

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Infertility affects approximately 15% of all couples trying to conceive and recent studies indicate an increase in male infertility rates [1]. Male problems account for more than 40% of infertility [2]. Male infertility can have different causes, including cryptorchidism, infectious diseases, varicocele, autoimmune diseases, testicular cancer, and genetic abnormalities. However, in over 30% of cases, the causes of male infertility are not recognizable (idiopathic oligoasthenoteratozoospermia) [3]. One of the main causes of male infertility is the reduction of sperm quality [4]. Reactive oxygen species (ROS)-mediated damage, and oxidative stress plays an essential role in reducing sperm quality [5]. Under physiological conditions, a small amount of ROS is produced by the spermatozoa for the capacitation and fertilization process. However, when the concentration of ROS in the body increases, spermatogenesis process may become disorderly. Also, lipid peroxidation and oxidative stress can damage sperm DNA [6]. Through its intrinsic scavenging activities, the body can eliminate ROS and other lipid peroxidation-derived metabolites. However, excessive amounts of this metabolites in semen can overwhelm the antioxidant defense mechanisms [5].
Evidence coming from previous studies has shown that there was a link between dietary pattern and the body's antioxidant defence system [7]. Some micronutrients such as vitamin C, zinc, folic acid, carnitine, and carotenoids play an antioxidant role in the body and can reduce the level of ROS and its harmful effects on semen parameters. Some previous studies have reported that men with a high dietary intake of antioxidants have a lower frequency of sperm aneuploidy and improve sperm quality [8910]. However, the results of the studies are still contradictory. Theiaim of this study was to describe the relationship between the dietary intake of antioxidant nutrients and semen quality in infertile men.
MATERIALS AND METHODS
Study population
The present study is a cross-sectional study on infertile men with oligospermia that was conducted at Isfahan Infertility and Fertility Center, Isfahan, Iran. Study participants were recruited at admission to the center for treatment of infertility between October 2017 and January 2018. One hundred seventy-five oligoasthenospermia men were enlisted who sought infertility remedy at the Isfahan Infertility Center were selected for this study. The Ethical Committee of Esfahan University of Medical Sciences approved the study with the code of IR.MUI.RESEARCH.REC.1397.1.265 and informed consent were obtained from all participants. Patients were asked to complete questionnaires about the demographic information, medical history and fertility history, drugs, physical activity, and smoking.
The inclusion criteria were: willing to contribute, age ranges from 20 to 45 years, low sperm count (< 20 million), and motility lower than 60%, damaged morphology higher than 65% and not receiving other treatments. We excluded patients whose causes of infertility were hormonal disorders, epididymal duct obstruction, testicular atrophy, testes scrotum, azoospermia, urinary tract infection, testicular surgery, testicular tumor, anatomical abnormalities of the genital area. Also, we excluded patients with diabetes, inflammatory disease, chronic kidney, and renal disease and if they were taking hormone therapy or antioxidant supplements such as vitamin C, omega-3, resveratrol, and vitamin E. A semen sample that was produced on-site by masturbation was taken from all of the participants.
Evaluation of anthropometric indices, dietary intake
Weight (Bioelectrical Impedance Analysis, Omron BF511; Omron Healthcare, Osaka, Japan) was measured while the participants wore light clothing and no shoes with 0.1-kg accuracy. Also, height was measured with a strip meter for with 0.5-cm accuracy. The BMI was calculated by dividing the body weight (kg) by the height (m2). A validated detailed food frequency questionnaire (FFQ) [11] was used to evaluate the participant's dietary intakes. This questionnaire contains a comprehensive list of food items (106 items) that are consumed by Iranian adults. The main groups in this questionnaire include dairy products (9 items); carbohydrate-based foods (10 items); fruits and vegetables (22 items); mixed dishes (29 items); and miscellaneous food items and beverages (36 items). The frequency of food intake varied from never or less than once/month to 12 or more times per day. Eventually, the amount of consumption of each item of food was computed and converted to grams per day using household measures [12]. To obtain nutrient intakes of each participant, we used Nutritionist IV software that was modified for Iranian foods [13].
Semen analysis
Men were asked to abstain from ejaculation for at least 72 hours before sample collection. Semen samples were obtained after three days of sexual abstinence at the Isfahan Infertility and Fertility Center. Abstinence time was recorded as the time between current and previous ejaculation as reported by the study subject. Ejaculate volumes were estimated by specimen weight, assuming a semen density of 1.0 g/mL. All of the participants underwent at least 2 semen analyses, and if the difference was more than 20%, the third sample was taken. Samples were held at 37 degrees Celsius to liquefy. After liquefaction, the samples were analyzed according to the World Health Organization guideline [14]. Briefly, sperm motility was assessed by the Computer Aided Sperm Analysis system (LABOMED, SDC313B; LaboMed Gerinnungszentrum, Berlin, Germany), which defined sperm as progressive, non-progressive and immotile. Normal morphology was assessed by Papanicolaou staining [15]. For evaluation of sperm concentration, we used from by a sperm counting chamber and expressed as million/mL. In this method, after diluting the sperm sample, the sperm counting chamber was loaded with the dilution, and the spermatozoa were allowed to settle in a humid chamber. From the same dilution, two chambers of the hemocytometer were assessed and at least 200 spermatozoa per replicate were counted. Semen samples were evaluated for sperm DNA fragmentation and DNA damage by Terminal deoxynucleotidyl transferase dUTP nick end labeling assay using the in situ cell death detection kit (Roche, Mannheim, Germany) [16]. Five hundred sperms per slide were assessed under a fluorescence microscope (BX51; Olympus, Tokyo, Japan) at ×100 magnification. Sperm with red heads were considered to have intact DNA, and those with green heads were assumed to have fragmented DNA.
Statistical analyses
Outcome variables were total sperm count, sperm density, sperm concentration, total sperm motility, DNA damage, and DNA fragmentation index (DFI). Exposure variables were average daily intake antioxidants. Subjects were divided into four groups based on the amount of dietary antioxidants intake. Men with the lowest intake of each micronutrient were considered as the reference group. Linear regression was used to examine the association of each antioxidant with semen quality parameters. We used analysis of covariance (ANCOVA) to calculate adjusted semen parameters for each nutrient quartile by relevant covariates. Multivariate ANCOVA models were created with continuous semen parameters as dependent variables, and antioxidant categories and covariates as independent variables. We considered that an association was present when we found a statistically significant linear trend across quartiles or a statistically significant difference in semen parameters between any of the quartiles. For statistical analyses, SPSS® ver. 20 (IBM Corp., Armonk, NY, USA) was used and p < 0.05 was considered significant.
RESULTS
The final analysis was done on the 175 infertile men. Table 1 lists the baseline characteristics of the study patients. Mean age of study participants was 32.19 years. Also, the mean weight and body mass index (BMI) of the participants in the study were 85.28 kg and 26.80 kg/m2, respectively. The 37% of the participants were smokers, and 5% of them reported alcohol consumption. The mean daily total intake was 5235.73 ± 244.28 µg/day for β- carotene, 1,041.50 ± 92.49 µg/day for α-carotene, 2,110.68 ± 92.43 µg/day for lutein, 481.63 ± 21.33 µg/day for β-cryptoxanthine, 5,117.75 ± 247.77 µg/day for lycopene, 259.74 ± 9.93 mg/day for vitamin C, 12.99 ± 0.54 mg/day for vitamin E and 8.89 ± 0.37 mg/day for α-tocopherol. The mean volume of semen produced at participant's ejaculation was 4.65 ± 1.78 mL, and the mean sperm counts were 56.04 ×106/mL. Also, the mean sperm concentration was 12.46 ± 5.46 ×106/mL, the mean percentage of motile sperm was 29.07% ± 18.2%, and mean value for morphologically normal sperm was 1.76% ± 1.08%. Table 2 has shown the correlation between covariate mean values and some baseline parameters. We found that there was a significant inverse association between age and sperm density (r = −0.015, p = 0.04); also, we observed a linear association between sperm density and carbohydrate intake (r= 0.15, p = 0.04). There were no significant associations between sperm-related parameters with BMI, total caloric, protein, and fat intake and physical activity level (p > 0.05). Table 3 presents the multivariate crude and adjusted model of dietary intake of antioxidant nutrients and semen parameters. We found a significant inverse association between β-carotene and vitamin C intake with DFI (Ptrend = 0.042 and Ptrend = 0.03, respectively). As shown in Table 3, after adjusting for covariates men in the highest quartile of daily lutein intake had a higher sperm total count (p = 0.03) than men in the lowest quartile (Ptrend = 0.045). Also, we observed that men in the highest quartile of high β-Cryptoxanthin intake had a higher sperm density (p = 0.034) compared with men in the lowest quartile (Ptrend = 0.02). Other semen parameters did not show statistically significant differences with the dietary intake of antioxidant nutrients.
Table 1
Baseline characteristics of the study population
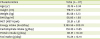
Values are expressed as mean ± standard deviation.
BMI, body mass index; MET, metabolic equivalent of task.
![]()
Table 2
Correlation between sperm quality related parameters with baseline variables

BMI, body mass index; MET, metabolic equivalent of task DFI, DNA fragmentation index.
*Statistically significant.
![]()
Table 3
Multivariate-adjusted model of dietary intake of antioxidant nutrients and semen parameters

Tests for linear trend were performed using the median value for each quartile. Multivariate model adjusted for BMI, total calorie intake, and physical activity.
DFI, DNA fragmentation index; Pa, crude p-value; Pb, adjusted p-value.
*Statistically significant.
![]()
DISCUSSION
In this cross-sectional study, dietary intake of vitamin C and β-carotene was inversely associated with DFI. Also, dietary intake of lutein and β-Cryptoxanthin was related to sperm total count and sperm density, respectively. Previous studies have suggested that the quality of sperm has declined over the last few decades. The reason for these changes is due to factors such as environmental factors, occupational stress, metal toxicity, chemicals, heat, smoking, radiation and nutritional factors. Also, obesity, which increases the severity of inflammation in the body, is one of the critical factor [171819]. Increasing the oxidative stress and producing ROS causes damage to the proteins, lipid membranes and DNA integrity of spermatozoa [2021]. Therefore, adequate dietary antioxidants intake is necessary to reduce the number of active oxygen species and for maintaining standard sperm quality and quantity [22]. Vitamin C is one of the important water-soluble vitamins that its potent antioxidant effects have been reported in previous studies [23]. Eskenazi et al. [24] showed that vitamin C has a positive effect on the quality of sperm in the older population. They reported that although the use of antioxidants was associated with improved sperm quality, but there was no clear dose relationship [24]. In the present study, vitamin C intake was inversely related to DFI. Vitamin C can increase glutathione concentration and the activity of testicular antioxidant enzymes such as catalase and superoxide dismutase that are essential for sperm survival by reducing the injuries resulting from oxidative stress [2526]. Also, vitamin C also improves the function of testicular enzymes and increases testosterone production [27]. In line with our study results, Greco et al. [28] in a clinical trial showed that taking 1 g vitamin C for 2 months improved the sperm DNA fragmentation in the infertile men. Vitamin C can act these beneficial effects during the testicular period of germ cell development by exerting a beneficial effect on germ cells, Sertoli cells, or both and leading to enhances the defense system against DNA damage [28]. In our study, similar to vitamin C, β-carotene was inversely related to DFI. Beta-carotene is the most common form of carotene in plants. Previous studies have reported that especially β-carotene acts as a powerful mitigator of oxidative stress in the absence of other antioxidants [29]. It has been shown that dietary β-carotene may have provided beneficial effect in modulation of ROS [30]. In our study, betacryptoxanthine was related to sperm density. Mínguez-Alarcón et al. [31] reported that there was a positive association between dietary intakes of cryptoxanthin and sperm-related parameters specially total motile sperm count in young university students. Also, Lorenzo et al. [32] found that cryptoxanthin plays a role in repairing DNA oxidative damage. Lutein is one of the other major carotenoids and in the present study, it was related to sperm total count. No previous studies have reported an association between cryptoxanthin and sperm total count.
We have not observed any significant association between lycopene, vitamin E, α carotene and α-tocopherol with sperm parameters. This contrasts with the results of previous studies. Mínguez-Alarcón et al. [31] found that there was a positive association between lycopene intakes and total motile sperm count. Also, Almbro et al. [33] reported that dietary intake of vitamin E significantly increased sperm competitiveness, but β-carotene did not. Finally, Moslemi et al. [34] in a clinical trial found that co-supplementation with vitamin E and selenium improved sperm quality and had protective effects on sperm in infertile men.
This study has several limitations that should be considered when interpreting our results. The design of our study was cross-sectional, and this prohibits inferring a causal link between dietary antioxidant intake and infertility. Therefore, in order to confirm the results of our study, randomized clinical trials are required. Also, we were not able to measure changes in serum levels of micronutrients, which could increase the accuracy of the results. Finally, because no perfect and accurate instrument for diet evaluation exists for our population, the reported intake may have reporting errors or biases. However, food frequency questionnaires have been previously shown to validly estimate usual intake in the Iranian adult population [11].
In conclusion, we found an inverse association between dietary consumption of some antioxidants and sperm-related parameters. Additional studies, particularly of prospective nature, are required to further investigate these associations.
 XML Download
XML Download