

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Non-alcoholic fatty liver disease (NAFLD) is a chronic disease induced by triglyceride accumulation in liver cells (more than 5% of the liver weight) in the absence of significant alcohol consumption [12]. NAFLD begins with simple steatosis and progresses to non-alcoholic steatohepatitis, and then to severe liver lesions including cirrhosis, and even hepatocellular carcinoma [3]. Moreover, NAFLD is associated with increased risk of other chronic disorders including cardiovascular diseases, diabetes and even chronic kidney disease that increase mortality and impose high financial costs to the healthcare system [456]. Due to the high incidence of NAFLD, it is important to investigate its pathogenesis and develop effective therapies for this hepatic disorder. Overweight/obesity are considered as the most important risk factors in this context [78]. In modern medicine, life style modification has been reported as the well-known strategy for managing body weight, but this strategy has achieved limited success over a long time [91011]. Therefore, demand for finding anti-obesity supplements to increase adherence these patients to aforesaid approaches has been existed. In this context, herbal agents such as Nigella [12], Cumin [13], cinnamon [14], cranberry [15], and saffron [16] have attracted most attention during the recent years, mostly due to their high popularity and high polyphenols content [1718].
Turmeric is a yellow powder that is extracted from the dried Curcumin longa L. (ginger family) [19]. It is used as a food colorant, and additive in Asian countries [20]. Turmeric has many valuable components but the one seems getting attention is curcumin [21]. Curcumin (diferuloylmethane) is a polyphenolic agent with a multitude of effects including anti-oxidant [22], anti-microbial [23], anti-inflammatory [24], anti-arthritic [25], gastro-protective [26], and neuro-protective activities [27]. Recently, researchers have reported that turmeric/curcumin can inhibit obesity by reducing the production of inflammatory compounds [2728]. The anti-obesity effects of curcumin have been investigated in some clinical trials [2930313233343536]; however, the findings are conflicting. Several trials reported the beneficial effects of turmeric/curcumin on anthropometric indices [30313235], but others did not show any significant effects [29333436].
Given the controversy in this area, we performed a meta-analysis of randomized controlled trials (RCTs) in order to evaluate the effect of turmeric/curcumin on anthropometric indices, including body weight, body mass index (BMI) and waist circumference (WC) in patients with NAFLD.
MATERIALS AND METHODS
Present review was conducted and reported in accordance with the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [37]. The protocol details of our meta-analysis were also registered with the PROSPERO website, registration number CRD42018111638.
Search strategy
The following international databases were searched for eligible studies published from their inception to January 27, 2019: PubMed, Scopus, Cochrane Library, and ISI Web of Science. The search terms used included: (‘Curcumin’ OR ‘Curcuminoid’ OR ‘Curcuma’ OR ‘Turmeric’ OR ‘Curcumin longa L.’) AND (‘Non-alcoholic fatty liver disease’ OR ‘NAFLD’ OR ‘Non-alcoholic steatohepatitis’ OR ‘NASH’ OR ‘Fatty liver disease’). We did not implement any restrictions on language and publication time. In addition, we searched trial registry websites including Iranian Registry of Clinical Trials (www.irct.ir), and ClinicalTrials.gov, to find unpublished studies. Since we did not want to miss any eligible papers, the bibliographies of all selected articles including original research papers and review papers were also scanned. The searches were performed by one of the authors (R.G.). Search terms together with the search strategy are presented as Supplementary material (Supplementary Table 1).
Study selection
After all identified studies were inserted in reference manager software (EndNote X6; Thomson Reuters, New York, NY, USA), duplicate publications were eliminated and remained articles were scanned based on title, abstract, or full text by two authors (R.G. and S.J.) separately. Finally, investigations utilizing a controlled trial design on adults with NAFLD and considering the effect of turmeric/curcumin supplementation on anthropometric indices namely body weight, BMI and WC were included in the present review. Studies with insufficient data on treatment or control groups were excluded. Protocols were also removed because no experiment was carried out. For the duplicate publications, we only included one with larger sample size. All differences on selections were settled by face-to-face discussion among reviewers.
Data extraction
Two independent investigators (R.G. and S.J.) abstracted following data from each trial and included in a table, whereas another author (A.H) was also present to resolve any controversies: study information (author's surname, study location, and publication year), characteristics of the patients (total sample size mean age, sex, and mean BMI), details of trial (design, type and dose of intervention, and follow up duration), and anthropometric measures before and after the intervention. The reviewers resolved disagreements through discussion. In cases of missing a relevant information in the papers, we contacted first authors for help.
Quality assessment of studies
The Cochrane Risk of Bias tool [38] was used by two separate investigators (R.G. and S.J.) to evaluate the methodological quality of the papers. This scale comprises of 7 criteria which are as follows: random sequence generation, allocation concealment, blinding, as well as the detection of incomplete outcome data, selective outcome reporting, and other potential sources of bias. Based on the recommendations of the Cochrane Handbook, judgment of each item was recorded as “Low,” “High,” or “Unclear” risk of bias. According to the Cochrane Risk of Bias items, the overall quality of individual study was considered as good (Low for > 2 domains), fair (Low for 2 domains), and weak (Low for < 2 domains). Any disagreement in this section was settled by a third researcher (A.M.).
Statistical analyses
Weighted mean differences (WMDs) and standard deviations (SDs) of the following outcomes, and the data of comparison between turmeric/curcumin supplementation and control were used to calculate overall effect size: 1) body weight (kg), 2) WC (cm), and 3) BMI (kg/m2). Given that selected studies were conducted in different settings, random-effect models were used for analysis [39]. When SD for mean differences was not reported, it was calculated by the following formula [40]:
SD change = square root [(SD baseline 2 + SD final 2) − (2 × R × SD baseline × SD final)]
To ensure the meta-analysis was not sensitive to the selected correlation coefficient (R = 0.5), we re-analyzed the WMDs using correlation coefficients of 0.2 and 0.8. In situations where only a standard error (SE) was reported, we calculated SD using the formula of SE×√n. Heterogeneity was examined using the I-squared (I2) index. I2 values greater than 50% were considered as significant heterogeneity [41]. In case of high heterogeneity between studies, we conducted subgroup analysis according to the type of supplement (turmeric or curcumin), trial duration (≥ 12 weeks or < 12 weeks), and baseline BMI (≥ 30 kg/m2 or < 30 kg/m2) to assess the impact of these factors on results. In the sensitivity analysis, a single study was omitted each time and the analyses were repeated to evaluate its influence on the overall effect size. Publication bias was also assessed via visual inspection of funnel plots and egger's regression asymmetry test [42]. A p value of < 0.05 was considered as statistically significant.
RESULTS
A total of 515 publications were identified through our searches and one paper was also identified by hand search. After removal of duplicates, 258 articles remained. Most of papers (n = 246) were excluded after reading title or abstracts since they were not relevant. After assessing the full text of 12 potentially related articles, 8 papers [2930313233343536] were included in our analysis. The most important reasons for exclusion were as follows: 2 studies [4344] were duplicate reports, one study was administrated turmeric/curcumin in combination with other components [45], and one study [46] was published as protocol. Figure 1 shows the details of study identification and selection process.

Study characteristics
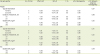
Characteristics of the 8 eligible articles are summarized in Table 1. Total of 449 participants were recruited and total sample size of each article ranged from 20 to 87. All of the studies were parallel randomized clinical trials. They were published between 2012 and 2019. One study was conducted in the Thailand [33] and the rest in the Iran [29303132343536]. Mean age of the subjects ranged between 40 and 65 years. One of the trials [35] had women participant with exclusively high enrollment rate and other trials[29303132333436] included both sexes. In two studies turmeric [2934] was administered, and in remaining 6 studies [303132333536] curcumin was administered. The dosage of the intervention varied from 80 to 100 mg/day and 2 to 3 g/day for curcumin and turmeric, respectively. The trial durations were between 8 and 24 weeks. All studies were carried out on subjects with baseline BMI ≥25 kg/m2. One study [35] was published in Persian, and the remaining seven studies were published in English. Of the 8 included studies [2930313233343536], seven [29303132333536] were original articles and one was a thesis [34].
Table 1
Characteristics of included studies

| Author [Reference No.] | Country | Total sample size (M/F) | Mean age, yr | Mean BMI, kg/m2 | RCT design (blinding) | Duration, wk | Dose and type of intervention | Comparison group | Results |
|---|---|---|---|---|---|---|---|---|---|
| Chirapongsathorn et al. [33] | Thailand | 11M/9F | 54 | 29 | Parallel (Yes) | 24 | Curcumin (NR) | Placebo (NR) | BMI ↔ |
| WC ↔ | |||||||||
| Claradeh et al. [35] | Iran | 22F | 65 | 27 | Parallel (Yes) | 12 | Curcumin (80 mg/day) | Placebo (Dextrose) | Weight ↓ |
| BMI ↓ | |||||||||
| Panahi et al. [43] | Iran | 51M/36F | 46 | 28 | Parallel (Yes) | 8 | Curcumin (1,000 mg/day) | Placebo (NR) | BMI ↓ |
| WC ↓ | |||||||||
| Navekar et al. [29] | Iran | 18M/24F | 41 | 31 | Parallel (Yes) | 12 | Turmeric (3,000 mg/day) | Placebo (Starch) | Weight ↔ |
| BMI ↔ | |||||||||
| Rahmani et al. [31] | Iran | 38M/42F | 48 | 30 | Parallel (Yes) | 8 | Curcumin (500 mg/day) | Placebo (NR) | Weight ↓ |
| BMI ↓ | |||||||||
| Jarahzadeh and Hosain [34] | Iran | 38M/26F | 40 | 31 | Parallel (Yes) | 8 | Turmeric (2,000 mg/day) | Placebo (Starch) | Weight ↔ |
| BMI ↔ | |||||||||
| WC ↔ | |||||||||
| Jazayeri-Tehrani et al. [32] | Iran | 46M/38F | 42 | 30 | Parallel (Yes) | 12 | Curcumin (80 mg/day) | Placebo (NR) | Weight ↓ |
| BMI ↓ | |||||||||
| Saadati et al. [36] | Iran | 27M/23F | 45 | 32 | Parallel (Yes) | 12 | Curcumin (1,500 mg/day) | Placebo (Maltodexterin) | Weight ↔ |
| BMI ↔ | |||||||||
| WC ↔ |
RCT, randomized controlled trial; M, male; F, female; BMI, body mass index; NR, not reported; WC, waist circumference.
![]()
After assessing the methodological quality of eligible studies, all of trials had good scores. Although random generation methodology was reported in all trials, only 5 studies reported enough information about allocation concealment [3031323436]. Six studies reported sufficient data for method which used for blinding design [293132333436]. All studies were showed low risk of bias according to incomplete outcome data and selective outcome reporting. Summary of quality assessment on selected publications are reported in Table 2.
Table 2
Cochrane risk of bias assessment

| Study | Random sequence generation | Allocation concealment | Blinding of participants, personnel and outcome assessors | Incomplete outcome data | Selective outcome reporting | Other sources of bias |
|---|---|---|---|---|---|---|
| Chirapongsathorn et al. [33] | L | H | L | L | L | U |
| Claradeh et al. [35] | L | U | H | L | L | U |
| Panahi et al. [43] | L | L | H | L | L | U |
| Navekar et al. [29] | L | H | L | L | L | U |
| Rahmani et al. [31] | L | L | L | L | L | U |
| Jarahzadeh and Hosain [34] | L | L | L | L | L | U |
| Jazayeri-Tehrani et al. [32] | L | L | L | L | L | U |
| Saadati et al. [36] | L | L | L | L | L | U |
![]()
Effect of turmeric/curcumin supplementation on body weight
The effect of the turmeric/curcumin supplementation on body weight was reported in 7 clinical trials [29313233343536]. Overall, meta-analysis by random effect model showed that turmeric/curcumin supplementation had no significant effect on the weight (WMD, −0.54 kg; 95% confidence interval (CI), −2.40, 1.31; p = 0.56) (Figure 2). There was no evidence of heterogeneity between the effect sizes of studies (I2 = 0.0%; p = 0.99). Subgroup analysis based on trial duration, type of intervention, and basline BMI revealed that the effect was not statistically significant in all subgroups (Table 3). Sensitivity analysis showed that the exclusion of any single trial from the analysis did not alter the overall effect.
 | Figure 2Forest plot of mean difference in body weight between supplementation with turmeric/curcumin and placebo group.WMD, weighted mean difference; CI, confidence interval.
|
Table 3
Subgroup analysis to assess the effect of turmeric/curcumin supplementation on body weight, BMI, and WC of patients with NAFLD
BMI, body mass index; CI, confidence interval; WC, waist circumference; NAFLD, non-alcoholic fatty liver disease.
*Calculated by Random-effects model.
![]()
Effect of turmeric/curcumin supplementation on BMI
The meta-analysis of seven studies [29303132343536] revealed that turmeric/curcumin supplementation did not significantly affect BMI (WMD, −0.21 kg/m2; 95% CI, −0.71, 0.28; p = 0.39) (Figure 3). The effect was homogenous across the included trials (I2 = 0.0%; p = 0.97). We carried out subgroup analysis based on based on trial duration, type of intervention, and participants' baseline BMI. Results showed that the effect was not statistically significant in all subgroups (Table 3). In addition, results of sensitivity analysis showed that present estimates were not affected by a single trial.

Effect of turmeric/curcumin supplementation on WC
Four studies [30333436] reported WC as an outcome measure. Pooled effect size from random effect model showed no significant effect of turmeric/curcumin in the reduction of WC (WMD, −0.88 cm; 95% CI, −3.76, 2.00; p = 0.54). There was no significant heterogeneity across interventions (I2 = 0.0%; p = 0.97) (Figure 4). We carried out subgroup analysis based on participants' baseline BMI. Results showed that the effect was not statistically significant in all subsets (Table 3). In addition, the overall estimates were not influenced by exclusion of none of eligible studies.

Publication bias
Based on visual inspection of the funnel plot (Figure 5), neither changes in body weight, WC and BM revealed any potential publication bias. Furthermore, Egger's test did not show any evidence of publication bias (p = 0.71 for body weight), (p = 0.12 for WC) and (p = 0.52 for BMI).

DISCUSSION
In present study, we found that supplementation of turmeric/curcumin had no significant effect on body weight, BMI and WC in patients with NAFLD. In addition, the findings of the classification based on the baseline BMI, type of administration and trial duration were in line with the overall results.
Our findings were in contrast with previous meta-analysis [47] which examined the anti-obesity effects of curcumin. They reported that curcumin supplementation comparing to placebo significantly reduced anthropometric indices. In contrary to our study which include patients with NAFLD, they examined subjects with multiple different diseases (e.g., type 2 diabetes, NAFLD and metabolic syndrome). Hence our finding might be affected by metabolic status and disease background. Moreover, theier positive result might be due, in part, to the fact that they considered articles with longer duration of intervention. In most articles we included, the duration of intervention was less than 8 weeks, which is not long enough time for investigating the anti-obesity effects of turmeric/curcumin. Therefore, it seems that more trials with adequate sample size and longer duration are needed to confirm our results.
Another meta-analysis [48] also indicated that curcumin could reduce body weight in NAFLD patients significantly. Although the results of referenced meta-analysis could be of interest to the readers, the limited number of trials (n = 4) suggests that the results obtained in they meta-analysis could be biased by sample size. Our meta-analysis provides a more robust confirmation on the lack of any weight lowering effect of curcumin compared with previous meta-analysis because of including a larger number of trials.
Precise mechanisms for effects of turmeric/curcumin on anthropometric indices have not been reported, thus far. However, some possible mechanisms have been reported in this regard. Most anti-adipogenic effects of turmeric/curcumin in cells and animals were accompanied by the suppression of peroxisome proliferator-activated receptor gamma and cytosine-cytosine- adenosine adenosine-thymidine expressions [4950], the master regulators of adipogenesis. Up to date investigations has also reported that curcumin can increase energy expenditure by enhancing adenosine triphosphate (ATP) production and increasing the activity of AMP-activated protein kinase (AMPK) [515253].
Another plausible mechanism of turmeric/curcumin on obesity is related to its impacts on hormones. Previous meta-analysis reported that curcumin administration could reduce leptin, and could increase adiponectin level, thereby modulated appetite and energy homeostasis [54]. On the other hand, overproduction of adiponectin hormone by activating AMPK could increase glucose utilization and fatty acid oxidation which, in turn, would facilitate the loss of weight [5055].
Psychological stress or anxiety may enhance dietary intake in some patients [5657]. It has been reported that curcumin can reduce anxiety by increasing the levels of monoamines serotonin, norepinephrine, and dopamine in brain [58]. The anti-anxious effects of curcumin were also demonstrated in some trials [5960].
In our study several limitations should be considered. First, the number of included trials and sample size of those studies were small. Second, the results of most studies were not adjusted for confounding factors which can affect obesity outcomes like usual dietary intakes of fruits and vegetables and physical activity level. Third, all included investigations were conducted in Asian countries and the data regarding the anti-obesity effects of turmeric/curcumin in other regions are still lacking. Lastly, the follow-up duration for the most of the studies was short. There were only 2 articles with longer duration (more than 12 weeks).
CONCLUSIONS
In conclusion, we found no significant effect of turmeric/curcumin supplementation on the anthropometric indices in patients with NAFLD. These results were not altered in all categories (type of treatment, treatment duration, BMI level) of outcome measurements. Currently there is not sufficient evidence to make solid conclusions about the effects of turmeric/curcumin on obesity; so future large-scale well-designed trials must be performed to find out possible anti-obesity effect of these components in these patients.
 XML Download
XML Download