum. These results indicate that vitamin D deficiency in IBD is mostly related with disease activity rather than decreased absorption due to inflammation of the small intestine. Therefore, in order to prevent various complications of vitamin D deficiency, it is important to maintain a prolonged remission state by controlling the activity of IBD.
Compared to other micronutrients, vitamin D levels tended to show a larger difference depending on disease activity. This result suggests that vitamin D deficiency itself in IBD may lead to disease aggravation. Recent studies have shown that vitamin D is involved in the immune system and inflammatory response by inhibiting the regulation of inflammatory cytokines and differentiation of proinflammatory cells.3233 Further, other studies demonstrated an experimental link between vitamin D status and severity of IBD in animals: vitamin D deficiency exacerbated the symptoms and severity of enterocolitis in interleukin-10 knockout mice, whereas supplementation with vitamin D ameliorated IBD symptoms, reduced inflammation, and improved histologic scores and mortality.34
According to Garg et al.,35 fecal leukocytes (e.g., calprotectin) more closely reflect intestinal inflammation than systemic markers (e.g., CRP, ESR, and WBC). They also reported an inverse correlation between the levels of vitamin D and calprotectin in patients with IBD. These findings support the theory that serum 25[OH]D may affect local tissue inflammation. Thus, vitamin D supplementation may need to be studied as a drug for regulating IBD inflammation and providing nutritional support.
In our study, patients in the active phase showed seasonal variation, with decreasing vitamin D levels in spring and winter. However, there was no significant difference by season in the remission phase, suggesting that patients in the active phase are more sensitive to seasonal factors.
There are limitations to our investigation. First, this study had a retrospective design and was performed in a single center with a small sample of patients. Second, the effects of sun exposure, dietary or over the counter vitamin D supplementation could not be measured accurately. In Korea, there is little exposure to sunlight between 33°N and 43°N, and there is not enough difference in available sunlight by season. Third, many patients lacked sufficient available endoscopic findings in order for us to investigate the association between vitamin D status and the degree of inflammation. Lastly, this study lacked bone mass densitometry study results and fecal calprotectin levels for most patients.
In conclusion, malnutrition and micronutrient deficiencies are common in IBD. Especially, vitamin D deficiency showed the greatest difference according to IBD activity, and it may be related to intestinal absorption as well as medication and sun exposure. IBD itself may affect vitamin D deficiency, and a low vitamin D level may aggravate the inflammatory response of IBD. Lack of micronutrients, including vitamin D, can lead to worsening of IBD and cause irreversible sequelae in growing children; therefore, it is important to prevent and correct vitamin D deficiency as soon as possible. In the future, it will be important to monitor the vitamin D level more carefully in the active phase, spring, and winter in Korean pediatric patients with IBD and to provide sufficient vitamin D supplementation if there is a deficiency.
 XML Download
XML Download