

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Aortic valve stenosis (AS) is the most common valvular heart disease in the elderly.12 Although surgical aortic valve replacement (SAVR) has been the treatment of choice to correct significant AS, the use of trans-catheter aortic valve implantation (TAVI) for the management of AS has been rapidly growing, and its indications have been widely expanded to intermediate and even low-risk patients for SAVR.34567
Current risk scores, such as the European System for Cardiac Operative Risk Evaluation (EuroSCORE) II and Society of Thoracic Surgery (STS) score, which were initially developed to predict early results after surgery, have been proven to be effective in predicting long-term outcomes after cardiac surgery89 and currently are used in the decision-making process between SAVR and TAVI.
In addition to these specialized risk score models for cardiac surgical patients, frailty has been suggested to be a major factor influencing patients' outcomes.10 Frailty is a state of increased vulnerability to poor resolution of homeostasis after a stressor event, which increases the risk of adverse outcomes.11 The frailty index (FI) was designed to quantify the variability in frailty status and various FI types have been introduced.12 Among the various scales, the FI based on routine laboratory data (FI-L), blood pressure and pulse rate was proven to be significantly associated with all-cause mortality during a 9-year follow-up and was as effective as the FI based on self-reported clinical features.13 The FI-L has advantages compared with other frailty measures; 1) it could be easily obtained from preoperative vital signs and blood sample tests without further examinations, 2) it is highly versatile and reproducible because it is determined by totally objective manner, and 3) it can reflect subclinical conditions which emerges only subtle changes in laboratory tests.
Because recent guidelines suggested age (≥ 75 years) as one of the significant factors to favor TAVI during the discussion in the heart team,6 this study hypothesized that frailty rather than the patient's age might be more important in the decision-making process for elderly patients. Therefore, the present study was conducted to evaluate the predictive value of FI-L on clinical outcomes after SAVR in elderly patients.
METHODS
Patient characteristics
From January 2001 to June 2018, 154 patients who were 75 years or older underwent primary SAVR at our institution and were enrolled in the present study. Patients who underwent concomitant valvular heart surgery and those with infective endocarditis were excluded. The etiologies of aortic valve disease were AS and aortic regurgitation in 141 and 13 patients, respectively. The mean age at the operation was 78.7 ± 3.6 years, and 78 patients (50.6%) were men. The mean EuroSCORE II and STS scores were 3.6 ± 2.5 and 3.7 ± 2.4, respectively. Twenty-six patients (16.7%) were in New York Heart Association functional classification III–IV. The baseline characteristics of the enrolled patients are summarized in Table 1.
Table 1
Preoperative characteristics and risk factors

Values are presented as mean ± standard deviation or number (%).
STS = The Society of Thoracic Surgeons, EuroSCORE = European System for Cardiac Operative Risk Evaluation, NYHA = New York Heart Association, FI-L = frailty index based on routine laboratory data, COPD = chronic obstructive pulmonary disease.
aA glomerular filtration rate < 60 mL/min/1.73 m2 for more than 3 months.
![]()
Surgical procedures and operative data
All operations were performed through median sternotomy. Bovine pericardial and porcine valves were used in 126 and 28 patients, respectively, with sizes ranging from 18 to 27 mm. Concomitant procedures included coronary artery bypass grafting (n = 28), ascending aorta replacement (n = 23) and arrhythmia surgery (n = 10). The mean cardiopulmonary bypass and aortic cross-clamp times were 183 ± 77 and 111 ± 38 minutes, respectively (Table 2).
Table 2
Operative data

| Variables | Total (n = 154) | |
|---|---|---|
| CPB time, min | 183 ± 77 | |
| ACC time, min | 111 ± 38 | |
| Concomitant procedures | ||
| Arrhythmia surgery | 10 (6.5) | |
| Aorta surgery | 23 (14.9) | |
| Coronary artery bypass grafting | 28 (18.2) | |
Values are mean ± standard deviation or number (%).
CPB = cardiopulmonary bypass, ACC = aortic cross-clamp.
![]()
FI-L calculation
The concept of FI-L was started with the view of seeing frailty as a state of impaired health arising from the accumulation of health deficits. The FI-L was calculated as a proportion of variables showing abnormal results out of 32 preoperative parameters based on blood and urine tests and the blood pressure and pulse rate (Supplementary Fig. 1).13 Median 28 (range, 26–32) variables could be obtained from study patients. Normal reference ranges for each variable as demonstrated in the Supplementary Fig. 1 were used to code each deficit as binary fashion. Each patient's FI-L score was calculated as the number of deficits present divided by the total number of deficits measured. Therefore, the FI-L score shows a quantitative measure of health deficits. A higher score indicates greater frailty.
Evaluation of clinical outcomes
Operative mortality was defined as any death within 30 days after surgery or during the same hospitalization. Postoperative follow-up was performed regularly on an outpatient basis with 3- to 4-month intervals. Patients who did not visit the clinic at the scheduled time were contacted by telephone to confirm their condition. In addition, data for the vital status and death from cardiovascular diseases were obtained from death certificates available at Statistics Korea. Clinical follow-up was closed on June 30, 2018. The median follow-up duration was 40 months (interquartile range [IQR], 15–74 months). Aortic valve-related events (AVREs) were defined based on the guidelines as follows14: cardiac death, structural valve deterioration, nonstructural valve dysfunction, valve thrombosis, embolism, bleeding event, and prosthetic valve endocarditis.
Statistical analysis
The statistical analyses were performed using the IBM SPSS statistical software version 23.0 (IBM Corp., Armonk, NY, USA), STATA version 12.0 (StataCorp, College Station, TX, USA) and SAS V.9.2 (SAS Institute, Cary, NC, USA). The data are expressed as the means ± standard deviations, medians with IQR or proportions. Comparisons of categorical and continuous variables were performed with the χ2 test or Fisher's exact test and Student's t-test or the Mann-Whitney U test, respectively. Time-related events were estimated using the Kaplan-Meier method and risk factors were analyzed using the Cox proportional hazards model. The proportional hazards assumption was checked by log-minus-log plots of survival functions for categorical variables or time-dependent covariates in the Cox model. Restricted cubic splines were used to check the assumption of linearity between continuous variable and its log hazard. Variables with P < 0.050 in the univariate analyses were entered into the multivariable models, and multicollinearity was controlled using backward stepwise regression. Discrimination ability for death was evaluated with Harrell's C-statistics from the jackknife method in the somersd package of STATA (StataCorp) and concordance index (C-index) was presented.15 The minimal P value approach was used to estimate an optimal cutoff value of a continuous variable predicting a time-related event.16 A P < 0.050 was considered statistically significant.
RESULTS
Early results
The mean patient FI-L was 20% ± 10.4%. The operative mortality rate was 3.9% (6 of 154 patients). The causes of death were low cardiac output syndrome (n = 2), sepsis (n = 3), and acute bowel ischemia (n = 1). Postoperative complications included new-onset atrial fibrillation (n = 45), respiratory complications (n = 15), and acute kidney injury (n = 13) (Table 3). One patient required a second-run cardiopulmonary bypass to correct a significant paravalvular leak detected on intraoperative transesophageal echocardiography. A paravalvular leakage was detected by postoperative transthoracic echocardiography in 6 patients, but the grade was trivial in all cases. One patient needed permanent pacemaker implantation on the 16th postoperative day due to a complete atrioventricular block after surgery.
Table 3
Early clinical outcomes

Data are presented as number (%).
LCOS = low cardiac output syndrome.
aDrawn from 129 patients who had no atrial fibrillation preoperatively; bAn increase of > 50% in serum creatinine level from the preoperative value; cCardiac index < 2.0 L/min/m2 or a systolic arterial pressure < 90 mmHg requiring inotropic support (dopamine or dobutamine) of > 5 mcg/kg per minute; dPostoperative pneumonia or prolonged ventilator support over 48 hours.
![]()
Long-term outcomes
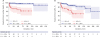
During follow-up, late deaths occurred in 29 patients including 9 cardiac deaths. The overall survival (OS) rates at 5, 10, and 15 years were 83.3%, 59.0%, and 41.6%, respectively (Fig. 1A). The AVREs occurred in 28 patients. The paravalvular leak disappeared in 5 out of 6 patients on follow-up echocardiography. In the other patient, it remained as less than moderate degree during the 1-year follow-up after surgery. Bleeding events and embolic stroke occurred in 6 and 4 patients, respectively. Aortic valve reoperation was required in only one patient due to prosthetic valve endocarditis 31 months after surgery. One additional patient was diagnosed with infective endocarditis, which was successfully managed with antibiotic therapy. The freedom rates from AVREs at 5, 10, and 15 years were 79.4%, 72.7%, and 52.9%, respectively (Fig. 1B).

Impact of the FI-L on early and late outcomes
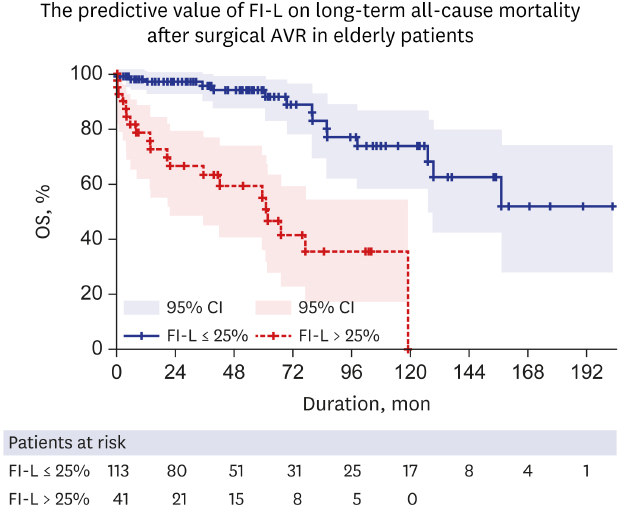
Univariate analyses demonstrated that chronic kidney disease (P = 0.009), diabetes mellitus (P = 0.030), EuroSCORE II (P = 0.009), STS score (P = 0.007), and FI-L (P = 0.002) were associated with early mortality. The Cox proportional hazards analysis showed that the FI-L was a significant factor associated with OS (Table 4). The C-index for OS was 0.767 for FI-L. Among 32 variables included in the FI-L, diastolic blood pressure (P = 0.034), serum bicarbonate (P = 0.002), calcium (P = 0.029), blood urea nitrogen (P = 0.009), albumin (P = 0.004), total bilirubin (P = 0.021), hemoglobin (P = 0.003), and glycohemoglobin (P = 0.014) levels were significant factors associated with OS. The C-index increased up to 0.825 when it was calculated from combined EuroSCORE II and FI-L. When the FI-L was combined with the STS score, the C-index increased up to 0.827 (Table 5). A minimal P value approach demonstrated that a FI-L of 25% was the best cutoff value to predict all-cause mortality after SAVR (Fig. 2). When the clinical outcomes were compared based on the FI-L, frail patients (FI-L > 25%) had higher rates of operative mortality (12.2% vs. 0.9%, P = 0.005) and cardiac death (P < 0.001) and AVRE (P < 0.001) during the follow-up (Table 6 and Fig. 3).
Table 4
Risk factor analyses for overall survival

CI = confidence interval, EuroSCORE = European System for Cardiac Operative Risk Evaluation, STS = The Society of Thoracic Surgeons, FI-L = frailty index based on routine laboratory data
![]()
Table 5
C-index for overall death
| Variables | C-index | 95% CI |
|---|---|---|
| FI-L | 0.767 | 0.681–0.852 |
| EuroSCORE II | 0.723 | 0.637–0.809 |
| STS score | 0.741 | 0.654–0.828 |
| FI-L and EuroSCORE II | 0.825 | 0.758–0.891 |
| FI-L and STS score | 0.827 | 0.764–0.890 |
C-index = concordance index, CI = confidence interval, FI-L = frailty index based on routine laboratory data, EuroSCORE = European System for Cardiac Operative Risk Evaluation, STS = the society of thoracic surgeons.
![]()
 | Fig. 2Kaplan-Meier curves for OS according to the cutoff value of the frailty index (FI-L).OS = overall survival, CI = confidence interval, FI-L = frailty index based on routine laboratory data.
|
Table 6
Comparisons of early and long-term clinical outcomes according to the FI-L
Data are presented as number (%).
FI-L = frailty index based on routine laboratory data, LCOS = low cardiac output syndrome.
aDrawn from 30 and 99 patients in the FI-L > 25% and FI-L ≤ 25% groups, respectively, who had no atrial fibrillation preoperatively.
![]()
DISCUSSION
The present study demonstrated two main findings. First, the early and long-term outcomes of SAVR in the elderly patients were favorable with early mortality and 10-year survival rates of 3.9% and 59%, respectively, and low incidences of paravalvular leak and permanent pacemaker implantation after surgery. Second, the FI-L was significantly associated with early and long-term mortality after SAVR in elderly patients.
Since the first report in 2002, the indications for TAVI have been expanded from high or prohibited surgical risk patients to intermediate and even low-risk patients for SAVR in current clinical practice.317 In addition, recent guidelines suggested age (≥ 75 years) as one of the significant factors to favor TAVI during the discussion in the heart team.6 However, previous studies demonstrated favorable early and long-term results after SAVR even in octogenarians,18192021 with early mortality rates from 5.5% to 9% and 5-year survival rates of approximately 70%. The early and long-term outcomes in the present study were in agreement with those of previous studies with operative mortality and 5-year survival rates of 3.9% and 83.3%, respectively.
In addition to age, the concept of frailty has emerged as one of the risk profiles especially in the elderly. Evidences has shown a significant association between the frailty and clinical outcomes in elderly cardiac surgical patients, which have also been growing very recently.222324 However, current models such as the EuroSCORE II and STS, included age but not frailty as a major risk factor for mortality and major morbidity after cardiac surgery.
The Frailty in Aortic Valve Replacement study22 is the largest prospective study to date to investigate the impact of frailty scales on outcomes after surgery in elderly patients undergoing SAVR or TAVI. The authors suggested that a brief 4-item scale outperformed other frailty scores and was recommended for use in this setting. However, the assessment of frailty should not rely on a subjective method. In the present study, the FI-L was selected from the various frailty scales for several reasons. It is an accumulation of different objective estimates as biomarkers of frailty. The validity of the FI-L in evaluating the frailty status has been proven in previous studies.1325 The FI-L is convenient and feasible using only existing preoperative data. Finally, it could be adopted in any retrospective studies like the present study. Our study clearly showed that the FI-L was significantly associated with early and long-term outcomes after SAVR in elderly patients. The minimal P value approach showed that a FI-L of 25% was the best cutoff value for predicting poor outcomes after SAVR. The C-index for OS was better with FI-L (0.767) than current risk model (EuroSCORE II). The C-index was increased when converging FI-L and EuroSCORE II in both early and long-term predictions of survival. Therefore, in addition to the current risk scores and age itself, the FI-L should be considered in the decision-making process between the SAVR and TAVI for the elderly.
There are several limitations that must be recognized in the present study. First, this study was a retrospective observational study conducted at a single institution. Second, the number of patients enrolled was relatively small to draw definitive conclusions. Third, multivariable analysis for the early mortality was not presented because the number of events was too small to run adequate analysis for this outcome. Fourth, only SAVR patients were enrolled and the results were not compared with those of TAVI patients. Further study might be needed if the FI-L could be a useful tool in decision making process between SAVR and TAVR.
In conclusion, frailty score but not patients' age is significantly associated with early and long-term clinical outcomes after SAVR in the elderly patients equal or more than 75 years. Combining frailty score to current risk scores might be helpful to predict long-term outcomes after SAVR in elderly patients.
 XML Download
XML Download