

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
An unprecedented increase in the prevalence of childhood obesity has occurred worldwide during the last few decades [12]. In South Korea, the prevalence of childhood obesity steadily increased from 11.6% to 16.5% between 2006 and 2016 [3]. To tackle these trends in childhood obesity, unhealthy eating behaviors including individual, familial and environmental risk factors are considered the key modifiable factors [4]. Dietary modification and nutritional education are essential elements of nutrition interventions [5].
Behavioral change theory-based studies [6789] have established successful nutrition intervention implementation. Social cognitive theory (SCT) [10] and transtheoretical model (TTM) [11] have been widely used as theoretical frameworks in childhood obesity. In particular, nutrition education combined with behavior change counselling was effective in childhood obesity for weight control and dietary modification [12].
Traditionally, school-based nutrition education [13] for the primary prevention of childhood obesity has been implemented. The secondary to tertiary prevention of childhood obesity requires more structured and comprehensive treatments including a healthier diet and weight [14]. Furthermore, evidence-based [15], customized nutritional intervention that considers obesity-related genetic, environmental, family, and community factors is powerful strategy for treating childhood obesity. The nutrition care process (NCP) [16] model is a well-known, systematic, problem-solving method that may allow the modification of diet-related behaviors and lifestyles in childhood obesity. None of studies have been treated and documented by using NCP according to nutrition and health status for childhood obesity.
Therefore, this study aimed to develop a theory- and evidence-based nutritional intervention to change the dietary habits of moderate to severe obese children and adolescents.
METHODS
Literature review
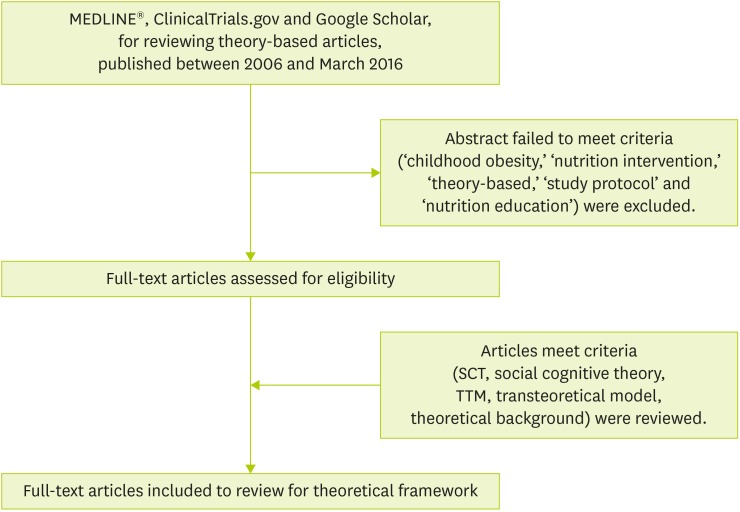
As shown in Figure 1, relevant research papers conducted in children and adolescents aged 10–18 from 2006 to 2016 were reviewed by a trained nutrition expert team. A search for theory-based scientific articles was reviewed in MEDLINE®, ClinicalTrials.gov and Google Scholar. Various terminologies were used such as ‘childhood obesity,’ ‘nutrition intervention,’ ‘theory-based,’ ‘study protocol’ and ‘nutrition education.’ Effective intervention components were reviewed and analyzed from a previous childhood-obesity intervention. We identified studies [171819202122232425262728293031323334353637] with SCT- based or TTM, to consider theoretical background, contents of nutrition education session and intervention components development.
Theoretical background
This protocol was designed to focus on a theoretical framework-employed SCT [10] and TTM [11]. SCT is widely used to design intervention programs that emphasize behavioral change strategies between personal and environmental factors [38]. SCT constructs including environments, behavioral capacity, self-control, observational learning, reinforcements, and self-efficacy have been applied in nutrition education curricula [39]. For development of this protocol, SCT was employed to address what factors affect unhealthy eating behaviors related to socio-environmental factors in moderate to severe obese children and adolescents in order to improve behavioral change to target healthy dietary habits and lifestyle modification. This conceptual framework nutritional intervention delivered based on the TTM stages of participants. TTM evaluates the stages of change in diet-related behaviors and lifestyle modification in moderate to severe obese children and adolescents.
Adoption of customized NCP model
The NCP model [16] is a well-known, systematic, problem-solving method that allows nutrition experts to care for their patients individually using a structured and standardized language. Four distinct, interrelated steps, nutrition assessment, diagnosis, intervention and monitoring/evaluation of NCP were adopted for the present study protocol. Prior to nutrition assessment of the participants, anthropometrics, biochemical data, self-reported questionnaires and 3-day food diaries were assessed. After analyzing the recorded data, diet-related problems were identified by a problem (P), etiology (E), and sign/symptom (S) form, which the NCP adopted (Academy of Nutrition and Dietetics, 2016). A nutrition diagnosis was documented by writing a PES statement after communication and collaboration with other providers and professionals. The customized nutritional intervention program comprised four monthly appointments that aim to identify barriers to healthy eating behaviors and inform the nutritional knowledge of a balanced diet in moderate to severe obese children and adolescents.
Setting and participants
Moderate to severe obese children and adolescents from ages 7 to 16 with body mass index (BMI) ≥ 95th percentile and their family were included. One hundred three participants and their families were recruited through posted flyers, newspaper advertisements, email, and social media. The sample size was calculated for our project based on changes in BMI-z score between groups. The study had 80% power with a two-sided significance level set at 0.05 to detect differences of 0.1 between usual care and physical activity (PA) groups. PA sessions were randomly assigned by senior researcher who is not blinded because of regional and individual time differences.
The questionnaire packets were sent to families who contacted the intervention team manager to join this study. The packets for participants contained a project brochure, a welcome letter, a detailed list for initial assessment, consent forms and a survey (clinical, PA and food & nutritional).
The study was conducted according to the guidelines laid down in the Declaration of Helsinki, with ethical approval from the Hallym University Sacred Heart Hospital's Institutional Review Board (approval number: 2015-I134) and all participants provided informed consent. This study was registered at cris.nih.go.kr (identifier: KCT0002111).
RESULTS
Nutritional intervention protocol and program development
Supplementary Table 1 describes the 16-week nutritional intervention protocol. For a baseline, the consent form, questionnaires for participants and parents, and 3-day food records were assessed by nutrition team. Anthropometric measurements and a biochemical assessment were performed by trained nurses. The nutritional intervention program included education and counselling, nutrition assessment, phone contact, text messages, online cooking recipes, and a compliance assessment (Supplementary Table 1).
The SCT components of nutritional intervention
The SCT components and objectives of the nutrition session are described in Table 1. All sessions aimed to provide nutritional knowledge and a practical mission in real life for individual dietary goal setting and self-control. Nutrition education (NE), skill building (SB), goal setting (GS), outcome expectation (OE), overcoming barriers (OB) and social support (SS) were applied to perform the monthly practical missions, individual goal setting to change dietary habits, and to seek environmental barriers in moderate to severe obese children and adolescents (Table 1).
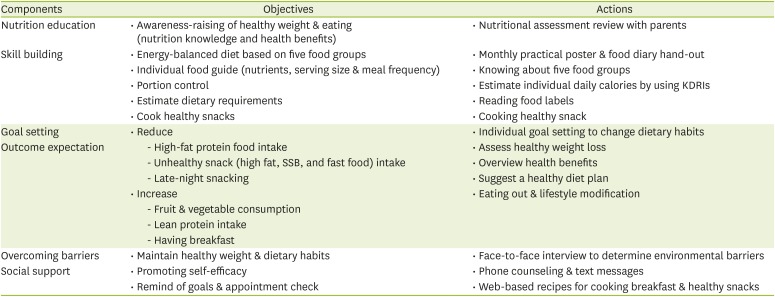
Table 1
An overview of SCT components and objectives
SCT, social cognitive theory; KDRIs, Dietary Reference Intakes for Korean; SSB, sugar-sweetened beverage.
![]()
Customized nutrition care process
Dietary, clinical assessment components and tools
An evidence-based nutritional intervention protocol was developed to adopt the NCP model to care for and manage childhood obesity. To assess the nutritional status of the participants, dietary habits, nutritional intake, medication and supplement history, life and social history, medical/health history, anthropometrics and biochemical markers were used by a nutrition expert. In this step, nutrition-related metabolic risk factors, dietary problems, nutritional knowledge, stages of change and the nutritional status based on an individual Dietary Reference Intake (DRI) were evaluated (Table 2).
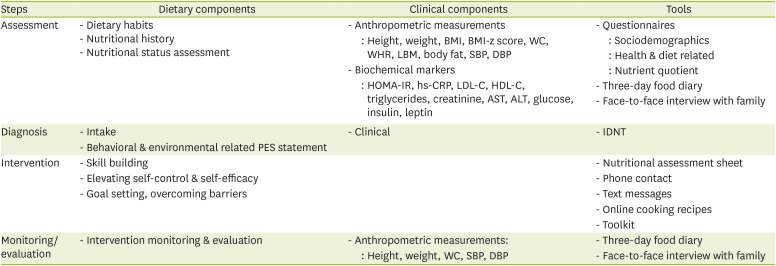
Table 2
Dietary and clinical components and tools of the NCP
NCP, nutrition care process; BMI, body mass index; WC, waist circumference; WHR, waist-hip ratio; LBM, lean body mass; SBP, systolic blood pulse; DBP, diastolic blood pulse; HOMA-IR, homeostatic model assessment-insulin resistance; hs-CRP, high-sensitivity C-reactive protein; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; AST, aspartate aminotransferase; ALT, alanine aminotransferase; IDNT, International Dietetics and Nutrition Terminology.
![]()
Dietary problems and employed nutrition diagnosis
A specific nutrition problem was identified by a PES statement from the nutrition assessment data for nutrition diagnosis. In this critical step, a nutrition problem was described by using standardized nutrition diagnosis language such as “inadequate energy intake,” “overweight/obesity,” and “food and nutrition-related knowledge deficit.” A nutrition expert team analyzed the terminology to label the nutritional diagnosis by using three main domains for treatment: intake, clinical and behavioral. Each selected International Dietetics and Nutrition Terminology (IDNT, 2015) were labeled for the three domains from the initial screening of the participants' dietary problems (data not shown).
Nutrition intervention and monitoring & evaluation
All consenting participants underwent 30 minutes of individual nutrition education and counselling throughout the 16-week intervention. A face-to-face diet-related interview was performed by a nutrition expert to find the barriers to healthy eating habits of the participants and their families for customized nutritional education and counselling. In every counselling session, a nutrition assessment sheet was provided based on the 3-day food diary of the participants. From the assessment sheet completed by a nutrition expert, each participant reviewed their problematic eating behaviors such as excessive fat intake or frequent sugar-sweetened beverage (SSB) consumption. During each session, theme-based nutrition education was taught to the participants. Monthly goal setting was discussed with the participants and their families at the end of each individual counselling session. Monthly phone contact and text messages were provided for the social support along with online food recipes to emphasize consuming vegetables and fruit and having the breakfast (Table 3).
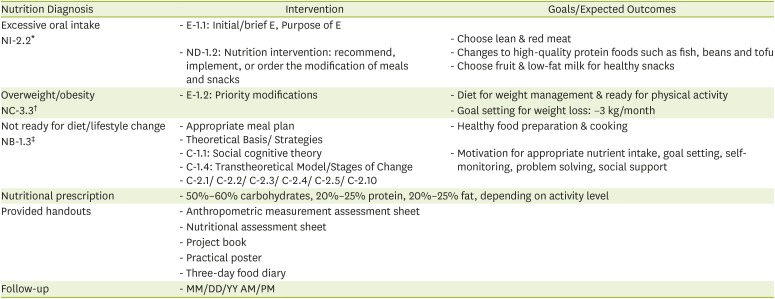
Table 3
Nutrition intervention components by using IDNT
IDNT, International Dietetics and Nutrition Terminology; NI, nutrition intake; NC, nutrition clinical; NB, nutrition behavioral; E, nutrition education; ND, nutrient delivery; C, nutrition counseling.
*Defined as “actual problems related to intake of energy, nutrients, fluids, bioactive substances through oral diet or nutrition support”; †Defined as “nutritional findings/problems related to medical or physical conditions”; ‡Defined as “nutritional findings/problems that related to knowledge, attitudes/beliefs, physical environment, access to food, or food safety”.
![]()
Monitoring and evaluation were overlapped to evaluate nutrition care outcomes (behavioral, physical, and environmental), food intake and individual goal achievements. Nutritional adherence was evaluated that TTM compliance with the intervention program (completed all nutrition and counseling sessions) by a nutrition professional using four nutritional diagnosis categories: intake (NI) problem, clinical (NC) problem, or behavioral (NB) problem, and TTM.
Five components of the nutrition education session
Five components of nutrition education were designed by a nutrition expert team; these aimed to promote healthy dietary habits by reducing unhealthy eating behaviors and a sedentary lifestyle. The first session, ‘My meal planning,’ aimed to assess children's problematic meal patterns through the food bicycle and five food groups. In the second session, ‘My meal portion,’ an individual DRI was calculated to control personal portions by using Dietary Reference Intakes for Korean [40]. For the third session, food labels were used to ‘Choose healthy (good vs. bad) snacks.’ The fourth session was ‘Cook with fruits and vegetables’ to practice healthy cooking and increase fruit and vegetable (F&V) intake for participants. The follow-up session was to ‘Maintain a healthy diet and weight’ and consisted of a certificate to cheer on and reward the participants (Table 4). As monthly content, customized dietary goal setting was attained by every participant with their family.

Table 4
The contents of nutrition education book and practice posters
*Handout: nutritional education materials for participants; †Tools: nutritional education theme-based tools for each session.
![]()
Development of the nutritional intervention program toolkit
All content in the nutritional intervention toolkit was developed by a nutrition expert team. Based on the study protocol, an educational toolkit was provided to the participants at the first nutrition education and counselling session (Visit 1). The program book and posters were able to be displayed at home where families who participate in the nutritional intervention program could support and help each other. The contents of each page consisted of the monthly title, a poster with an illustrated guideline for a practical mission, and a goal-setting space. Three different mission posters were handed out at the baseline, and fourth and eighth weeks of the nutrition session. After tracking each monthly poster, the participants and their families were encouraged to upload the completed posters on the community website.
The logotype was designed to consider community movement and cooperation to overcome stigmatization for participants and their families. Resources for promoting healthy eating practices including a program book, practice posters, food diaries and a water bottle were provided to all participants to motivate their healthy eating and lifestyle.
DISCUSSION
To intervene systemically, strengthened evidence and continuous care were required in the secondary and tertiary prevention of childhood obesity in a community setting. Little is known about studies that have been adopted to customize the nutrition care process (NCP) model in childhood obesity. This is the first study to develop a nutritional intervention protocol for South Korean children and adolescents with moderate to severe obesity. The present theoretical framework and customized NCP approach protocol were designed with integrated strategies for participants and their families to evaluate unhealthy dietary behaviors and lifestyles. In addition, five healthy diet-related education programs with the social cognitive theory (SCT) components were developed to treat childhood obesity. An educational toolkit for a nutrition program was designed to cheer on and support the participants.
A theoretical framework has been carried out in several previous studies [6789]. SCT offered a theoretical underpinning for the behavior changes in previous childhood obesity nutritional interventions [6]. Improved culinary skills increased the consumption of fruits and vegetable (F& V), which affected participants' long-term health [41]. Furthermore, applied nutrition education (e.g., fruit-flavored water) supported the behavioral changes in participants' diets. An ongoing cohort study [7] provided nutrition education sessions for participants, which encouraged more healthful foods instead of sugar-sweetened beverage (SSB), processed foods and fast foods. In addition, a round-table session for their families was helpful to build strategies for overcoming barriers. Familial involving intervention enhanced emotional and psychosocial health improvements in obese Latino youth with prediabetes [8] by fostering social support components [4243]. These elements could assist with building self-efficacy in this critical age as a ‘gold-standard’ for sustainable health-related behavioral change [44]. A systematic review reported positive dietary outcomes (reduced fat intake or increased F&V consumption) and significant changes in stage actions and maintenance from the previous transtheoretical model (TTM)-based interventions [9]. In the present study, the constructs of SCT were applied to the nutritional intervention protocol development. This protocol aimed to increase awareness of healthy eating behaviors, customize food guidance (nutrients, serving size, and snack & meal frequency), reduce unhealthy snacking and maintain healthy dietary habits in moderate to severe obese children and adolescents. During the intervention, the SCT components (nutrition education [NE], skill building [SB], goal setting [GS], outcome expectation [OE], overcoming barriers [OB] and social support [SS]) of the program helped set individual goals for changing the dietary habits, and building the skills (portion control, nutrition label reading and cooking healthy snacks) of participants with their families. Furthermore, TTM-based customized face-to-face nutrition counselling, phone contact with families, and text messages were implemented to continuously support participants.
Problematic eating behaviors were prevalent in obesity-related dietary patterns in numerous previous studies. It also has been reported from several studies that high quantities of fat, sugar, and calories can lead to various obesity-related health problems. In particular, dietary patterns such as eating out and consuming fast food, SSB, portion size and energy-dense foods, F&V intake, skipping breakfast, and unhealthy snacking habit [45] were important key eating behaviors for obtaining a qualitative dietary assessment of childhood obesity. Data from the 2017 Korean Youth Risk Behavior survey indicates a lower intake of fruit and milk vs. a higher consumption of fast food and SSB in Korean youth [46]. Consistent with these reports, this study protocol was designed to identify obesity-related dietary behaviors and modify the key factors of diet and lifestyle through a customized NCP in moderate to severe obese children and adolescents. At the beginning of the intervention, assessed individual dietary problems of the participants were labeled with selected International Dietetics and Nutrition Terminology in this study. All participants were individually counseled to overcome diet-related problems and barriers based on their nutritional status and readiness. Over 16 weeks, a nutrition expert taught all participants monthly theme-based nutrition education and developed nutritional knowledge and skills (e.g., portion control and reading food labels) to adapt to their real life.
The Childhood Obesity Research Demonstration project [34] in the U.S. is a well-established real-world implementation of evidence-based intervention among numerous childhood obesity studies. The project teams built in each community aimed to improve healthy weight and growth among children by increasing the obesity-related nutritional and physical knowledge and skills of the parents, providers, teachers and organizations. The Identification and prevention of Dietary- and lifestyle-induced health EFfects In Children and infants (IDEFICS) [35] study is a community-oriented intervention that aims to prevent childhood obesity in eight European countries. From the baseline survey (n = 11,674), high levels of sedentary behavior, low F&V and SSB consumption and low PA were presented as obesogenic factors. Even the week effects were reported over the 2-year follow-up [36], however, lower consuming sugar were observed after six years further follow-up from the families and children who participated in the intervention when compared with the control group [37].
The present nutrition education content and program toolkit were consistently designed to target all family members, so that siblings and peers could join the participants in focusing on healthy eating and F&V consumption not only during the intervention also maintaining healthy habits in diet and lifestyle after the intervention. Such advantageous properties of the education content and program toolkit might be useful in the childhood obesity weight management field to overcome stigmatization and build social support. It can also be generalized and scaled to other populations and communities for easy access. Another strong point of the present study is a theory-based framework that adopts an evidence-based NCP approach in childhood obesity. With this approach, it might be possible to find obesity-related behavioral and environmental factors surrounding moderate to severe obese children and adolescents. Additional strengths of the study include the educational resources and individual nutrition sessions. These methods help with engagement and support to build a ‘rapport’ between participants and their families with nutritional experts as mediators during the intervention. Additionally, the participants' use of a unique toolkit for individual strategies and goal setting that is based on the constructs of the SCT could interplay a role for participation.
Nevertheless, some limitations exist due to the lack of previous research for guiding the study protocol focused on this population. Therefore, the latest published formative research and childhood obesity guideline 28 were reviewed to develop the present study protocol. Secondly, a customized NCP requires sufficient time to accurately assess each participant. Therefore, a more systematic procedure (e.g., electronic or internet-based) and well-trained nutrition staff would be needed to utilize this protocol in a real setting.
A theory-based framework and evidence-based NCP study protocol were developed in the present study. In the study protocol, the obesity-related, modifiable risk factors of the participants were treated through diet and eating behaviors during the intervention. A unique project toolkit and nutrition sessions were used to improve the eating behaviors of moderate to severe obese children and adolescents by changing their unhealthy dietary habits. This nutritional intervention protocol and program might assist with implementing and disseminating further research in childhood obesity.
 XML Download
XML Download