

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Microfracture is generally known as the first-line surgical treatment for focal cartilage defects owing to its many advantages such as technical simplicity and cost-effectiveness. The technique itself and first treatment results were published in 1994 by Rodrigo,1) and Steadman et al.2) introduced an advanced technique to enhance chondral resurfacing in 2002. Since then, the microfracture procedure has been widely used and considered as the routine strategy for treatment of chondral lesions for the past 15 years. Despite the long history and popularity of this procedure, the quality of cartilage repair after microfracture is variable and remains unclear. The healed cartilage at the chondral defect site after microfracture is known as fibrocartilage or hyaline-like cartilage, and the appearance of healed lesions is inconsistent.3)
Furthermore, limited information is available about the clinical outcomes after microfracture for chondral lesions in middle-aged patients. Many studies have been conducted to evaluate the outcomes in adolescent or young patients treated with microfracture for traumatic chondral lesions.2456789) Although some studies including patients aged more than 40 years have been reported, there has been no study focusing on middle-aged patients between 40 and 60 years.1011121314) According to a recently published study on the incidence of arthroscopy-documented cartilage injuries of the knee in 21,392 patients, an outstanding increase and the most frequent use of knee arthroscopy for cartilage injury during 3 years (2008–2011) was observed in the age group of 40–60 years.15) Curl et al.16) conducted a study on cartilage injury with a review of 31,516 knee arthroscopies and reported that grade IV lesions based on a modified Outerbridge scale were found three times more frequently in patients over 40 years of age. Progression of cartilage defects could result in joint inflammation and further degeneration and disability leading to osteoarthritis (OA).17) Owing to increased incidence and advanced degree of knee chondral lesions in middle-aged patients, the number of non-advanced symptomatic knee OA patients in the United States in 2016 was highest in the age group of 40–60 years.18) However, the rarity of research on knee cartilage injury of middle-aged patients between 40 and 60 years limits prediction of treatment outcome.
In addition, reports on the outcome of microfracture in middle-aged Asian patients are rare. They are commonly exposed to the high-flexion activities such as kneeling, squatting, and cross-legged sitting in daily life for cultural reasons. During high flexion, excessive compressive pressure is generated at all compartments of the knee joint, leading to accelerated degeneration of cartilage.19) However, prediction of treatment outcome is limited due to the lack of research on knee cartilage injury of middle-aged Asian patients between 40 and 60 years. Therefore, the purpose of this study was to investigate the changes in clinical and radiological outcomes of arthroscopic microfracture of knee chondral lesions in middle-aged Asian patients over time.
METHODS
This study was conducted in compliance with the principles of the Declaration of Helsinki. The arthroscopic surgery database of one tertiary referral center was reviewed retrospectively after obtaining approval from the Institutional Review Board (IRB No. 1611-022-531) with written informed consents. Patients were included in this study if they had localized cartilage defects of the knee confirmed by arthroscopy, had a minimum 1-year follow-up after microfracture, and were between the ages of 40 and 60 years at the time of surgery between January 2000 and September 2015. Microfracture surgery was performed according to the indication of 1 or 2 symptomatic focal full-thickness articular chondral defects (International Cartilage Repair Society [ICRS] grade 3–4) on the femoral condyles or trochlea, with a total size between 1 and 5 cm2. All arthroscopic procedures were determined and performed by a senior surgeon (MCL). To identify the cases with early OA, patients with progressive degenerative changes on X-ray (higher than Kellgren-Lawrence [KL] grade 3 and coronal deformity greater than 5 degrees from the mechanical axis [MA]) were excluded (Fig. 1). Concomitant surgeries with microfracture were reviewed, and to reduce data heterogeneity, only meniscectomy was included. Therefore, patients who underwent microfracture with other procedures including ligament surgery, realignment procedure, and foreign body removal were excluded. Patients who had not been followed up serially or missed a follow-up visit were contacted by telephone to ask for an outpatient department visit or for data collection. If there was no response after a minimum of three attempts at contact, the patient was considered lost to follow-up. In total, 71 patients were available for the clinical follow-up.

Patients' demographic information such as age, sex, laterality, weight, height, body mass index (BMI), and follow-up duration were obtained from the arthroscopic surgery database. The surgical record showed information on the size and location of cartilage defects and combined surgery. The recovery status of the osteochondral lesions was compared using the magnetic resonance observation of cartilage repair tissue (MOCART) score in 32 patients who underwent magnetic resonance imaging (MRI).20) For determination of the correlation of clinical outcome with MRI findings, the following nine variables of MOCART score were tested for correlation with the clinical score: degree of defect repair and filling of the defect, integration of border zone, surface of the repair tissue, structure of the repair tissue, signal intensity of the repair tissue, subchondral lamina, subchondral bone, adhesions, and synovitis. For clinical evaluation, preoperative and 1-, 2-, 5-, 7- and 10-year follow-up scores were compared by using the International Knee Documentation Committee (IKDC) score, modified Lysholm score, Knee Injury and Osteoarthritis Outcome Score (KOOS), Tegner activity scale, and visual analog scale (VAS, 1–10) score for pain and patient satisfaction.2122) The serial change in MA, KL grade, and joint line obliquity on simple radiographs were evaluated. To evaluate the failure rate of microfracture, the incidence of conversion to additional procedures such as total knee arthroplasty (TKA), unilateral knee arthroplasty (UKA), or high tibial osteotomy (HTO) was calculated.
Surgical Technique
Microfracture was performed arthroscopically in all patients. After assessment of the full-thickness articular cartilage lesion, the exposed subchondral bone was debrided of unstable cartilage. During debridement of the cartilage, marginally attached cartilage from the surrounding rim of the articular cartilage or loose bodies was also removed thoroughly to form a stable perpendicular edge of healthy vital cartilage around the defect.23) Then, an arthroscopic awl was used to make multiple perforations into the exposed subchondral bone plate while taking care to not make excessive damage to the subchondral bone.2) The holes were placed 3–4 mm apart without breaking the subchondral bone plate between them. Fat droplets from the marrow cavity were identified to confirm appropriate depth (2–4 mm). When the blood flow from the bone marrow appeared to be adequate in all areas of the defect after reduction of the fluid pressure and deflation of the tourniquet, the procedure was terminated. Intra-articular drains were not inserted.
Rehabilitation Protocol
To promote recreation and development of the newly recruited mesenchymal stem cells from the bone marrow, continuous passive motion (CPM) was applied for all patients regardless of the size and location of the lesion. After surgery, patients were advised to perform CPM in the recovery room with increasing range of motion, with the usual speed of one cycle per minute for 6–8 hours per day.2)
For patients with medial and lateral tibiofemoral chondral lesions, only crutch-assisted toe-touch weight bearing was allowed for 2 weeks, and tolerable weight bearing was allowed according to lesion size. For patients with patellotrochlear chondral lesions, tolerable weight bearing was allowed with full knee extension. Closed kinetic chain exercises were started at 2–3 weeks after surgery, and open kinetic chain exercises were started at 7–8 weeks postoperatively. More complex sports-specific activity was initiated at 2–3 months postoperatively and return to sports activity was recommended at 4–6 months postoperatively.
Statistical Analysis
Patient demographic data were summarized and analyzed. Correlations between variables of MOCART score and clinical scores were analyzed with the Spearman correlation coefficient and the Student t-test. For ordinal variables with more than three categories such as the degree of defect repair and filling of the defect, integration of border zone, surface of the repair tissue, and signal intensity of the repair tissue, the Spearman correlation coefficient was used; for variables with two categories such as structure of the repair tissue, subchondral lamina, subchondral bone, adhesions, and synovitis, the Student t-test was used. For preoperative and postoperative 1-, 2-, 5-, 7-, and 10-year follow-up functional scores, pairwise comparisons with paired t-test were performed and followed by Bonferroni correction for multiple comparisons. Serial comparison of X-ray measurement was assessed by pairwise comparison of Friedman rank sums. Survivorship analysis with conversion to additional surgery as an end point was performed by using Kaplan-Meier survival curves. All results were analyzed with IBM SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA). A p-value < 0.05 was considered statistically significant.
Go to : 
RESULTS
The mean age of the patients at the time of microfracture was 51.3 ± 4.7 years (range, 40 to 60 years). Of 71 patients, 44 were female and 27 were male. The mean BMI was 26.5 ± 3.3 kg/m2 (range, 18.9 to 30.5 kg/m2). Thirty-seven (53%) and 34 (47%) patients underwent microfracture on the right side and left side, respectively; there was no bilateral case. The mean follow-up duration was 7.2 ± 2.6 years (range, 1.0 to 17.4 years). The number of patients who had a follow-up period of more than 1, 2, 5, 7, and 10 years was 71, 65, 39, 26, and 12, respectively (Table 1). The mean cartilage defect size was 3.4 ± 1.9 cm2 (range, 1.1 to 5.2 cm2). Concomitant meniscectomy was performed in 33 patients (47%), and microfracture alone was performed in 38 patients (53%). There were 43 lesions (60%) on the medial femoral condyle, 15 lesions (21%) on the lateral femoral condyle, nine lesions (13%) on the trochlear condyle, and four lesions (6%) on multiple locations (Table 2).
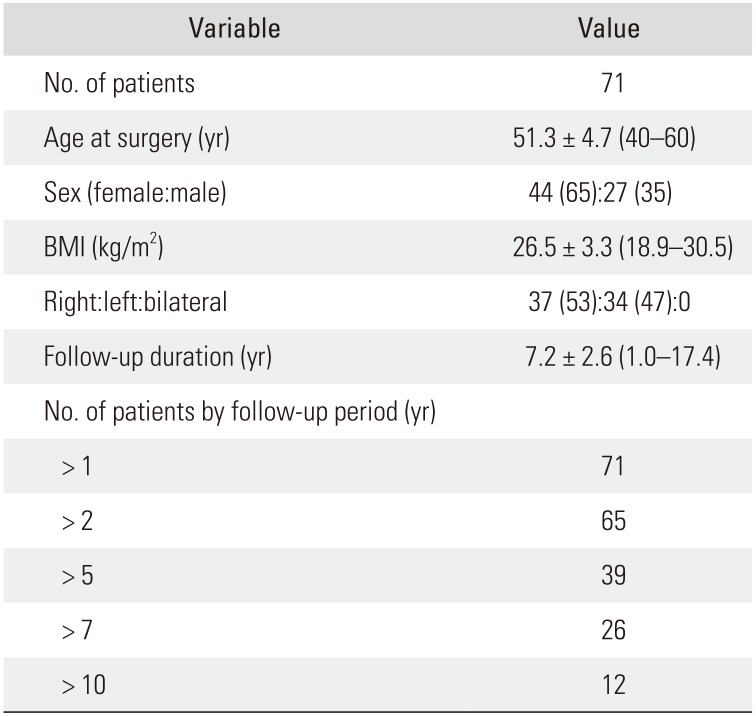
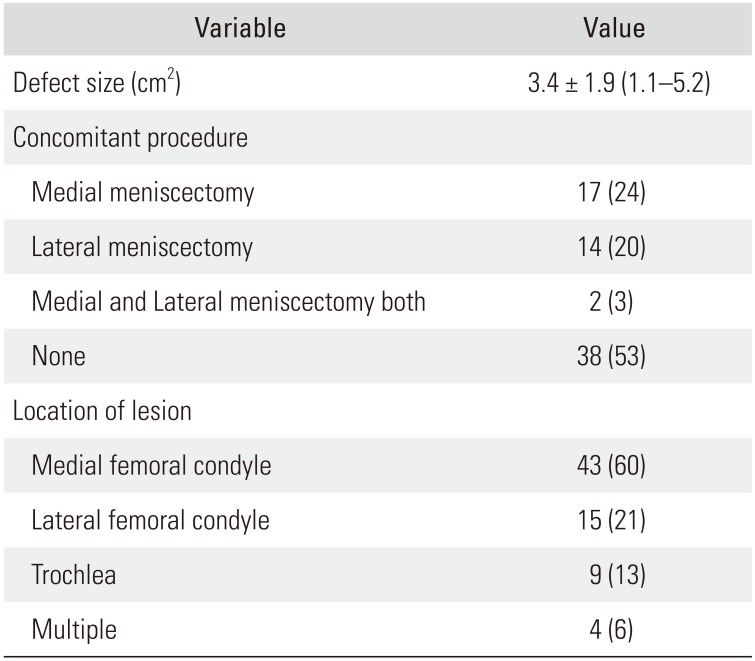
Table 1
Summary of Demographic Characteristics
![]()
Table 2
Summary of Surgical Characteristics
![]()
MRI Evaluation
MRI was done in 32 patients at a mean follow-up of 2.1 ± 0.3 years (range, 1.8 to 2.5 years). The MOCART score revealed three cases (9%) of full recovery, two cases (7%) of hyperplastic recovery, 23 cases (70%) with more than 50% filling, and four cases (14%) with less than 50% filling. The degree of the integration at the border was incomplete in most cases. The surface of recovered tissue was intact in 23%, and the rest was incomplete; 38% of the recovered tissue was homogenous and showed intact subchondral lamina. The clinical scores did not correlate with the MRI findings (Table 3).
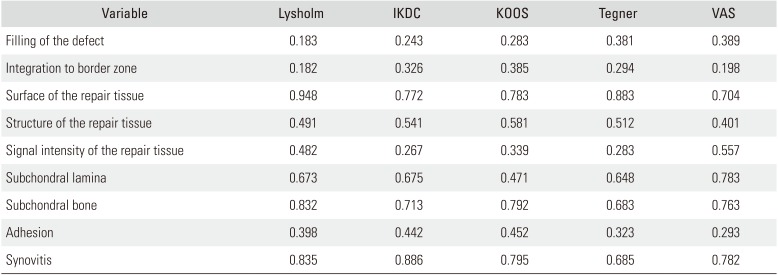
Table 3
The p-value of Spearman Correlation Coefficient and t-test in Comparison of Clinical Outcome and Variables of MOCART Score
![]()
Clinical Outcomes
Clinical trend analysis of patients undergoing microfracture showed a significant improvement in all clinical results (Lysholm, IKDC, KOOS, Tegner, and VAS scores) at 1 year after surgery (p < 0.05). However, all clinical outcomes deteriorated with time at 2, 5, 7, and 10 years. In particular, the IKDC, Lysholm, and VAS score showed statistically significant deterioration (p < 0.05) from 1 year to 10 years after surgery. At the final follow-up of more than 10 years, there was no clinically significant improvement and the scores were almost the same as the preoperative ones (Fig. 2). Regarding patient satisfaction, 59% of the patients showed overall satisfaction at the final follow-up.
 | Fig. 2Changes in clinical scores. All clinical results at 1 year after surgery showed significant improvement (*) and tended to deteriorate with time at 2, 5, 7, and 10 years. In particular, Lysholm, International Knee Documentation Committee (IKDC), and visual analog scale (VAS) scores showed statistically significant deterioration from 1 to 10 years after surgery (#). KOOS: Knee Injury and Osteoarthritis Outcome Score.
|
Radiological Evaluation
According to the evaluation of the KL grade, there were significant differences with time. Specifically, significant degenerative change was confirmed from 5 years after surgery (Fig. 3). However, there was no significant change in the mechanical axis and joint line convergence angle (Table 4).
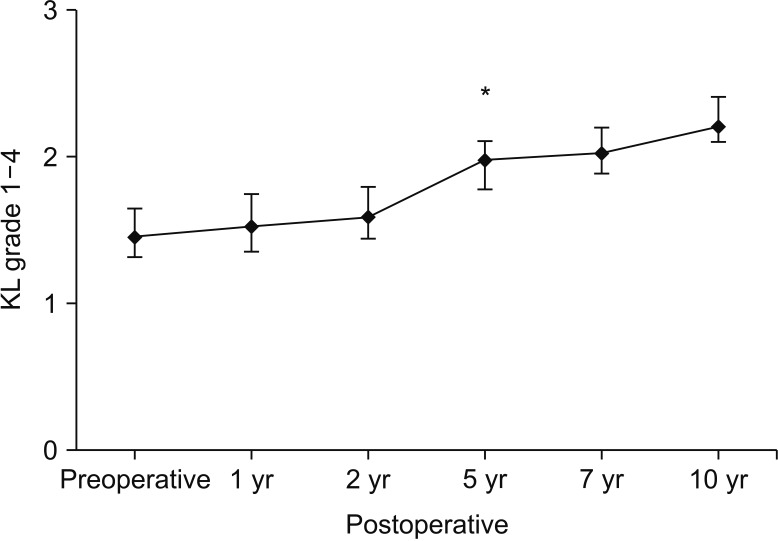 | Fig. 3Changes in Kellgren-Lawrence (KL) grade. There were significant changes with time. The significant degenerative change was confirmed from 5 years after surgery (*).
|

Survivorship Analysis
Four patients underwent conversion TKA during the follow-up period; none underwent UKA or HTO. The mean duration of conversion to TKA after microfracture was 7.1 ± 2.3 years (range, 4.8 to 10.5 years) (Fig. 4).

Go to :
DISCUSSION
The most important finding of this study is that the clinical results of microfracture of knee chondral lesions in middle-aged patients showed the best improvement at postoperative 1 year but gradually worsened thereafter until postoperative 10 years. The clinical scores at 2, 5, and 7 years after surgery were also higher than the preoperative scores; however, the scores were lower than the 1-year postoperative scores. Furthermore, the clinical scores at 10 years after surgery were similar or lower than the preoperative scores. Radiological results assessed by KL grade remained stable until postoperative 5 years, after which there was a tendency of deterioration.
Data on the clinical outcomes after microfracture for chondral lesions in middle-aged patients are limited, whereas studies on traumatic lesions in athletic or young patients have been frequently reported. Steadman et al.9) reported that the Lysholm and Tegner scores at 11 years after microfracture were significantly improved and the degree of pain was significantly decreased compared with the preoperative scores. In this retrospective study, patients younger than 45 years were included and all the chondral lesions were caused by trauma. Similarly, in a long-term study (15 years) of young athletes, Gobbi et al.7) concluded that microfracture had benefits for younger patients and small lesions. Therefore, these two studies suggest that the healing outcomes could be more favorable in younger patients with fresher tissues than those in our patients who had a mean age of 51 years and degenerative changes. In other words, older age and progression of arthritis could be associated with deterioration and worsening of outcomes. The results of the present study can be also supported by the results from other studies. Kreuz et al.4) divided patients into groups by age and concluded that those older than 40 years had deterioration over time during a mid-term follow-up. In a 10-year follow-up study, Bae et al.10) reported that the survival rate of microfracture, performed in patients with comparably older age (mean, 57 years; range, 41 to 71 years), decreased to 67.9% at 10 years compared with 88.8% at 5 years.
Asians are commonly exposed to high-flexion activities such as kneeling, squatting, and cross-legged sitting for cultural reasons. During high flexion, excessive compressive pressure is generated at all compartments of the knee joint, leading to accelerated degeneration of cartilage.19) Still, there have been no studies comparing the outcomes of microfracture between Asian and Western patients. Therefore, we have no choice but to refer to studies on middle-aged Western patients to estimate differences with Asian patients. A study with an average of 36-month follow-up period showed no deterioration in clinical scores but a high reoperation rate of 22% (18/81).11) Another study with an average of 23-month follow-up showed early deterioration of ICRS score at 36 months postoperatively.4) Interestingly, some favorable outcomes were observed in studies with Asian patients. A 36-month follow-up study in patients with a mean age of 61 years (range, 50 to 74 years) showed no deterioration in clinical scores until final follow-up.13) Another study involving patients with a mean age of 57 years (range, 41 to 71 years) showed deterioration from 5 years after surgery, and 38.1% conversion rate to TKA.10) These differences might be attributable to different demographic characteristics and life styles: middle-aged Westerners have high BMI and more sports activities. In addition, differences in study design might be responsible for different conclusions. Therefore, it is difficult to assess the effect of high flexion activities on the outcome of microfracture based on previously published studies. Further comparative prospective studies are needed.
There are several studies on the early and mid-term success of microfracture in the knee joint.56111224) A retrospective study with a large cohort (350 patients) who were followed up for an average of 4 years after microfracture found that the functional parameters improved over the first 2 years and plateaued thereafter.24) A recent retrospective study of 102 knees reported that all functional parameters showed excellent improvements at the mid-term follow-up (mean, 5.7 years) after microfracture.12) In addition, in a systematic review of 5-year outcomes, Kraeutler et al.6) confirmed the equivalence of microfracture and first-generation autologous chondrocyte implantation in terms of clinical outcomes and reported similar failure rates of 18.5% and 17.1%, respectively. These results are similar with those of the present study. Although there were deteriorations during the follow-up, the outcomes at 5 years after surgery were considered favorable when compared with the preoperative functional scores.
A recent pooling of data in the form of systematic reviews and meta-analyses has demonstrated that cartilage defect-related factors correlate with outcomes after microfracture.825262728) Mithoefer et al.27) reported a significantly higher rate of return to sports in athletes with defects < 2 cm2 compared with that in athletes with larger lesions. In the current study, we selected only patients in whom full-thickness chondral lesions were diagnosed clinically and confirmed by arthroscopy, and microfracture was not performed for any lesions greater than 5 cm2. The average size of the lesions was 3 cm2 (range, 1 to 5 cm2). Gill et al.29) reported that the treatment of chondral defects with the microfracture technique had better results when the size of the lesion was less than 4 cm2, showing a trend of less pain at final follow-up. Although there were long-term deteriorations, the favorable outcomes observed at the midterm follow-up in our study are consistent with the results of the authors.29)
Although studies that used X-ray measurement to determine outcomes after microfracture were rare due to the limitation of the method in the evaluation of cartilage, some important findings were reported according to previous studies.1011) One mid-term follow-up study showed that the mechanical axis before surgery was related with the survival rate of microfracture.11) Another study reported that preoperative alignment on X-ray affected degenerative osteoarthritic change of the knees in follow-up X-ray.10) In the present study, radiological arthritic progression was observed from 5 years after surgery. The KL grade showed a significant change in the higher grades at 5 years after microfracture, and this tendency continued until last follow-up. Considering that X-ray is the first tool for evaluating outcomes during the follow-up periods, this finding, along with previously reported results, seems to be helpful in predicting the prognosis of patients.
This study has several limitations including its retrospective nature, small sample size, and lack of a control group. The number of patients decreased over the follow-up period: only 12 patients were available for evaluation at the 10-year follow-up. Furthermore, patients with more symptoms tend to revisit the outpatient clinic more frequently and longer. Despite these limitations, meaningful conclusions could be drawn from the natural clinical course of the disease and treatment in a typical patient population consisting of middle-aged Asian patients between 40 and 60 years, which has not been dealt with in previous controlled studies. Another limitation of our study is the lack of objective outcomes data such as the results of second-look arthroscopy or histologic biopsy findings. In our center, second-look arthroscopy is not regularly performed in patients who receive microfracture without any complication. Instead, MRI was performed to check the cartilage status and to evaluate the MOCART score. However, in the current study, MRI findings did not correlate with clinical scores. One of the reasons is that morphological MRI parameters could not be completely reliable due to lack of other specific combined factors visible on MRI such as inflammation, nerve growth, and increased vascular penetration. In addition, clinical outcomes are influenced by other demographic and environmental factors such as age, BMI, defect size, and joint degeneration.30) Therefore, more accurate radiological scales in correlation to clinical outcomes should be developed. Finally, serial analysis of joint space with X-ray based on KL grade could have some limitation in patients who underwent meniscectomy. These patients generally show joint space narrowing over time. Therefore, it is difficult to exactly determine whether breakdown of the healed cartilage or inadequate meniscal coverage is the main cause of joint space narrowing. In future studies, patients should be classified according to the procedure combined with microfracture.
Most patients showed more than 50% of defect filling at 2 years after surgery in MRI. The clinical results of microfracture of knee chondral lesions in middle-aged patients showed the best improvement at postoperative 1 year but gradually worsened thereafter until postoperative 10 years. Radiological arthritic progression was observed at 5 years after surgery.
Go to :
 XML Download
XML Download