

 PDF
PDF Citation
Citation Print
Print


CLINICAL MANIFESTATIONS OF SEVERE CUTANEOUS ADVERSE DRUG REACTIONS
Adverse drug reactions (ADRs) are estimated to cause approximately 3%–6% of all hospital admissions, occur in 10%–15% of patients and have a fatality rate of 0.32% in hospitalized patients [123]. Rawlins and Thompson [4], classified ADRs into 2 types, A and B. Type A, the predictable reactions, account for more than 80% of ADRs and relate to overdosage and the pharmacological activities of given drugs. The unpredictable reactions, type B, are responsible for fewer than 20% of ADRs and comprise both immune-mediated and non–immune-mediated reactions. Immune-mediated reactions have been classified by Gell and Coombs into 4 main subtypes of reactions (Fig. 1) [5]. Of these subtypes, IgE-mediated and delayed hypersensitivities are the most common.
Fig. 1
Classification of adverse drug reactions. NSAID, nonsteroidal anti-inflammatory drug; SJS/TEN, Stevens-Johnson syndrome/toxic epidermal necrolysis; HSS/DRESS, hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms; AGEP, acute, generalised, exanthematous pustulosis.

Approximately one-fifth of all drug-induced ADRs are cutaneous adverse reactions and affect 2%–3% of hospitalized patients [6]. Severe cutaneous adverse reactions (SCARs), a form of T-cell-mediated hypersensitivity, account for approximately 2% of drug-induced cutaneous adverse reactions. The clinical spectrum of SCARs comprises Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), drug rash with eosinophilia and systemic symptoms (DRESS) (also known as drug hypersensitivity syndrome [HSS] or drug-induced hypersensitivity syndrome [DIHS]), and acute generalised exanthematous pustulosis (AGEP) [7]. Clinical and laboratory manifestations of severe cutaneous adverse drug reactions are summarised in Table 1 and the classification of adverse drug reactions is depicted in Fig. 1.
Table 1
Clinical and laboratory manifestations of severe cutaneous adverse drug reactions

| Clinical phenotypes | Leading culprit medications | Index-day | Early symptoms | Skin lesions | Mucous membranes | Systemic symptoms |
|---|---|---|---|---|---|---|
| SJS/TEN [7936] | -Anticonvulsants (CBZ) | Within 4 weeks, shorter if re-exposure occurs | -Fever>38°C | -SJS: skin detachment<10% BSA | -Involvement of more than 2 mucous membranes in 80%–90% of SJS/TEN cases | -Liver: transiently elevated transaminases |
| -Allopurinol | -Discomfort of throat, eyes | -TEN: skin detachment>30% | -Ocular | -Kidney impairment (mostly due to fluid loss) | ||
| -Antibiotics | -Skin rashes | -Overlap SJS/TEN: 10%–30% | -Nasopharyngeal, oropharyngeal | -Leukopenia | ||
| -NSAIDs | -Atypical target lesions (raised or flat) | -Genital | ||||
| -Nikolsky's sign present in TEN (cause: necrolysis of epidermis) | -Anal | |||||
| -Haemorrhagic lesions on lips | ||||||
| HSS/DRESS [947] | -Anticonvulsants | Within 6 weeks | -Fever>38°C | -Maculopapular/morbilliform rashes | -Very rare, only in overlap clinical phenotypes SJS/DRESS | -Liver: elevated transaminases |
| -Allopurinol | -Skin rashes (flu-like syndrome) | -Exfoliative dermatitis | -Kidney insufficiency | |||
| -Dapsone | -Desquamation | -Eosinophilic pneumonitis, meningitis, myocarditis, pancreatitis | ||||
| -NSAIDs | -Facial oedema | -Lymphadenopathy: palpable lymph nodes (>1 cm and at least 2 sites) | ||||
| -Haematological abnormalities: atypical leukocytes, eosinophilia (>1,500 cells/µL) | ||||||
| -Evidence of viral infection or reactivation: HHV 6, EBV, parvovirus B19 reactivation | ||||||
| AGEP [949] | -Antibiotics | Within 48 hours to less 2 weeks | -Fever>38°C | -Exanthema | -Very rare, in severe cases | -Hyperleukocytosis |
| -NSAIDs | -Pustules | -Neutrophils≥7,000/µL | ||||
| -Anticonvulsants | -Mild eosinophilia |
SJS/TEN, Stevens–Johnson syndrome/toxic epidermal necrolysis; CBZ, carbamazepine; NSAID, nonsteroidal anti-inflammatory drug; BSA, body surface area; HSS/DRESS, hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms; HHV, human herpes virus; EBV, Epstein-Barr virus; AGEP, acute, generalised, exanthematous pustulosis.
Despite their being uncommon, SCARs, especially SJS/TEN and HSS/DRESS, result in a very great burden of disease. These reactions not only carry with them a high mortality (10%–50%) and high morbidity (60%) with severe ocular complications, alopecia and oral and dental complications [8], but also create a substantial economic burden for patients' families and society [9]. The fatalities typically occur in otherwise healthy individuals. Moreover, a minority of these patients may develop autoimmune diseases and/or an increased risk of reactions to other medications [9].
Risk factors for drug-induced SCARs are manifold and related to both the drugs and the drug users [10] (Fig. 2). Genetic risk factors are, however, the most important, remarkably so in carbamazepine (CBZ), abacavir (ABC), and allopurinol-induced SCARs.

Stevens-Johnson syndrome/toxic epidermal necrolysis
The incidence of SJS and TEN is estimated to be approximately 1 to 6 cases and less than 2 cases in every 1 million people per year, respectively [111213], depending upon the use of certain drugs and the presence of infectious conditions. Leading causative medications for SJS/TEN are antibiotics, anticonvulsants, allopurinol and nonsteroidal anti-inflammatory agents [141516]. Interestingly, in Japan, Yamane et al. [17] reported that 69% of SJS and all TEN cases are associated with CBZ, whilst allopurinol has been found to be the most common cause of SJS in Europe and Israel [18]. In the human immunodeficiency virus (HIV) cohort the incidence of SJS is 10 times higher than in the general population [19]. In addition, infectious diseases caused by Mycoplasma pneumonia and Herpes simplex have been reported as causes of SJS/TEN without the involvement of medications [2021]. In Vietnamese patients with CBZ-induced SCARs, a history of Herpes virus infection has been reported to be more frequent than it is in tolerant controls (odds ratio, 9.78; 95% confidence interval [CI], 1.17–81.43; p = 0.02) [22].
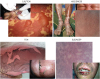
Clinical manifestations characteristic of SJS/TEN include skin detachment and mucosal erosions. The first symptoms and signs of these reactions typically occur after several days (within 4 weeks) of using the medication (index-day) [22]. The index-day occurs earlier if a patient with a history of SCAR is re-exposed to the culprit medication. The early symptoms of SJS/TEN are fever higher than 38°C, ocular discomfort and sore throat. Mucous membrane involvement then occurs and skin lesions appear and become more generalised over time [9]. The common lesions in the mucous membranes are erythema, blisters and erosions which can affect the eyes, nasopharynx, oropharynx, genitalia or anus (Fig. 3). The skin lesions in SJS/TEN manifest initially as erythema and atypical target lesions which are either macular or maculopapular. These lesions coalesce and may form very large blisters (greater than 5-cm diameter). In TEN, necrotic lesions can become generalised rapidly. The epidermal sheet detaches and sloughs under pressure (Nikolsky's sign) (Fig. 3C). SJS is distinguished from TEN by the extent of the body surface area (BSA) involved in skin detachment. SJS is defined as skin detachment of less than 10% of BSA whereas TEN is more extensive with skin detachment in 30% of BSA or greater. Skin detachment of between 10%–20% of BSA is defined as an overlapping phenotype of SJS and TEN.
Fig. 3
Clinical manifestations of different clinical phenotypes of severe cutaneous adverse drug reactions. The photos of patients with severe cutaneous adverse drug reactions who participated in the study approved by the council of science and ethics, Bach Mai Hospital (1007/QD-BM dated 1/6/2015). The informed consent forms were signed.
Internal organ involvement in SJS/TEN in the acute phase is manifest mainly as mild hepatic injury with transient elevated transaminases, kidney impairment and/or epithelial necrosis of the digestive tract and/or the respiratory tract [232425]. The reported failure of internal organs which occurs in some patients is believed to be due to infection caused by leukopenia and loss of the skin barrier and electrolyte and fluid balance disturbances due to loss of fluids and electrolytes into the extensive blisters.
The severity of the disease is measured by SCORTEN (maximum 7) (severity-of-illness score for TEN) that has been defined as seven criteria consisting of age (over 40 years), heart rate (more than 120 bpm), presence of malignant disease, skin detachment (greater than 10% of BSA), serum urea level (>10 mmol/L), bicarbonate level in arterial blood (<20 nmol/L), and blood glucose (>14 mmol/L). The higher the SCORTEN, the higher the mortality rate [26].
Long-term complications after recovery from SJS/TEN are common. Most result from adhesions of the mucous membranes and strictures in the digestive or respiratory tracts [2527282930]. Some require surgical intervention [31]. Especially common are severe ocular complications such as symblepharon, severe dry eye, trichiasis, and conjunctival invasion into the cornea, which sometimes cause visual disturbance [323334]. There is one case report of cirrhosis as a delayed complication of SJS [35].
The treatment of SJS/TEN, consists of withdrawing suspected medications and symptomatic and supportive treatment. Identification and discontinuation of the suspected medication is associated with better outcomes while delayed discontinuation or long half-lives of culprit medications increases morbidity and mortality [9]. Supportive and symptomatic care entails restoring fluid balance, providing nutrients, limiting pain, providing skin care and preventing fatal complications. In SJS/TEN, patients have an increased risk of fluid and protein leakage, leading to hypovolemia, functional renal insufficiency, and thermal dysregulation. Fluid replacement should be given as early as possible and adjusted daily [36]. High protein and high calorie nutritional therapy delivered by nasogastric tube is also recommended [936]. Patients with SCARs are at high risk of infection due to leukopenia and open wounds; however, antibiotic therapy is only indicated when infection is present [9] and antibiotics are not recommended prophylactically. Wound care and minimising skin detachment, avoiding adhesions and functional complications of mucus membranes are the targets of skin care in SJS/TEN patients. Treatment in a burns unit, with the room temperature between 30°C–32°C is recommended [36].
In parallel with supportive and symptomatic care, targeted treatments may be given (Table 2). The use of all of these treatments; corticosteroids, intravenous immunoglobulin and cyclosporine, remains controversial. The tumor necrosis factor inhibitor, etanercept, has been reported to be of benefit in encouraging skin healing without complication, presumably by reducing epithelial cell apoptosis [937].
Table 2
Targeted treatments for severe cutaneous adverse drug reactions

| Clinical phenotypes | Targeted treatments | Outcomes |
|---|---|---|
| SJS/TEN | Corticosteroid [130131132] | -As empirical treatment, IV methylprednisolone 1–2 mg/kg/day, up to 600–1,000 mg/day (pulse therapy) |
| -Related to increasing hospitalisation period and infection. Not related to mortality rate in acute phase of SJS/TEN | ||
| IVIg [36133134] | -Consensus favours therapy for SJS/TEN | |
| -No significant difference in mortality rate in comparison with corticosteroids and supportive and symptomatic care only | ||
| -No significant difference in mortality rate between high dose and low dose IVIg | ||
| Cyclosporine [135136] | -Dose 3–10 mg/kg/day, short term | |
| -Reduces mortality rate in comparison with IVIg | ||
| Anti-TNF agents (etanercept and infliximab) [37137138139] | -Benefit in healing skin lesions | |
| -Benefit in survival rate | ||
| HSS/DRESS | Corticosteroid [44140] | -Systemic corticosteroids (IV or oral) for severe HSS/DRESS |
| -Topical corticosteroids for mild to moderate HSS/DRESS | ||
| IVIg [9141142] | -Relate to complications, poorly efficacious even though IVIg has antiviral and immunomodulatory properties | |
| -Benefit in DRESS resistant to systemic corticosteroid | ||
| Antiviral drugs [47] | -No longer used because of poor efficacy and toxicity | |
| AGEP | Corticosteroid [143] | -Topical corticosteroids |
Hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms
Unlike SJS/TEN, HSS/DRESS is characterised by nonbullous skin lesions and involvement of internal organs. The incidence of HSS/DRESS ranges from 1/1,000 to 1/10,000 drug users [38]. It has a mortality rate of up to 10% [3940]. A number of medications such as allopurinol, aromatic anticonvulsants, sulphonamides, dapsone, and minocycline have been described as causes of HSS/DRESS [384142], however, allopurinol seems to be the most frequent culprit [4143].
Early symptoms of HSS/DRESS are flu-like symptoms, including fever higher than 38°C and skin rashes. Misdiagnosis is not uncommon because the index-day is frequently long, between 2–6 weeks [43]. A variety of skin lesions can be seen in HSS/DRESS such as maculopapular/morbilliform rashes, exfoliative dermatitis and desquamation [43]. Additional signs which have been reported in HSS/DRESS are facial or peripheral oedema, lymphadenopathy with palpable lymph nodes (>1 cm and >2 sites) and, rarely, mucosal involvement.
Internal organ involvement in HSS/DRESS is the result of an infiltration of eosinophils or lymphocytes in tissues [9]. The main organs affected are the liver (manifest as elevated transaminase levels) and the kidney (characteristically interstitial nephritis) [43]. Eosinophilic pneumonitis, meningitis, myocarditis, and pancreatitis have also been noted [41]. Haematological abnormalities in HSS/DRESS are eosinophilia (>1,500 cells/µL), atypical lymphocytes, leucocytosis and sometimes thrombocytopenia. In addition, the association of virus infections (human herpes virus, Epstein-Barr virus, cytomegalovirus) with HSS/DRESS has been confirmed by polymerase chain reactions, with an IgM positive or an IgG rise [41].
In HSS/DRESS treatment, as in other forms of SCARs, suspected culprit medications must be discontinued as soon as possible. Suitable skin moisturisers reduce burning and pruritus, however, unlike in SJS/TEN, targeted treatment of HSS/DRESS is important [9]. Corticosteroids have frequently been shown to be efficacious; delivered systemically when severe with organ involvement and topically in mild to moderate HSS/DRESS [9], however, premature discontinuation or rapid dosage decreases are associated with relapses. In a retrospective study of 38 cases with DRESS, topical steroid was superior to a systemic regimen in preventing relapse; however, the authors acknowledged that selection bias may have influenced the results [44]. Intravenous immunoglobulin has also been used as a therapy for HSS/DRESS because of its antiviral and immunomodulatory effects, however, its use, in general, may be complicated by severe malaise and pulmonary embolism [45]. When there is evidence for viral infection or reactivation in HSS/DRESS [46], antiviral agents such as ganciclovir and valganciclovir hydrochloride have been given [47], however, poor efficacy and toxicity have been noted.
Long-term complications commonly associated with HSS/DRESS include autoimmune diseases such as Graves' disease, Hashimoto's disease, thyroiditis and type 1 diabetes [48].
Acute generalised exanthematous pustulosis
AGEP is characterised by the rapid development of a pustular eruption, a fever higher than 38˚C and an elevated white cell count, usually occurring within 48 hours of patients commencing the culprit drug. The index-day ranges from 48 hours to less than 2 weeks [9]. Although occasionally viral infections have been involved, drugs are the cause in more than 90% of AGEP [49]. In the EuroSCAR study, the most common causative medications were antibiotics such as pristinamycin, quinolones, ampicillin/amoxicillin, whilst anticonvulsants were rarely responsible. Pre-existing infection did not increase the risk of developing the complication of infection [50]. Most AGEP are benign and spontaneous recovery occurs after 2 weeks [51]. In severe AGEP, mucous membrane and internal organs can be involved. The mortality rate of AGEP is around 2%, 5 to 10 times less than in HSS/DRESS and SJS/TEN, respectively [15].
Overlapping clinical phenotypes of SCARs
Although very rare, overlap clinical phenotypes among SCARs have been reported [752]. The clinical manifestations can overlap between SJS/TEN and AGEP, SJS/TEN and HSS/DRESS [53] and AGEP and HSS/DRESS [54]. The diagnosis of overlap is based on clinical morphology and skin biopsy findings [755] (Fig. 3).
HLA AND SEVERE CUTANEOUS ADVERSE DRUG REACTIONS
Strong associations between human leukocyte antigen (HLA) and SCARs were first discovered in ABC-induced hypersensitivity where an association with HLA-B*57:01 [5657] was found in Caucasians and then CBZ and allopurinol-induced SCARs were found to be associated respectively with HLA-B*15:02 (2004) [58] and HLA-B*58:01 (2005) [59] in Han Chinese. During the last decade, a number of HLA alleles have since been reported to confer susceptibility to drug-induced hypersensitivity, such as HLA-Cw8 in nevirapine hypersensitivity [60], HLA-B*73:01 in oxicam SCARs [61], HLA-B*59:01 with methazolamide-induced SJS [62], HLA-A*31:01 and CBZ-induced SCARs [63], and HLA-B*13:01 and dapsone hypersensitivity [6465]. Several populations in the Asia Pacific region have genetic susceptibilities for CBZ and allopurinol-induced SCARs.
Genetic susceptibility to CBZ-induced SCARs
CBZ, an aromatic amino anticonvulsant, employed since 1965 for multiple indications such as epilepsy, mental disorders and neurologically-based conditions, has been the most frequently prescribed anticonvulsant world-wide for both adults and children [6667]. The incidence of CBZ hypersensitivity is around 5%–10% with a wide clinical spectrum and it accounts for 4.1%–5.9% of SJS/TEN [68]. The incidence of CBZ-induced SCARs in Asians is approximately ten times higher than that in Caucasians [6869] and whilst non-genetic risk factors exist (age, sex, and comorbidities), a crucial role is played by pharmacogenetic risk factors.
HLA-B*15:02
Genetic susceptibility to CBZ-induced SCARs has been described in a number of populations (Table 3). The most striking genetic association was detected in a cohort of Han Chinese in Taiwan where HLA-B*1502 was found in 100% of 44 patients with CBZ-induced SJS/TEN (OR, 2504; 95% CI, 126–49,552) [58]. These findings were replicated in an extended cohort of subjects of Chinese descent originating from separate geographic areas of China [70717273], Taiwan [74], and Hong Kong [75]. In addition, HLA-B*15:02 has also been reported as a genetic susceptibility factor in CBZ-induced SJS/TEN in Thailand [76], Malaysia [77], Singapore [78], Vietnam [2279], and India [80]. Although the association between the HLA-B*15:02 allele and CBZ-induced SJS/TEN is very strong in almost all Asians, this was not found to be so in Europeans [6381], Japanese [82], and Koreans [83], which is likely due to the variable distribution of HLA-B*15:02 in different populations (prevalence very high in China, Southeast Asia, and India and very low in Europe, Japan, and Korea) [84].
Table 3
Pharmacogenetic risk factors in carbamazepine hypersensitivity

| Allele/variant | Population | Phenotype | OR (95% CI) | p value | References |
|---|---|---|---|---|---|
| HLA-B*15:02 | Taiwan | SJS/TEN | 2,504 (126–49,552) | pc = 3.1310−27 | [58] |
| Taiwan | SJS/TEN | 1,357 (193.4–8,838.3) | pc = 1.6 × 10−41 | [74] | |
| HSS/MPE | 0.77 (0.1–5.1) | p > 0.05 | [74] | ||
| China | SJS/TEN | 184 (33.2–1,021.0) | N/A | [70] | |
| China | SJS/TEN | N/A | p < 0.001 | [71] | |
| MPE | N/A | p = 0.110 | |||
| China | SJS/TEN | N/A | p < 0.01 | [72] | |
| Thailand | SJS/TEN | 75.4 (13.0–718.9) | p < 0.001 | [144] | |
| Thailand | SJS/TEN | 54.76 (14.62–205.13) | p = 2.89 × 10−12 | [76] | |
| Thailand | SJS/TEN | 25.5 (2.68–242.61) | p = 0.0005 | [75] | |
| Vietnam | SJS/TEN | 33.78 (7.55–151.03) | p < 0.0001 | [22] | |
| DRESS | NS | ||||
| Malaysia | SJS/TEN | 16.15 (4.57–62.4) | p = 7.87 × 10−6 | [77] | |
| Malaysia | SJS/TEN | N/A | p = 0.0006 | [145] | |
| Korea | SJS/TEN/HSS | N/A | NS | [83] | |
| UK | SCARs | N/A | NS | [81] | |
| North America | SJS | 38.6 (2.68–2,239.5) | p = 0.002 | [86] | |
| HSS/MPE | N/A | p = 1.000 | |||
| HLA-A*31:01 | Taiwan | HSS/DRESS | 12.17 (3.6–41.2) | p = 0.0021 | [74] |
| Japan | SJS/TEN/DIHS | 10.8 (5.9–19.6) | p = 3.64 × 10−15 | [82] | |
| Korea | HSS | 8.8 (2.5–30.7) | p = 0.001 | [83] | |
| Europe | HSS/SJS/TEN/MPE | 9.12 (4.03–20.65) | NS | [63] | |
| North America | HSS | 26.36 (2.53–307.89) | p = 0.0025 | [86] | |
| North America | MPE | 8.57 (1.67–57.50) | p = 0.0037 | ||
| HLA-B*15:11 | Japan | SJS/TEN | 16.2 (4.76–55.6) | p = 0.0004 | [88] |
| Korea | SJS/TEN | 18.0 (2.3–141.2) | p = 0.011 | [83] | |
| China | SJS | 30.77 (1.63–580.87) | p = 0.003 | [90] | |
| Asians | SJS/TEN | 0.27 (0.11–0.64) | p = 2.7 × 10−3 | [87] | |
| HLA-B*24:02 | China | SJS | 2.33 (1.16–4.69) | 0.015 | [90] |
| TNF2 allele (rs1800629) | Caucasians in Europe | Serious hypersensitivity | 2.4 (1.2–4.8) | p = 0.01 | [91] |
| rs3130690 | Taiwan | SJS/TEN | 45.65 (23.34–89.13) | pc = 1.29 × 10−39 | [74] |
| rs2848716 | Taiwan | SJS/TEN | 6.86 (4.29–10.96) | pc = 2.10 × 10−14 | [74] |
| rs750332 | Taiwan | SJS/TEN | 6.46 (3.94–10.44) | pc = 8.45 × 10−12 | [74] |
| rs2894342 | Taiwan | HSS | 7.11 (3.07–16.51) | pc = 0.0064 | [74] |
OR, odds ratio; CI, confidence interval; HLA, human leukocyte antigen; SJS/TEN, Stevens-Johnson syndrome/toxic epidermal necrolysis; HSS/MPE, hypersensitivity syndrome/maculopapular exanthems; DRESS, drug reaction with eosinophilia and systemic symptoms; SCAR, severe cutaneous adverse drug reaction; DIHS, drug-induced hypersensitivity syndrome; N/A, not applicable; NS, nonsignificant; pc, corrected p value; TNF, tumor necrosis factor.
HLA-A*31:01
The association between HLA-A*31:01 and all phenotypes of CBZ-induced SCARs has been confirmed in Caucasians [63] and Japanese [82] who have a high allele frequency (up to 0.084 in Japanese) [84]. In a Japanese study, Ozeki et al. [82] observed HLA-A*31:01 was present in 37 of 61 patients with SCARs, significantly higher than in the general population (OR, 10.8; 95% CI, 5.9–19.6). Similarly, McCormack et al. found in Europeans that HLA-A*31:01 was associated with all types of CBZ-induced SCARs in SJS (OR, 25.93; 95% CI, 4.93–116.18) and HSS (OR, 12.41; 95% CI, 1.27–121.03) [85]. In contrast, studies in Canada [86], Korea [83] and Taiwan [74], have confirmed HLA-A*31:01 is a genetic risk factor for only non-bullous skin reactions such as HSS and MPE, and not for SJS/TEN [69]. Genin's meta-analysis in different ethnic groups concluded HLA-A*31:01 is a strong genetic susceptibility gene for DRESS (pooled OR, 13.2; 95% CI, 8.4–20.8) and only very weakly associated with CBZ-induced SJS/TEN (pooled OR, 3.94; 95% CI, 1.4–11.5) [69].
HLA-B* 15:11
An association between HLA-B*15:11, a member of the HLA-B75 serotype with HLA-B*15:02, and CBZ-induced SCARs, albeit weak, has also been demonstrated in Asian populations. This risk allele can be responsible for bullous cutaneous adverse reactions [87]. In 14 Japanese (28.6%) with typical or atypical SJS/TEN, Kaniwa et al. [88] determined 4 with SJS/TEN (28.6%) were positive for HLA-B*15:11 compared with 1% of controls and none of the patients possessed HLA-B*15:02. They concluded HLA-B*15:11 is also a genetic risk factor for CBZ hypersensitivity. In Korea, HLA-B*15:11 was found to be present in 43% (3 of 7) SJS/TEN Korean patients in comparison with 4% of controls [88]. Due to their small sample size, no statistically significant difference was observed. In comparison with healthy Korean controls, the presence of this allele was significantly higher (OR, 18.4; 95% CI, 3.8–88.0; p < 0.05] [83]. Sun et al. [73] found 1 of 11 Chinese CBZ-induced SJS/TEN patients negative for HLA-B*15:02, who possessed HLA-B15:11. In Vietnamese patients, HLA-B*15:11 was not observed to be associated with CBZ-induced SCARs [22]. Despite the controversial and weak nature of this possible association, Amstutz et al. [89] recommended this possible association be further tested in larger studies because this allele was absent in 8 European patients and only present in 1 of 42 Thai patients with CBZ-induced SJS/TEN [83]. In a systematic review, examining pooled results from 20 studies, Grover and Kukreti [87]. compared the prevalence of HLA-B*15:11 in 720 CBZ-induced SJS/TEN with that in 1,113 CBZ-tolerant controls. This revealed that HLA-B*15:11 appears to be a genetic risk factor for CBZ-induced SCARs in Asians (OR, 17.43; 95% CI, 3.12–97.40; p = 1.1×10(-3)). In line with this finding, in 2017, Shi et al. [90] reported HLA-B*15:11 is strongly associated with CBZ-induced SJS in Chinese (OR, 30.77; 95% CI, 1.63–580.87, p = 0.003).
Other genetic variants associated with CBZ-induced SCARs
In 2001, Pirmohamed et al. [91] reported a polymorphism in the tumor necrosis factor (TNF)-α gene promoter region related to CBZ-induced serious hypersensitivity in Caucasians (OR, 2.4; 95% CI, 1.2–4.8), which was not observed, however, in the Genome-Wide Association Study conducted by Hung et al. in Taiwanese [74].
Variants protective against CBZ-induced SCARs
HLA-B*40:01 reportedly protects Han Chinese from bullous CBZ- induced SCARs [8792] and Alfirevic et al. [93], in 2006, reported three “heat-shock protein cluster” (HSP 70) genes (Chromosome 6, MHC class III), as being protective against serious CBZ hypersensitivity reactions. Their findings did not allow them to conclude whether this gene group is responsible or whether it reflects linkage with other polymorphisms or genes. Recently, Nguyen et al. [22] found in Vietnamese patients that HLA-B*46:01 was present more frequently in CBZ tolerant individuals versus CBZ-induced SJS/TEN/DRESS patients (OR, 0.27; 95% CI, 0.08–0.94). They noted, however, that HLA-B*46:01 is the second most frequent allele in the Vietnamese population and postulated that this observation resulted from the prevalence of HLA-B*15:02 in the patient group engendering an unequal presence of HLA-B*46:01 allele in the 2 groups.
HLA-A*24:02 appears to be a controversial genetic factor. In 2014, in their review, of patients classified by clinical phenotype, Grover and Kukreti. [87] found that the allele HLA-A*24:02 is a protective variant for SJS/TEN in Asians (OR, 0.27; 95% CI, 0.11–0.64; p = 2.7 × 10(-3)). In 2017, HLA-A*24:02, however, was reported to be a risk factor for CBZ-induced SJS in Chinese albeit with a weak association (OR, 2.33; 95% CI, 1.16–4.69; p = 0.015) [90].
Genetic susceptibility to allopurinol-induced SCARs
Since the 1960s, allopurinol, a xanthine oxidase inhibitor, has been used as first-line therapy for gout, hyperuricaemia related to cell-lysing therapy in malignant diseases and kidney stones associated with hyperuricosuria.
HLA-B*58:01
Allopurinol-induced SCARs, have also been found to result from a major genetic susceptibility factor-HLA-B*58:01 (Table 4). In 2005, Hung et al. [59] demonstrated a strong association between HLA-B*58:01 and allopurinol-induced SCARs in Han Chinese in Taiwan, with HLA-B*58:01 present in all 51 patients with SCARs (21 TEN, 30 DIHS patients) while it was identified in only 21 of 135 allopurinol tolerant controls (OR, 580.3; 95% CI, 34.4–9780.9). Their findings have been reproduced in other Asian populations; Thai [94], Korean [95] and Japanese [96], and a meta-analysis of 6 Asian studies, by Somkrua et al. [97] reported a high pooled odds ratio of 96.60 (95% CI: 24.49–381.00). This strong association has also been reported across European populations [619899].
Table 4
Pharmacogenetic risk factors for allopurinol hypersensitivity

| Allele | Population | Phenotype | OR (95% CI) | p value | References |
|---|---|---|---|---|---|
| HLA-B*58:01 | Taiwan | HSS/SJS/TEN | 580.3 (34.4–9780.9) | p = 8.1 × 10−18 | [59] |
| Thailand | SJS/TEN | 348.3 (19.2–6336.9) | p = 1.61 × 10−13 | [94] | |
| South Korea | SJS/TEN/DRESS | 97.8 (18.3–521.5) | pc = 2.45 × 10−11 | [95] | |
| Hong Kong | SJS/TEN/HSS | 123.5 (12.8–1,195.1) | p < 1 × 10−4 | [146] | |
| Japan | SJS/TEN/HSS | 62.8 (21.2–185.8) | p = 2.44 × 10−8 | [96] | |
| Europe | SJS/TEN/HSS | 80 (34–187) | p < 10−6 | [61] | |
| Portugal | All SCARs | 39.11 (4.49–340.51) | N/A | [98] | |
| DRESS | 37.71 (4.13–343.87) | N/A | |||
| SJS/TEN | 44.00 (3.18–608.19) | N/A | |||
| HLA-A*33:03 | South Korea | SJS/TEN/DRESS | 20.5 (5.4–78.6) | pc = 3.31 × 10−6 | [95] |
| Italy | SCARs | 10.155 to infinity | pc = 0.0011 | [99] | |
| Japan | SJS/TEN | 3.32 (1.46–7.54) | p = 0.0077 | [96] | |
| HLA-Cw*03:02 | South Korea | SJS/TEN/DRESS | 82.1 (15.8–426.5) | pc = 9.39 × 10−11 | [95] |
| Italy | SCARs | 10.155 to infinity | pc = 0.00105 | [99] |
OR, odds ratio; CI, confidence interval; HLA, human leukocyte antigen; HSS/SJS/TEN, hypersensitivity syndrome/Stevens-Johnson syndrome/toxic epidermal necrolysis; DRESS, drug reaction with eosinophilia and systemic symptoms; SCAR, severe cutaneous adverse drug reaction; MPE, maculopapular exanthems; N/A, not applicable; NS, notsignificant; pc, corrected p value.
Unlike with HLA-B*15:02, where the allele is only associated with CBZ-induced SJS/TEN in Asians and not HSS/DRESS, HLA-B*58:01 appears to be the common genetic risk factor for allopurinol-induced SCARs worldwide, probably due to the distribution of HLA-B*58:01 being comparable in Asians and Europeans. However, why this risk allele is not phenotype specific remains unknown.
HLA-A*33:03 and HLA-Cw*03:02
HLA class I alleles, other than HLA-B*58:01, have been reported as being associated with allopurinol-induced SCARs; HLA-A*33:03 in the Korean, Japanese [96] and Italian populations and HLA-Cw*03:02 in the Korean [95] and Italian populations [99] (Table 4). HLA-B*58:01, however, appears to be the most important genetic risk factor because it best predicts allopurinol-induced SCARs [95].
CURRENT UNDERSTANDING OF PATHO-MECHANISMS IN HLA-ASSOCIATED CBZ AND ALLOPURINOL-INDUCED SCARS
HLAs and TCRs
Principally, HLA molecules contribute to drug hypersensitivity reactions in the antigen presenting phase of T-cell-mediated immune responses. The susceptibility HLA proteins can present specific medication or a metabolic product of that medication to naïve CD8 T cells by Hapten/Pro-hapten, pharmacological interaction (P-I) or Altered peptide repertoire models (Fig. 4). Once these antigens are recognized by specific T-cell receptors (TCR), the effector phase of the immune response will occur, resulting in the proliferation of CD8 T cells and the release of cytokines [9100101]. Both CBZ and allopurinol and their metabolites are presented to T cells by antigen presenting cells (APC) without a requirement for intracellular antigen processing [102], consistent with the P-I model [103].
Fig. 4
Patho-mechanism of T-cell-mediated reactions and co-stimulators. A shows the Hapten and Pro-hapten hypothesis. In this model, the drug (Piperacillin) is processed intracellularly and presented on the surface of APCs in the complex of MHC class I. Indeed, the drug binds to endogenous peptide or protein by covalent bonds. B shows the P-I model. In this model, the drugs or their metabolites (CBZ or Allopurinol) are able to bind directly to TCR by noncovalent bonds without the intracellular processing of drug. C shows the altered peptide repertoire model. In this model, the drug (abacavir) is able to bind to the MHC (peptide binding groove) and this result in alteration of the peptide repertoire. The costimulators, including viral infections or reactivations, may become involved in the patho-mechanism, accompanied by cross-talk between dendritic cells and natural killer cells [111]. Consequently, different clinical phenotypes of severe cutaneous adverse drug reactions will be formed according to the key cells and cytokines involved. SJS/TEN, Stevens-Johnson syndrome/toxic epidermal necrolysis; HSS/DRESS, hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms; AGEP, acute, generalised, exanthematous pustulosis; APC, antigen presenting cell; pDC, plasmacytoid dendritic cell; P-I, pharmacological interaction; KIRs, killer immunoglobulin-like receptors.

CBZ-induced SCARs
In CBZ-induced SJS/TEN, Wei et al. [104] proved in vitro that CBZ or its active metabolites can interact directly with HLA-B*15:02 peptide to form the complex of HLA-B*15:02 peptide/beta-2 microglobulin/CBZ and TCR that can activate CD8 T cells. The activation of CD8 T cells leads to the apoptosis of keratinocytes resulting from the degranulation of perforin and granzyme B and Fas/FasL interaction [105]. Furthermore, Chung et al. [106] compared global gene expression between cells obtained from active lesions and peripheral blood mononuclear cells (PBMCs) and found granulysin, a biomarker for cell-mediated immune responses, increased when natural killer (NK) cells and cytotoxic T cells were activated. The authors concluded that this biomarker plays a central role in the apoptosis of keratinocytes in SJS/TEN phenotypes. In summary, there are important contributions from cytokines such as granulysin, perforin, granzyme B and TNF-α in SJS/TEN through the activation of CD8 T cells, following the recognition of HLA-specific drug complexes.
However, HLA does not play a role itself. In 2011, Ko et al. [107] compared the TCR profile on CBZ-specific T cells in SJS/TEN patients carrying HLA-B*15:02 with that of CBZ tolerant patients and healthy individuals who have never been exposed to CBZ. The results showed that the TCR Vβ-11-ISGSY clonotype was present mainly in SJS/TEN patients (16/19), absent in all CBZ tolerant patients (17) and present in only 4 of 29 healthy individuals without CBZ exposure. In addition, their functional study showed that in the PBMCs of healthy individuals who possess both HLA-B*15:02 and the TCR Vβ-11-ISGSY clonotype, CBZ-specific cytotoxicity could be primed in vitro. These results, therefore, indicate that T-cell stimulation occurs in CBZ-induced SJS/TEN only when both a specific HLA allele and a specific TCR clonotype are present. This finding is able to partly explain why the majority of HLA-B*15:02 carriers can tolerate CBZ (97%) and why HLA-B*15:02 is specific for both the clinical phenotype and the patient's ethnicity.
As previously described, unlike HLA-B*15:02, HLA-A*31:01 confers genetic susceptibility for all clinical phenotypes in CBZ-induced SCARs, mainly in Japanese [82] and Caucasians [63]. A functional study conducted by Lichtenfels et al. [108] revealed that HLA-A*31:01 is able to activate restrictedly CD8 T cells obtained from patients with CBZ-induced SCARs [108]. The authors also found involvement of HLA class II (HLA-DRB1*04:04) in the activation of CBZ-specific CD4 T cells that had been observed in Caucasian patients with CBZ-induced SCARs [109]. In addition, HLA-A*31:01 and HLA-DRB1*04:04 are in linkage disequibrilium, forming a common haplotype in Caucasians [108]. Therefore, Lichtenfels et al. proposed that this common haplotype can contribute to the response of multiclonal T cells seen in Caucasian patients with CBZ-induced SCARs, differing from Asian patients in whom little expansion of the CBZ-specific CD4 T cell population was observed [107108]. In view of these findings, it appears that the presence of HLA-A*31:01 is not involved in determining the specific clinical phenotype in CBZ-induced SCARs.
Allopurinol-induced SCARs
In allopurinol-induced SCARs, Yun et al. [110] carried out an experiment using PBMCs obtained from patients and it revealed that allopurinol and its early metabolite in plasma, oxypurinol, are able to bind the HLA-B*58:01 molecule in the F pocket of the peptide binding groove, resulting in activation of specific T cells. Moreover, the authors also found that the specific T cells do not use particular TCR repertoires to recognize the complex of allopurinol/oxypurinol and HLA-B*58:01 in allopurinol-induced SCARs.
Costimulation from innate immune responses
Innate immunity has been reported as an emerging cofactor in the context of the adaptive immune response in general and T-cell-mediated drug reactions in particular [111]. It has been implicated in reducing the threshold of T-cell activation [112]. In addition, gene expression profiling demonstrated a temporarily high level of gene transcriptions encoding for alarmin proteins in the acute phase of delayed drug hypersensitivity, especially in SJS/TEN [113]. Alarmins are able to recruit, activate APC and augment the adaptive immune response [114]. The involvement of the innate immune response, however, has been reported to be mainly related to dendritic cells (DCs).
In T-cell-mediated reactions, especially in the hapten or pro-hapten models, the drug or its metabolites have to be presented by mature DCs after intracellular antigen processing to be able to elicit T cell activation (Fig. 4). Therefore, it is likely that DCs play a role in the initial stages of drug sensitization. In the P-I models that do not require intracellular antigen processing, DCs have been shown to maturate and be activated directly by drug or its metabolites as danger signals [103111]. For instance, in the case of allopurinol hypersensitivity, specific T cells have been reported to be directly and immediately activated by oxypurinol, an early metabolite of allopurinol in plasma, and bound to HLA-B*58:01 without intracellular antigen processing in DCs [110]. In line with these findings, allopurinol has also been reported to be able to induce an innate immune response in a human DC cell line [115]. Therefore, it is very likely that DCs in allopurinol-induced SCARs may be activated directly by allopurinol/oxypurinol acting as danger signals. Certain drugs can change the maturational status of DCs, increasing T-cell proliferation in allergic patients in comparison with tolerant controls [111]. In addition, there is evidence emerging which demonstrates the involvement of innate immune responses in T-cell-mediated reactions in virally infected patients [10], in keeping with the hypothesis that viral infection might be able to alter the phenotype of DCs via Toll-like receptors that have the ability to present antigen to naïve T cells in draining lymph nodes after migrating to the nodes [111]. In addition, current evidence has revealed that T-cell-mediated drug reactions share characteristics with autoimmune diseases [116117], and it is proposed there may be a common pathway for both T-cell-mediated drug reactions and autoimmune diseases. Finally, in the context of interaction with other innate immune cells such as NK cells, the cross-talk may be crucial in determining whether T-cell activation occurs at the early stage of antigen recognition when the close interaction between adaptive immunity and innate immunity is formed [111]. Taken together, the evidence supports a role for innate immunity in T-cell-mediated reactions, mainly via the DCs.
FUTURE DIRECTIONS FOR RESEARCH IN HLA-ASSOCIATED SCARs
In the last decade, our knowledge of the patho-mechanisms in HLA-associated SCARs has grown considerably, particularly our understanding of the way in which T cells recognise their corresponding HLA molecules and of the role of cofactors, such as drug concentration and viral infection. Laboratory bench findings have been translated to the implementation and dissemination of HLA screening programs to prevent SCARs. Screening has not only prevented SCARs, it has freed up individuals without the risk alleles for treatment with the drugs which are the leading causes of SCARs. However, although the pharmacogenetic research has allowed us to prevent SCARs, as the majority of individuals (53% in ABC and 97% in CBZ and allopurinol), who possess these genetic risk alleles tolerate ABC, CBZ or allopurinol [10112], respectively, it has also become clear that DNA sequencing has been only the starting point of the story. A number of studies now have investigated the possible role of epigenetics (DNA methylation and posttranscription regulation by microRNAs) in the development of HLA-associated SCARs. As emerging evidence shows epigenetic factors play an important role in regulation of the immune system overall [118119120121122], further research into epigenetic influences in SCARs are drawing parallels with other immune conditions, such as systemic lupus erythematosus.
Apropos of epigenetic research, in 2017, Sun et al. [123] first studied a genome-scale DNA methylation profiling of 15 patients and 20 matched controls to determine there is an association between DNA methylation and allopurinol-induced SCARs, and validated their results by using pyro sequencing in 40 patients and 48 controls. The authors found 26 genes modified at 41 CpG islands. Of these, hypomethylation of PSORS1C1 (cg24926791) was significant in DRESS (p = 0.00127) and in SJS/TEN (p = 3.75 × 10-13) in comparison with the controls, respectively. This result suggested that the level of DNA methylation may be important in the development of allopurinol-induced SCARs. Further studies will be required to elucidate the exact role of this CpG island.
MicroRNAs (miRNAs) are short noncoding RNAs, 19–23 nucleotides long, which play various key roles in biological processes and regulation of immune responses have been estimated to regulate approximately 30% of human genes [124]. In regulating the immune response, miRNAs have been reported to be expressed specifically on different immune cells and are involved in differentiation, maturation and activation of cell effectors [125]. A number of miRNAs involved in T-cell-mediated ADRs have been identified. Overexpression of miR18a-5p in skin and serum has been demonstrated in patients with TEN, implying a link with epidermal necrolysis [126], whilst serum miR124 was proposed as a biomarker for TEN [127]. Moreover, a cellular study found that miR18a and miR155 in CBZ-specific CD4+T cells were up-regulated during their activation in a drug and time dependent manner, supporting the observations of their expression levels in serum or skin in patients [128]. More importantly, miR148a is able to regulate the expression level of HLA-C in HIV-infected patients in relation to the 3' untranslated region of HLA-C, associated with control of HIV [129]. This finding represents an example of regulation of HLA class I expression through an interaction between a miRNA and a genetic polymorphism. Taken together, studying the role of epigenetics should lead to a better understanding of T-cell-mediated ADRs in general and HLA-associated SCARs in particular.
HLA-associated SCARs then, have journeyed from the bedside to the bench and have thus enabled their prevention by pharmacogenetic screening. Researchers are now poised to discover more of the basic molecular mechanisms in immunity in general as they investigate the patho-mechanisms in SCARs.
 XML Download
XML Download