

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
After small bowel resection, when the remnant bowel is less than 200 cm long and concludes with an ostomy (thus lacking colonic continuity), the incidence of high-output stoma (HOS) is high [1]. The definition of HOS remains controversial, but an effluent volume exceeding 2,000 mL/day is considered clinically significant in terms of possible complications [23]. These complications include electrolyte abnormalities, renal dysfunction caused by water loss, and malabsorption-induced weight loss [4]. Management of complications and maximization of patient outcomes require successful adaptation of the remaining small bowel [5]. The extent of intestinal adaptation varies by the residual bowel length and sites of resection; however, pharmacological and nutritional therapies improve the performance of the remnant bowel. Antimotility agents are commonly used to maximize absorption by controlling intestinal transit time, and antisecretory agents are employed to reduce gastric acid secretion and nutrient loss caused by diarrhea. Nutritional therapy seeks to decrease stool volume and improve consistency; individualized dietary plans are based on the patient's nutritional requirements, considering hydration and possible parenteral nutrition (PN). A comprehensive long-term plan for life after discharge is essential, and nutritional education following the dietary guidelines for ostomy patients should be offered.
The ostomy nutrition guide [6] recommends a low-residue/high-protein diet commencing immediately after surgery and a regular diet resumed as soon as the bowel adapts. In the transitional period, small meals every 3–4 hours and consumption of 6–8 cups of water/day are recommended. At 6–8 weeks after surgery, fiber-containing foods should be started, and new foods should be tested in terms of intestinal rehabilitation. In particular, a patient who has a short bowel after an ostomy may require a dedicated dietary strategy. When HOS is in play, avoidance of sugary beverages and consumption of hypertonic fluids instead of water are important. As the small bowel is short, adaptation takes longer; inclusion of high-fiber vegetables in the diet may need to be delayed. Multivitamin/mineral supplementation should continue until a regular diet is tolerated.
Multidisciplinary management is required to ensure patient recovery and a good quality of life [3]. In the long term, dietitians must be alert to nutritional deficiencies and dehydration, and revise the nutrition care plan and education accordingly. Adults with particular dietary habits may find it difficult to adhere to new dietary guidelines; repeated nutritional education (not just single sessions before and after discharge) is important. Moreover, home nursing (PN and caring for the stoma) may be needed to manage the patient's general condition [7]. A nutrition support team (NST) plays pivotal roles not only in acute care but also home care settings [1].
This case report shares our experience with the nutritional management of HOS after a patient with Crohn's disease underwent extensive small bowel resection. The study was approved, and the need for informed consent waived, by the Institutional Review Board of the Seoul National University College of Medicine (approval No. 1905–174–1036).
CASE
A 42-year-old male whose Crohn's disease had been controlled with medications for more than 19 years visited the emergency room (ER) with small bowel dilation and mechanical ileus in October 2018. Emergency surgery was performed because the ileus became exacerbated and small intestinal perforation was suspected. A severe adhesion and a fistula were found at the 200 cm point (in the Treitz ligament) and another severe adhesion was evident in the distal ileum. Bowel segments about 80 cm in length both proximal and distal to the lesion were resected and then loop ileostomy was formed. The remaining small bowel was 160 cm in length.
Nutrition management
At the time of ER admission, an initial nutritional assessment was conducted. He was moderately malnourished based on the American Society for Parenteral and Enteral Nutrition (ASPEN)/Academy of Nutrition and Dietetics (AND) malnutrition criteria [8]. His estimated nutritional need was 25–30 kcal/kg usual body weight (UBW)/day with 1.2–2.0 g protein/kg UBW/day based on guidelines for the adult critically ill patient [9]. Because of the mechanical ileus, total PN was initiated with a target of 25 kcal/kg UBW/day and 1.4 g protein/kg UBW/day. PN was customized to prevent the development of electrolyte imbalances.
After extensive small bowel resection, the estimated energy requirement was 1,500 kcal/day (derived using the Penn State equation). In order to decrease stomal output and allow persistent luminal stimulation, continuous tube feeding with a low-residual formula (500 kcal) was initiated at 20 mL/hr over 24 hours. When he could tolerate 1,200 kcal/day at 50 mL/hr over 24 hours, he was weaned off PN (1,058 kcal/day, protein 58 g/day). According to evaluations about 1 month after surgery (postoperative day [POD] #30), he had continued to lose weight; he weighed 41.1 kg (body mass index [BMI] 13.9 kg/m2) which meant he had lost 21.6% of his body weight at admission. HOS (about 3,000 ml/day) and elevated blood urea nitrogen (24.0 mg/dL) and creatinine (1.6 mg/dL) were observed, so the risk of dehydration was high. Although on POD #30 magnesium concentration was not measured, it was 1.5 mEq/dL on POD #14, and since it was the marginal level and PN was suspended, deficiency of micronutrient was also expected. Intake via tube feeding was 1,400 kcal/day (34 kcal/kg current body weight [CBW]) and protein 56 g/day (1.35 g/kg CBW). Our NST decided to increase the enteral nutrition (EN) supply to the target calorie level and to provide supplemental PN (commercial 3-in-1 PN with multivitamins and trace elements, 345 kcal/day, protein 16 g/day) to replenish nutrients lost. Total amount supplied, including EN and PN, was 1845 kcal/day (45 kcal/kg CBW) and protein 75.8 g/day (1.85 g/kg CBW).
He commenced an oral diet 6 weeks after operation (POD #43) and was again weaned from PN. A dietitian evaluated dietary intake, and assessed stomal output volume and consistency. The estimated dietary intake was 1400 kcal/day with protein 80 g/day. The stomal output was approximately 3,000 mL/day (the bag was emptied 10 times/day) of watery diarrhea. The dietitian educated the patient on the need for frequent small meals, the sipping of fluid between meals (thus not with meals) to ensure hydration, and the avoidance of foods containing high levels of fiber and sugary beverages, which might exacerbate stomal output. Multivitamins and multiminerals were recommended. As a typical Korean meal includes a bowl of vegetable soup and several vegetable side dishes, the need to strictly avoid soup and vegetables was emphasized. The guidelines recommend commencing vegetables 6–8 weeks after operation. However, given his HOS status, a vegetable-free diet was maintained until the stomal output fell to below 2,000 mL/day, even 8 weeks after the operation. To enhance compliance and to help him understand the principles of food selection, the dietitian visited him 4 times.
As discharge approached, the dietitian conducted a nutritional re-assessment. The patient exhibited severe malnutrition based on the ASPEN/AND criteria [8]. He had lost 25.4% of his body weight and exhibited moderate loss of muscle mass and body fat. His estimated nutritional requirements were 35–45 kcal/kg UBW/day and 1.5–2.0 g protein/kg UBW/day. He was taking 1,800 kcal and 90 g protein/day but still losing weight. To increase his weight and improve his nutritional status, home PN support was recommended. The NST planned home PN three times/week (commercial 3-in-1 PN with multivitamins and trace elements, 578 kcal, protein 26 g).
When he was re-admitted 1 month after discharge (POD #106), nutritional re-assessment was performed. His percent of ideal body weight value was 71.6%, his BMI was 15.8 kg/m2, and the nutritional intake met his requirements; his nutritional status had improved compared to that 1 month earlier. His progress is summarized in Table 1.
Table 1
Summary of the nutritional interventions delivered by the nutrition support team

PN, parenteral nutrition; EN, enteral nutrition; ER, emergency room; NPO, nil per os; POD, postoperative day; ICU, intensive care unit.
![]()
The energy intakes from both EN and PN after loop ileostomy are shown in Figure 1. Two months after operation (POD #60), his body weight was 40.3 kg at discharge. He maintained the oral intake that he had established in the hospital, and received home PN, for 2 months after discharge. About 18 weeks after the operation (POD #106), he was re-admitted to manage necrosis of both feet and hands associated with use of an inotropic agent in the intensive care unit. His body weight was 46.6 kg (BMI 15.8 kg/m2), and had thus increased by 15.6% since discharge.
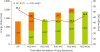 | Figure 1Changes in nutritional intake and body weight after ileostomy.OP, operation; POD, postoperative day; EN, enteral nutrition; PN, parenteral nutrition.
*Tube feeding intake; †estimated oral intake; ‡home PN (3times/week) converted into daily.
|
After ileostomy, intravenous PN and/or fluids were administered for about 18 weeks. Table 2 lists the laboratory data, stomal output volumes, and the PN infusion details. Although a large stomal output (about 3,000 mL/day) of watery diarrhea was observed in the early postoperative period, the electrolyte balance was optimized via infusion therapy. When he was re-admitted (POD #106), his stomal output was slightly reduced but the consistency had thickened significantly.
Table 2
Data after the operation of ileostomy formation

OP, operation; POD, postoperative day.
*Estimated volume: number of bag-emptying/day × one-time emptying volume.
![]()
DISCUSSION
When HOS develops after extensive small bowel resection, it can cause complications such as dehydration, electrolyte imbalances, and undernutrition [134]. Our case is a useful example of how intensive nutritional therapy can prevent such complications. Improvement of the patient’s nutritional status was essential, because not only does Crohn's disease exhibit a high rate of postoperative relapse [10], but rehabilitation is the principal treatment for limb necrosis in relatively young patients.
Intensive nutritional management allowed improvements in nutritional status, such as weight gain and maintenance of adequate hydration. To optimize results, a multidisciplinary approach (team-based care) is essential [11]. Dietitians play key roles in care [4]. Assessment of energy demand based on current nutritional status is an important feature of nutritional care. The ASPEN guidelines [8] recommend 35–45 kcal/kg/day (the need may attain up to 60 kcal/kg/day) and protein 1.5–2.0 g/kg/day for small bowel syndrome (SBS) patients with end-jejunostomies. One report described a patient who was losing weight on an intake of 2,600 kcal/day despite the fact that the estimated requirement (using the Schofield equation) for her current body weight was 1,660 kcal/day [12]. Throughout the nutrition care process, nutritional requirements should be estimated considering both the patient's intake and the volume lost in the stoma. For our case, the estimated requirement was 2,100 kcal/day (40 kcal/kg/day) with protein 103 g/day (2.0 g/kg/day) for a target body weight of 52.4 kg (the baseline weight). At about 2 months after discharge, his body weight was 46.6 kg. Thus, weight gain was observed, but the target was not attained. If the patient can tolerate it, more intensive nutritional support may be considered.
Another factor affecting outcomes is how strictly the patient follows the dietary guidelines. Strict dietary adherence decreases dependence on intravenous support [5]. Our patient took six meals daily (three regular meals and three small meals), but eschewed soup. He consumed a considerable amount of protein at every meal. He used refined grain to minimize dietary fiber intake and ate few high-fiber vegetables. Multivitamin/mineral supplements were consistently taken.
In cases of HOS caused by a short bowel, parenteral infusion therapy (fluid and/or PN) is inevitable. The need for long-term intravenous support depends on the remnant length of the small intestine, and less support may be required as absorptive capacity improves [3]. Thompson et al. [7] reported that 50% of SBS patients with Crohn’s disease require permanent home PN. Wall [5] found that a patient with about 105 cm of remnant small bowel required PN for 4 years after discharge. Our patient visited the outpatient clinic several times, but did not receive follow-up nutritional management, and appropriate infusion therapy was thus not possible. Thus, when he was re-admitted after 2 months without infusion therapy, an electrolyte imbalance attributable to dehydration was detected (data not shown). However, even after hospitalization, he refused PN support. Infusion therapy is delivered by home care nurses and may become economically burdensome in the long term. In study of Thompson et al. [7], insurance coverage was of concern to those who required home therapy, and in study of Winkler and Smith [13], home PN imposed financial hardship on families caring for patients. However, SBS patients require long-term management; their insurance coverage should alleviate the economic burden of continuing treatment.
In conclusion, nutritional therapy is essential for successful management of, and prevention of complications in, patients with HOS. The nutritional interventions include estimation of dietary requirements and education on how to reduce stomal output and the need for infusion therapy. Our present case is a good example of nutritional care for a patient with HOS.
 XML Download
XML Download