

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Aging is a natural process that is one of the stages of human growth and development. Improvement in living conditions, health care, longevity, and life expectancy has been associated with aging phenomenon in societies.12 The series of changes that occur by increasing the age, especially in the aging period, comprise the main issues of this transition period, including: death of the relatives along with loss of power, life goals, and physical skills.3 Since the aging phenomenon affects all aspects of human life addressing its challenges and adopting appropriate policies to improve physical, social, and mental status of the elderly is crucial.13
Women are confronted with specific issues arising from their physiological conditions. One of these issues is the menopausal transition during which women experience additional problems due to the reduction in estrogen.4 Menopause is part of the critical phases of a woman's life, which characterizes the transition from fertility to infertility.5 Menopause is inevitable and goes back to the early history of human creation. Its occurrence in women has been associated with different cultural, economic, and religious attitudes.67 With aging in women and the occurrence of menopausal phenomena, changes in their various dimensions of health, will occur (physical, psychological and various types of diseases) therefore, with regard to these changes, the elderly menopause is vulnerable and decrease quality of life.8
Aging is a critical period of life, and considering the problems and needs of this stage is a social necessity. However, health promoting behaviors and quality of life are important issue that have been neglected.9 Latest resources introduce quality of life as degrees of satisfaction and achieving the needs in physical, social, psychological, structural, behavioral, and activity related domains, and more importantly the feeling of well-being.1011 Quality of life assessment in clinical trials lead to closer ties between patients, physicians, and health care providers that consequently increases patients' awareness of their diseases, familiarize people with their health conditions and the advantages and disadvantages of different treatment, and emphasizes on the role of patients in choosing therapeutic approaches.12 Therefore, considering quality of life and the influence of psychology and lifestyle can increase the efficiency and independence of the elderly significantly, and help them to manage multiple complications and various treatments in the aging period.13 Quality of life is a subjective component of welfare, and in elderly means more emphasis on social policy, and reforming social goals in order to establish productive life for the elderly.14 Quality of life in elderly is largely dependent on the social environment in which they live. This issue is affected by physical, psychological and social changes in this period. Especially since the elderly menopause have been identified as a vulnerable population, and are one of the sections of society that comprise most of the healthcare services due to their chronic and acute diseases.1516 Quality of life is often characterized by objective and subjective dimensions. The objective dimensions include standard of living, income, education, health, economic status, and social interaction. While the subjective dimensions comprise life satisfaction, happiness, and the value with which a person lives.17 Based on the statistics, the proportion of elderly population in rural areas are higher than urban areas than urban areas, especially due to the migration from rural to urban areas. In fact, many rural residents are in elderly age. This issue affects the quality of life in rural areas.18 It seems elders who live in rural areas are at the risk of reduced quality of life compared to those who live in urban areas, especially because of the economic and social factors. Therefore, considering the needs of the elderly with respect to their regional, cultural, social, and economic differences seems necessary, in order to provide appropriate planning for them.19 The present study aimed to compare the quality of life of elderly living in urban and rural areas of Abadeh city (Iran).
Go to : 
Materials and Methods
This descriptive, cross-sectional study was conducted to evaluate the quality of life of elderly menopause living in urban and rural areas of Abadeh city (Iran). The two-stage (systematic random classification) and objective-based sampling methods were utilized in this study. By referring to health centers in 312 and 68 elderly menopause were selected in urban and rural areas, respectively, through systematic random sampling. It is necessary to mention that the sample size of 380 elderly menopauses was calculated according to the following formula:
The researcher then referred to their homes and if the elderly menopause met the inclusion criteria and provided the consent to answer the questions, were included in the study.
The inclusion criteria were as follows: aged more than 60 years; living in urban or rural areas of Abadeh city at the time of data collection; and providing the consent to participate in the study. While those who were severely ill (need to be hospitalized), had hearing problems, were guests from other regions of the country, had foreign nationality and cognitive disorders were excluded from the study. In order to collect data, the researcher admitted to the homes of elderly menopause, and after getting informed about their characteristics, if they met the criteria for inclusion, gave them necessary information about the aims of the study and get their informed consent. After selecting the eligible participant, the researcher was introduced to them and the objectives of the study were elaborated for the participants. The informed consent was obtained from the subjects and they were assured that their information will remain confidential.
The questionnaires were then filled with the interview method. The information was collected using Leiden-Padua questionnaire (LEIPAD) for assessment of quality of life in elderly along with demographic information questionnaire. LEIPAD questionnaire was developed in 1998 by De Leo et al.20 and can be easily used as an international tool in all seniors' groups in different communities. The questionnaire has 31 questions that evaluate the quality of life of the elderly menopause in seven dimensions of physical function, self-care, depression, anxiety, cognitive function, social function, sexual function and satisfaction with life. The questions in this questionnaire are scored with Likert scale and the responses are scored from zero (poor condition) to three (very good). The highest score in this questionnaire is 93.20 This questionnaire was translated and standardized in Iran by Sajadi and Biglarian,21 and its validity and reliability was confirmed (α = 0.874). Preliminary data were analyzed by SPSS version 21 (IBM Corp., Armonk, NY, USA) software, along with descriptive indices (mean, standard deviation, frequency, etc.,) independent t test, Scheffe test, and ANOVA.
Go to :
Results
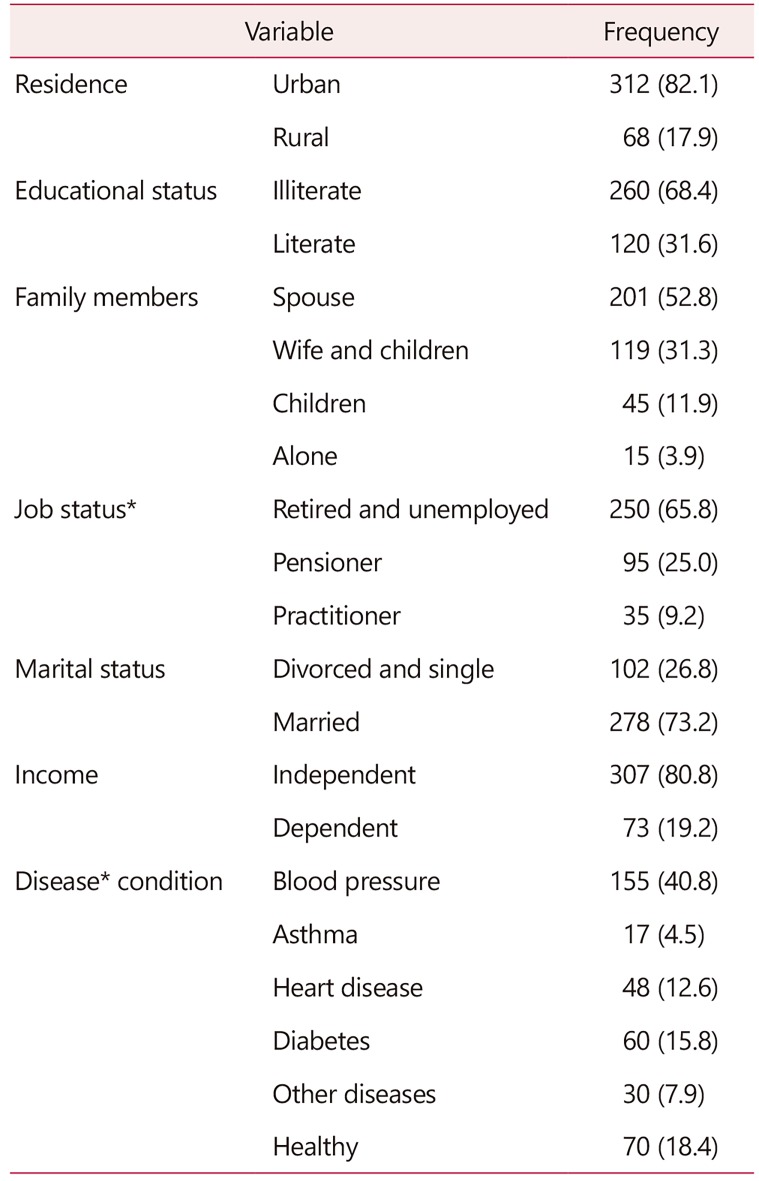
Based on the findings, of total 380 participants, 312 were from urban areas, while 68 participants were from rural areas and none of the samples were excluded from the research. In addition, 278 persons were married individuals, and 102 persons were widows and/or single. Other demographic information is provided in Table 1.
Among the demographic characteristics, there was a significant relationship between the quality of life of the elderly and the job status, disease status, and age (P < 0.05). there was no significant relationship with marital status, gender, residence, educational status, and family members (P > 0.05).
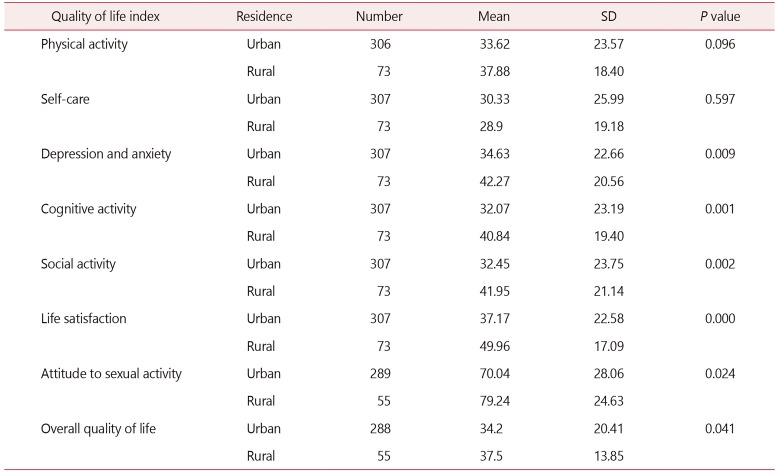
Comparing the quality of life and its dimensions including physical activity, self-care, depression, anxiety, cognitive function, social function, life satisfaction, and sexual activity revealed that the overall average of quality of life in rural and urban areas were 37.5 and 34.2, respectively, and the difference was not statistically significant. However, there was significant difference in the mean score of depression and anxiety, cognitive function, social function, life satisfaction, and sexual activity in urban and rural elderly menopause. The mean cognitive function was 40.84 in rural and 32.7 in urban elderly menopause.
The mean scores of depression and anxiety dimension were 42.27 and 34.63 in ruarl and urban areas, respectively, while the respected values were 41.95 and 32.45 for social dimension in these groups. The mean scores in life satisfaction and sexual activity dimensions were 49.96 and 79.24 in rural areas, and 37.17 and 70.04 in urban areas, respectively. As it was noted, the difference between these values was statistically significant. The values in rural areas were higher than urban areas (Table 2).
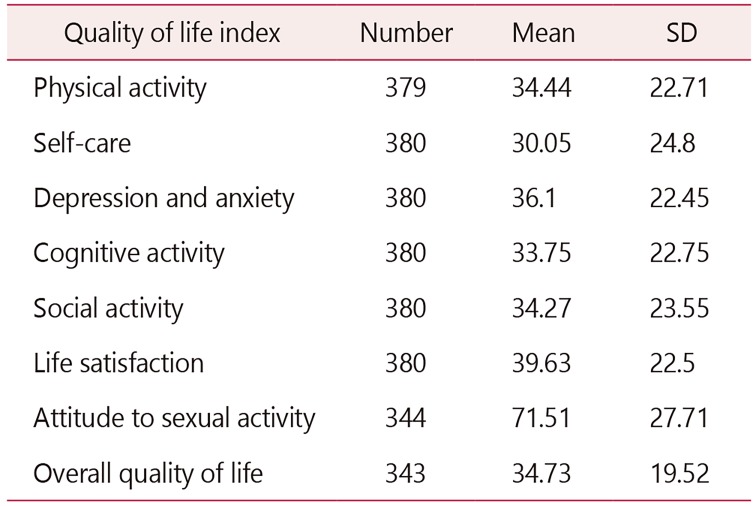
As it is shown in Table 3, the score of quality of life in elderly menopause was highest in the attitude to sexual activity (71.51) and lowest in self-care (30.05). The results of Pearson correlation coefficient test, regarding the relationship between demographic characteristics and quality of life indicated that there is a statistically significant association between age and total score and domains of quality of life. In fact, as the age increases the quality of life decreases (P < 0.001). While the results suggested that the only significant difference is between the total score of quality of life and the domains of depression and anxiety, cognitive function, social function, life satisfaction, sexual attitude, and the disease condition (P < 0.001).
The overall score of quality of life and its dimensions in various occupational groups shows a statistically significant difference (P < 0.001). However, this relationship was only observed in dimensions of cognitive function, social function, and sexual attitude. The findings demonstrated that significant difference with companions in the home is only in domains of cognitive function, social function, life satisfaction, and sexual attitude (P < 0.001). But independent t test revealed that there is a statistically significant difference in sexual attitude and marital status (P < 0.001).
Go to :
Discussion
Comparing the quality of life and its dimensions including physical activity, self-care, depression, anxiety, cognitive function, social function, life satisfaction, and sexual activity revealed that the difference in overall average of quality of life in rural and urban areas was not statistically significant. While the mean score of depression and anxiety, cognitive function, social functioning, life satisfaction and sexual activity in urban and rural elderly menopause showed a statistically significant difference. It seems that the lack of significant difference in overall quality of life in urban and rural areas' residents is due to the proximity of the urban and rural districts in Abadeh city. Another study by Zhou22 in China indicated that by comparing quality of life in urban and rural areas, all aspects of quality of life, except public health, were lower in rural population than urban population.
In another study it was found that the difference between the quality of life in urban and rural areas is related to socio-economic factors, lack of trust in health services, and lack of similar attitude to independence in villages that leads to growing dissatisfaction of quality of life in rural elderly menopause.23 In study Kelekçi et al.24 found that vulvar dermatoses was particularly significantly associated with decreased quality of life. Another research on comparing urban and rural lifestyle in Chinese elderly population demonstrated that the quality of life in is lower in village than the city, and rural menopause have higher symptoms of depression due to solitude that consequently can lead to lower quality of life in these menopause.25 In terms of significant association between domains of social activity in both groups, Baernholdt et al.26 suggested that the domain of social activity is inferior in rural seniors compared to urban elderly.
The results of Pearson correlation coefficient regarding the relationship between age and quality of life indicated that there is a significant and inverse association between age and all aspects of quality of life along with overall score of quality of life. Similarly, Mohaqeqi Kamal et al.27 suggested that quality of life is significantly and inversely associated with age in elderly people. In evaluation of the relationship between marital status and quality of life the findings showed a significant relationship between marital status and sexual activity dimension. In fact the mean score of sexual activity among the married elderly (18.84) was higher than widow and single seniors (15.67). In line with previous research, Alipour et al.28 suggested that the average scores for overall quality of life is higher in married elderly people. They believed this is associated with more supporting networks in married people.
However, this association has not been confirmed in Mohaqeqi Kamal et al.27 and Khalesi29 studies. Regarding the association between gender and quality of life of the elderly, consistent with Ahmadi et al.'s study,30 the findings of the present study indicated that the overall quality of life score is not significantly associated with gender. In addition, quality of life in social relations' dimension was higher in women compared to men which corroborates Apidechkul31 findings. In terms of the association between level of education and quality of life in elderly menopause, in most domains (cognitive function and social activities) there was a statistically significant relationship. In fact, most elderly people with higher educational levels had higher average scores compared to those with lower levels of education. This finding match previous research that considered education as a crucial factor in dynamic elderly lifestyle.32
The results of this study showed that there the overall quality of life score and scores of physical activity, self-care, depression and anxiety, cognitive function, life satisfaction, and sexual activity dimensions had significant difference in various occupational groups. The Scheffe test indicated that in domains of physical activity, depression and anxiety, and cognitive function the scores of pensioners and working people has no significant difference, while the scores of retired people were higher than them. These findings are consistent with Rezvani et al.'s study.33 In the study of Shirvani and Heidari,6 the mean total score of quality of life of member of the association was significantly greater than non-members of the elderly support association.
Cross-sectional design of the study along with its dependency to the time and place of the interview and mood states of the elderly are amongst the limitations of this study. For further research, it is suggested that investigation be conducted in larger communities, and the comparison be performed on elderly people living in urban and rural areas and those living in nursing homes.
Despite the impact of various variables on quality of life of elderly menopause in urban and rural areas, by implementing specific plans to improve the quality of life of elderly, including social and economic support, and providing appropriate conditions for them to fulfill their emotional and psychological needs effective steps can be taken to enhance the quality of life of elderly menopause in urban and rural areas, and minimize the negative impacts of these variables on their lives.
Go to :
 XML Download
XML Download