

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Eczema is a common chronic childhood skin disease with complex etiologies [1]. It may be due to a genetic deficiency in ceramide production in the skin [2] or stimulation from environmental triggers [3]. The prevalence of eczema is increasing both in Western countries such as the United States and the United Kingdom [45] and Asian countries such as China, Korea, and Japan [6]. It is estimated that 30% of Hong Kong children (approximately 160,000 children) have eczema [7]. Poor skin integrity in children with eczema leads to their stigmatization and bullying by other children, and persistent itchiness affects their school performance and quality of sleep [8]. Previous studies have highlighted that although having children with skin disease in the family affects the physical, psychological and financial aspects of the family members' quality of life (QoL), the available tools mostly target the QoL of children with eczema rather than that of their families [9]. The impact of eczema on QoL has been quantified in children and adults using established QoL measures, e.g. the Family Dermatology Life Quality Index (FDLQI) that is self-administered by parents or caregivers to assess the impact of children with eczema on their QoL. However, the Chinese version of the FDLQI (C-FDLQI) has not yet been validated in a Chinese population.
The validity and reliability of the original version of the FDLQI have been established. It has high internal consistency (Cronbach α = 0.88) and test-retest reliability (intraclass correlation coefficient, 0.94). Reportedly, FDLQI scores are strongly correlated (Spearman rank correlation = 0.69) [9] with those of Finlay and Khan's (1994) Dermatology Life Quality Index, a measure that evaluates the impact of skin disease on the QoL of an affected person aged 16 years and above [10]. The FDLQI comprises 10 items, each concerning the family member's perception of a specific impact on his/her health-related QoL (HRQoL) over the last 1 month. The impact of eczema on the HRQoL of the family is scored from none (0) to extremely severe (3), and the scores for individual items are summed to generate a total score; a higher total FDLQI score indicates a greater impairment of the family member's HRQoL [9]. The FDLQI has been translated into many languages and is used in several countries. Although the C-FDLQI is available (School of Medicine, Cardiff University, 2018), its validity and reliability have not yet been established.
This study aimed to evaluate the psychometric properties of the C-FDLQI on parents or caregivers of children with eczema in Hong Kong.
MATERIALS AND METHODS
Phase 1
The approval to determine the content validity and semantic equivalence of the C-FDLQI was obtained from the authors of the original FDLQI. The 2 FDLQI versions (original and Chinese) were reviewed and rated independently by an expert panel composed of 5 bilingual health professionals (including an academic in paediatrics, a dermatologist, an advanced practice nurse, an experienced registered nurse in paediatrics and a research associate). The content relevance of the versions was rated on a 4-point scale, ranging from not relevant (1) to very relevant (4). The content validity index (CVI) was then calculated based on the percentage of total items rated by the experts. The semantic equivalence of the items between the 2 versions was rated using a 4-point Likert scale of appropriateness, ranging from not appropriate (1) to very appropriate (4). A CVI of >0.9 and semantic equivalence of >80% for all items in the C-FDLQI were considered acceptable [11]. The average item CVI of the C-FDLQI was 0.96, and semantic equivalence between the 2 versions was 0.92.
The C-FDLQI was then tested on 10 parents of children with eczema recruited at the paediatric dermatology clinic of a regional hospital. The parents were asked to comment on the clarity of the items and the presentation of the C-FDLQI. All participants were mothers, the majority of them had a secondary school level of education and 2 mothers had a bachelor's degree. They completed the tool without requests for clarification and made no comments.
Phase 2
The psychometric testing of the C-FDLQI was conducted in the paediatric dermatology outpatient clinic of a regional hospital after receiving approval from the Joint Chinese University of Hong Kong-New Territories East Cluster (CUHK-NTEC) Clinical Research Ethics Committee, Hong Kong. Two trained research assistants screened the eligible participants through the medical records of the paediatric dermatology outpatient clinic. The inclusion criteria were parents or caregivers of 3-month- to 17-year-old children with physician-diagnosed eczema. The parents/caregivers were able to read and speak Cantonese and were free from psychiatric disorders. The parents/caregivers were excluded if their children had acute or chronic illnesses requiring systemic treatment. The participants were recruited using convenience sampling. The target sample size for a 10-item tool was considered 100 participants in accordance with the recommendation of at least 10 participants per parameter for factor analysis [12]. This sample size was also anticipated to be adequate for examining other psychometric properties of the C-FDLQI, including internal consistency, test-retest reliability, and convergent validity. The participants were asked to complete a demographic form that included questions about their age, sex, education level, career, and the age of their children, as well as the self-reported C-FDLQI. The participants were also asked whether they had any questions or difficulties while completing the questionnaires. Fifty of them (the first 50 participants recruited in the study) were asked to complete a second identical questionnaire 2 days after the baseline assessment to ensure that the children's skin condition had remained the same [13] for test-retest reliability.
The internal consistency and test-retest reliability of the tool were assessed using Cronbach α and weighted kappa (κ), respectively. The convergent validity (a subtype of construct validity) of the C-FDLQI was evaluated by examining the correlations of the C-FDLQI with SCORing Atopic Dermatitis (SCORAD), the Cantonese version of the Children's Dermatology Life Quality Index (C-CDLQI), and the Chinese adaptation of Generic Self-Efficacy scale (C-GSE). Pearson r was used for normally distributed data, and the Spearman rank correlation coefficient (ρ) was used for nonnormally distributed data [14]. Known-group comparison was performed based on the hypothesis that parents/caregivers of children with moderate to severe eczema achieve higher scores in the C-FDLQI than the parents/caregivers of children with mild eczema. The structural validity of the C-FDLQI was assessed by confirmatory factor analysis to test the single-factor structure.
Measurements
Grading of eczema severity
The severity of eczema symptoms [15] is most commonly assessed using the SCORAD index developed by Kunz et al. [16] The index is based on individual items about the intensity of the affected area, including erythema, oedema/papulation, oozing/crusts, excoriations, lichenification and dryness, with each item rated on a scale of 0 to 3. The extent of the affected area is determined using the ‘rule of nines' with a maximum score of 83. The subjective symptoms are the effects of daytime pruritus and sleep loss rated on an analogue scale of 0 to 10. The tool assesses disease severity with a maximum score of 103 and categorizes the severity as mild (<25), moderate (25–50) or severe (>50). The 3 index parameters of the SCORAD showed strong correlation with one another (r = 0.79 [p < 0.0001] between extent and intensity; r = 0.71 [p = 0.0001] between extent and subjective symptoms; and r = 0.91 [p < 0.0001] between intensity and subjective symptoms) [17].
Quality of life
The original CDLQI was developed by Lewis-Jones and Finlay [18] to determine how skin diseases affect the daily lives of children aged 3–16 years. It comprises 10 questions with a maximum possible score of 30 and a minimum score of 0. A higher score indicates a lower QoL. The CDLQI was completed by 233 children who attended a dermatology outpatient clinic (mean score ± standard deviation [SD], 5.13 ± 4.9) and 102 children without skin disease (mean score ± SD, 0.38 ± 0.74). Its test-retest repeatability on 46 paediatric dermatology patients showed a mean difference of 0.28 between the baseline and retest scores. The Spearman correlation coefficient was 0.86 (p < 0.001) between the standard deviation of the difference and the standard deviation of the measurement [18]. Chuh [19] evaluated the effects of dermatological conditions on the QoL of 5- to 16-year-old children using the C-CDLQI. The results revealed that the C-CDLQI demonstrated high internal consistency (Cronbach α = 0.83), good test-retest reliability (Pearson r = 0.96, p < 0.01) and a strong correlation with the severity of skin problems (Pearson r = 0.85, p < 0.01) [19]. Although the CDLQI is a self-administered questionnaire, the parents/caregivers could assist their child in completing it if the children were too young.
Self-efficacy
The self-efficacy of children was measured using the GSE scale, which was developed by Schwarzer and Jerusalem [20] to assess the general sense of perceived self-efficacy to predict coping with daily hassles and adaptation after experiencing all kinds of stressful life events. The internal consistency (Cronbach α) of the GSE scale ranges from 0.75 to 0.90. Schwarzer, Bäßler, Kwiatek, Schröder, and Zhang [21] tested the C-GSE scale on 293 first-year undergraduates. The results revealed a Cronbach α of 0.92, and principal component analyses revealed eigenvalues of 5.49, 0.84 and 0.74. This 10-item tool is scored on a 4-point Likert scale, ranging from ‘not at all true’ to ‘exactly true.’ A higher GSE score indicates better self-efficacy.
Data analysis
All statistical analyses except confirmatory factor analysis were performed using the IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA). Descriptive statistics (means, SD, frequencies, and percentages) were used to summarise the demographic and clinical characteristics of parents/caregivers and their children and the scores of the measurement tools. Data normality was checked using skewness statistics and normal probability plot. Internal consistency was assessed using Cronbach α that indicated pairwise correlations between tested items. A reliability coefficient α of ≥0.70 was considered to indicate acceptable reliability [22]. Weighted κ was used to assess the item-to-item agreement between 2-time points for the ordinal data [23]. A κ value of <0.4 was considered to represent poor agreement; between 0.4 and 0.75, acceptable agreement; and >0.75, a high level of agreement. Pearson r and Spearman ρ were used to evaluate convergent validity for normally and nonnormally distributed data, respectively. A correlation coefficient of >0.40 was considered to indicate adequate convergent validity [22]. Confirmatory factor analysis was performed using Lisrel 9.3 (Scientific Software International, Inc.) to examine the structural validity of the tool. The one-factor structure of the tool was evaluated using goodness-of-fit indices, including the chi-square value, root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR) and non-normed fit index (NNFI). An insignificant chi-square value indicates a good fit. Smaller RMSEA and SRMR values indicate a better fit: values ≤0.05 (for both RMSEA and SRMR) indicate a good fit, and values >0.05 but ≤0.08 (for RMSEA) and ≤0.10 (for SRMR) indicate an acceptable fit [24]. The NNFI usually ranges from 0 to 1, with values ≥0.95 but <0.97 indicating an acceptable fit and values ≥0.97 indicating a good fit [24]. All statistical tests were two-sided, and a p value of <0.05 was considered to be statistically significant.
Ethical considerations
Ethical approval for the study was obtained from the Joint CUHK-NTEC Cluster Research Ethics Committee. The participants' rights and safety were protected by adhering to the Hong Kong Personal Data (Privacy) Ordinance, the Declaration of Helsinki and institutional policies. The eligible parents/caregivers were told the aim and procedure of the study and were informed of their right to confidentiality and to withdraw from the study without negative consequences to their children's current medical regimens in the hospital. Informed consent was obtained from the participating parents/caregivers, and assent was obtained from the participating children and adolescents. Participation was voluntary, and all collected data were kept strictly confidential and will be destroyed 6 years after the completion of the study.
RESULTS
Sample characteristics
Of the 155 eligible parents/caregivers approached to participate in the study, 147 parents/caregivers of 3-month- to 17-year-old children with physician-diagnosed eczema were recruited as a convenience sample with child-parent dyad as the unit of analysis (response rate, 94.8%). Eight participants refused to participate because of a lack of interest. To assess the test-retest reliability of the C-FDLQI, 50 participants were asked to complete a second identical questionnaire 2 days after the baseline assessment. There were no significant differences in baseline and clinical characteristics between participants in the retest and no retest groups. The majority of the participants were mothers (120 [81.6%]), followed by fathers (21 [14.3%]) and caregivers, including grandparents and uncles (6 [4.1%]). Most of the participants were 40–50 years old (57.1%), and 29.9% of the participants were 29–39 years old. Approximately 72.8% of the participants had <12-year-old children. Based on the SCORAD index [16], 81 participants (55.1%) had children with mild eczema, whereas 66 (44.9%) had children with moderate to severe eczema. The majority of the participants were female and Hong Kong residents (85% and 92.5%, respectively) (Table 1).
Table 1
Demographic and clinical characteristics of the family participants (n = 147)

Values are presented as number (%) or mean ± standard deviation.
C-CDLQI, Children's Dermatology Life Quality Index in Cantonese version; C-FDLQI, Chinese version of the Family Dermatology Life Quality Index; C-GSE, Chinese Adaptation of the General Self-Efficacy Scale; SCORAD, SCORing Atopic Dermatitis.
Internal consistency
The C-FDLQI demonstrated good internal consistency with a Cronbach α of 0.95. The means and standard deviations of the items were similar, indicating that they have the same concept. In addition, the Cronbach α for all items remained close to the current score of the C-FDLQI even if one item was deleted; thus, all items were retained in the translated version (Table 2).
Table 2
Descriptive and reliability statistics of the Chinese version of the Family Dermatology Life Quality Index (C-FDLQI) (n = 147)
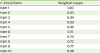
Test-retest reliability
The test-retest reliability was good. The good item-to-item agreement was found for each item of the C-FDLQI, with weighted κ ranging from 0.70 to 1.00 (Table 3).
Convergent validity
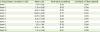
Pearson r and independent t test were used to evaluate the convergent validity of the normally distributed scores of the C-FDLQI. The total scores of the C-FDLQI showed positive correlations with those of the SCORAD (Pearson r = 0.62, p < 0.001) and C-CDLQI (Pearson r = 0.75, p < 0.001) but a significant negative correlation with those of the C-GSE (Pearson r = -0.28, p < 0.001) (Table 4). Known-group comparisons between the parents/caregivers of children with mild eczema and those of children with moderate to severe eczema showed significant differences as assessed by independent t test (t = -7.343, p < 0.001). These findings indicated that the C-FDLQI had acceptable convergent validity.
Table 4
Pearson coefficients of correlation of the total score of C-FDLQI against the SCORAD, C-CDLQI, and C-GSE (n = 147)

C-CDLQI, Children's Dermatology Life Quality Index in Cantonese version; C-FDLQI, Chinese version of the Family Dermatology Life Quality Index; C-GSE, Chinese Adaptation of the General Self-Efficacy Scale; SCORAD, SCORing Atopic Dermatitis.
*Correlation is significant at the 0.05 level (2-tailed). **Correlation is significant at the 0.01 level (2-tailed).
The C-FDLQI showed no statistically significant associations with gender, education level or career of the parents/caregivers of children with eczema.
Construct validity
The structure validity of the one-factor structure of the C-FDLQI was evaluated by confirmatory factor analysis. All goodness-of-fit indices (χ2 = 44.4, df [degrees of freedom] = 35, p = 0.132, RMSEA = 0.043, SRMR = 0.029, and NNFI = 1.0) indicated that the one-factor structure of the C-FDLQI showed a good fit to the data. All items showed significantly high loadings of >0.84, indicating that the latent construct of the C-FDLQI was well reflected by the items (Fig. 1).

DISCUSSION
This study was the first to examine the reliability and validity of the C-FDLQI in parents/caregivers of children with eczema in Hong Kong. The results showed that the C-FDLQI has high internal consistency. Further, significant positive correlations were observed between the total scores of C-FDLQI and C-CDLQI, suggesting that the poor QoL of children with eczema was associated with the poor QoL of their family members. The total scores of the C-FDLQI showed positive correlations with those of the C-CDLQI and SCORAD, but significant negative correlations with those of the C-GSE. These results indicate that the severity of children's eczema symptoms affects the QoL of both children and their parents/caregivers. However, better self-efficacy in administering treatment contributed to less severe eczema symptoms.
Over 70% of the participants reported that the difficulty level of the tools was acceptable. Their main comment was that the questions of the C-GSE were too vague to answer. However, the C-GSE was the only validated tool available in the Chinese version for measuring self-efficacy for comparison with the other tool. Taken together, the results suggest that the C-FDLQI can be used to facilitate the accurate evaluation of the QoL of parents/caregivers of children with eczema for effective eczema management in the future.
As the participants were recruited from only one paediatric dermatology outpatient clinic in a regional hospital and the majority were mothers aged 39–49 years, some bias in the findings is likely. Therefore, the results may not be generalizable to the entire population of parents of children with eczema. Further studies in different settings and different populations are warranted. Moreover, the C-FDLQI is a self-report tool; thus, the findings may be biased because of a difference in the interpretation of the questions between the participants. Different modes of administering the C-FDLQI, such as using an electronic device, should be evaluated in future studies to ensure the accuracy of the findings and explore the differences in the participants' responses. Finally, parents/caregivers had to assist very young children in completing the CDLQI; thus, reporters' assumptions and biases could have affected the internal validity of the study.
In conclusion, the results suggest that the C-FDLQI is a reliable and valid tool for measuring the QoL of Chinese parents or caregivers of children with eczema, and the findings were comparable to those of a previous study that demonstrated that the C-FDLQI is a simple and practical instrument.
 XML Download
XML Download