

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cardiac implantable electrical device (CIED) therapy reduces morbidity and mortality in appropriately selected patients,1)2) but this benefit is thought to be mitigated by complications, including infection.3) Infection in a permanently implanted CIED is a serious complication. It may occur either as a surgical site infection occurring within 1 year after implantation,4) or as late-onset lead endocarditis. CIED implantation rates are on the rise worldwide,5) and the population of patients living with a CIED is growing. As a consequence, CIED infections are also increasing. Although it is well recognized that the rate of CIED infection is increasing faster than the rate of CIED implantation,6)7) there are limited published data on the risk-adjusted mortality and cost associated with CIED infection or the relationship of these outcomes to different CIED types, especially in Asian countries.
Several studies8)9)11) have identified risk factors for infection in permanent CIED systems. However, the results of these studies are somewhat contradictory, and the risk factors for such infections have not been studied in a large cohort. This study sought to define the CIED infection rate, risk factors and cost with infection.
METHODS
Data source
In the Korea, almost the entire population has health insurance through National Health Insurance (NHI) or Medical Aid. Hospitals and clinics submit inpatient and outpatient claims data on spent cost covered by NHI or Medical Aid programs for reimbursement to the Health Insurance Review & Assessment Service (HIRA), which assesses the quality of the medical practice. HIRA collects patient clinical data through insurance claims, and the HIRA database is mainly open to researchers with academic or public policy purposes.12) The following information is provided: patients' gender and age information, their use of inpatient and outpatient services, pharmacy dispensing claims, medical device usage, and mortality data. This study was approved by the Institutional Review Board of Korea National Institute for Bioethics Policy (P01-201708-21-011), and informed consent was waived.
Study population
From the entire Korean population in the Korean HIRA database, 16,963 patients with newly-implanted CIED who were aged 19 years or older were identified during the period from January 1, 2014 to December 31, 2016. The study cohort was consisted of all admissions that included a procedure for CIED generator implantation, replacement, or revision identified using the corresponding NHI procedure codes for pacemakers (O0203, O0204, O0205, O0206, O0208, O0209 and O0210), implantable cardioverter defibrillators (ICDs) (O0211 and O0212), cardiac resynchronization therapy devices with defibrillator (CRT-D) (O0211 and O0212), or cardiac resynchronization therapy devices without defibrillator (CRT-P) (O0203,O0204, O0205 and O0206). The following were exclusion criteria: 1) those who were hospitalized less than 1 day (n=36), 2) those who had undergone epicardial pacemaker implantation (n=19). Finally, we included 16,908 patients who performed new CIED implantation (Figure 1). We excluded patient with hospital stay less than 24 hours to prevent the erroneous case from being included in the study because it is rare for patient with pacemaker implantation was discharged within a day. We excluded epicardial pacemaker because of different procedure and higher complication rate than percutaneous pacemaker implantation.
Figure 1
Study population.
CIED = cardiac implantable electrical device; HIRA = Health Insurance Review & Assessment Service; NHI = National Health Insurance.

Infection was identified using the Korean Standard Classification of Disease (KCD), Seventh Revision diagnosis codes for infection due to a cardiac and vascular device (T80, T81, T82 and T87), bacteremia (A48 and A49), septicemia (A40 and A41), shock (R57), or fever (R50). Admissions that included only electrode implantation, replacement, or revision without evidence of infection were not considered as infection.3)13) The type of CIED was classified to pacemaker, ICD and CRT-D/P. The pacemaker and ICD were subclassified as single chamber and dual chamber.
The more detailed definitions of CIED related procedures, devices and infections are presented in Supplementary Table 1. ICD-10 codes used for defining the comorbidities are presented in Supplementary Table 2.
Outcomes
Our analysis had 3 primary outcomes: infection, admission length of hospital stay, and admission cost. Admission costs were calculated with the method used by the Korean NHI to calculate costs for establishing payment rates under the Fee-For-Services System.
Statistical analysis
Continuous variables were expressed as mean±standard deviation (SD) and categorical variables were reported as frequencies (percentages). The categorical variables were compared by Fisher's exact test or Pearson χ2 test, and continuous variables were compared by the Student's t-test. Crude incidence rates for CIED infections were calculated by dividing the number of incident cases of CIED infection by the number of person-years accumulated in the population with CIED implantation or replacement.14) The 95% confidence interval (CI) and p value for difference between two incidence rates were calculated using the Poisson approximation. Kaplan-Meier survival curves for CIED infection according to implantation condition were constructed and compared using a log-rank test. Patients were censored at the time of death, end of follow-up, or other termination of CIED treatment. In order to investigate the association between the clinical conditions and the CIED infection, we used Cox proportional hazards regression models. The factors considered in the models are age, sex, and clinical variables, including replacement (vs. first implantation), diabetes mellitus, hypertension, congestive heart failure, and single chamber (vs. dual chamber). These variables used to construct the model were based on the results of previous studies that reported independent risk factors for CIED infection.15)16) Results are presented as hazard ratios±95% CIs. For the multiple regression model, only the risk factors in the final model are presented. All the tests were two-tailed, and p<0.05 was considered significant. The regressions were estimated using with SAS version 9.3 (SAS Institute Inc, Cary, NC, USA).
RESULTS
The characteristics of patients
A total of 16,908 patients underwent one or more CIED implantations during the study period. The numbers of pacemaker, ICD and CRT implantation were 13,440 (79.5%), 2,712 (16.0%) and 698 (4.1%), respectively. The proportions of first implantation and replacement were 77.6% (n=13,113) and 22.4% (n=3,795), respectively. One or more CIED replacements were carried out in 3,795 (22.4%) patients. Patient characteristics at the time of first CIED implantation or replacement are shown in Table 1.
Table 1
The comparison of clinical characteristics of patients with first implantation and replacement of CIED
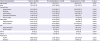
Data are presented as mean±standard deviation for continuous variables. Numbers in parenthesis are percentage.
CIED = cardiac implantable electrical device; CKD = chronic kidney disease; CRT-D = cardiac resynchronization therapy devices with defibrillator; CRT-P = cardiac resynchronization therapy devices without defibrillator; ESRD = end-stage renal disease; ICD = implantable cardioverter defibrillator.
During the study period, CIEDs were removed without replacement in 229 (1.4%) patients. Whereas, the remaining 16,679 (98.6%) patients were living with an implanted CIED at the end of the study period.
Infections
During the follow-up period of 17.1±10.6 months, a total of 462 patients had infection with the incidence of 1.95/100 person-years. Among 462 patients with CIED infection, 132 (28.6%) patients had undergone the implantation of new CIED after the removal of infected CIED. The comparison of baseline characteristics of non-infected and infected groups is presented in Table 2. Compared with non-infected group, infected group was older, included more male, and had comorbidities and replacement more frequently. Single chamber pacemaker and ICD, and CRT-P were more frequently implanted, and aspirin or warfarin were more frequently prescribed in infected than non-infected groups.
Table 2
The comparison of clinical characteristics of non-infected and infected patients with CIED
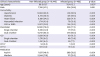
Data are presented as mean±standard deviation for continuous variables. Numbers in parenthesis are percentage.
CIED = cardiac implantable electrical device; CKD = chronic kidney disease; CRT-D = cardiac resynchronization therapy devices with defibrillator; CRT-P = cardiac resynchronization therapy devices without defibrillator; ESRD = end-stage renal disease; ICD = implantable cardioverter defibrillator.
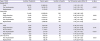
Table 3 shows infection rate according to type of CIED and first implantation or replacement. After the first CIED implantation, 259 had infection with the incidence of 1.4/100 person-years. Whereas after replacement, 203 had infection with the incidence of 3.97/1,000 person-years. CIED infection rate was higher after the replacement than the first CIED implantation (p<0.001). The incidence of infection was 1.88, 2.26 and 2.26/100 person-years in pacemaker, ICD and CRT-P/D, respectively. In both pacemaker and ICD, there was no difference in infection rate between single and dual chamber.
Table 3
Infection rate according to first implantation or replacement, and type of CIED
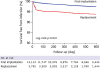
The time to CIED infection is illustrated by Kaplan-Meier plots in Figure 2. After first implantation, infection occurred continuously. However, after replacement, the rate of infection increased abruptly at first 50 days, and increased continuously after 50 days.
Risk factors associated with infection
Our simple regression analysis indicated that the risk of CIED infection was increased by replacement, diabetes mellitus, hypertension, congestive heart failure, single chamber and older age.
According to our multiple regression analysis, the risk of CIED infection was increased by replacement with adjusted hazard ratio (aHR) of 3.15 (95% CI, 2.60–3.78), diabetes with aHR of 1.94 (95% CI, 1.58–2.38), and congestive heart failure with aHR of 1.86 (95% CI, 1.51–2.50) (Table 4).
Table 4
The risk factors of CIED infection

aHR = adjusted hazard ratio; CI = confidence interval; CIED = cardiac implantable electrical device; HR = hazard ratio.
*The factors considered in the models are age, sex, and clinical variables, including replacement (vs. first implantation), diabetes mellitus, hypertension, congestive heart failure, and single chamber (vs. dual chamber).
Hospitalization duration and medical cost related to cardiac implantable electrical device infection
The average hospitalization was 14.1±9.3 and 17.2±12.4 days for CIED infection after first implantation and replacement, respectively. The duration of hospitalization was significantly longer for replacement than first implantation of CIED (p=0.002). There was no significant difference of duration of hospitalization for CIED infection among pacemaker, ICD and CRT-P/D.
The average cost per person related to CIED infection was US$17,105. The average cost of replacement was more expensive than that of first implantation ($17,591±13,688 vs. $15,795±9,544, p=0.009). Compared with that of pacemaker ($13,736±10,049), the average costs for ICD ($28,402±8,448) and CRT-P/D ($29,674±9,012) were more expensive in CIED infection (Table 5).
Table 5
Hospitalization duration and medical cost related to CIED infection
DISCUSSION
The present study represents the nationwide population-based study of CIED infections, associated risk factors and medical cost of infection after first CIED implantations and CIED replacements. This study also provides the device type–specific estimates of cost associated with CIED infection in the current era of CIED use in Korea. Second, the replacement of CIED were associated with a substantial incremental risk of CIED infection. Although the majority of infections occurred within the first year of follow-up, a large number of infections were found to occur during the late follow-up period, >1 year post-implantation. This very late onset of infection is consistent with the findings from other studies that consider extended follow-up periods9)10)17) and with the current understanding of slowly progressing, implant-related infection.18)
The incidence of CIED infection in our population was 1.41 per 100 person-years after the first implantation. This is similar to the rate of other epidemiological studies that include long-term follow-up have calculated cumulative rates per patient or device and report infection rates of 2.210) and 1.6%,9) respectively. The effect of this difference is unclear; the rate of infection in ICD systems has been reported to be similar to the rates observed for pacemaker systems.9)10)
The infection rate after CIED replacement was almost 2.64 times higher than that of first CIED implantation. This increase is similar was previous study that the incidence of surgical site infection was 4.82/1,000 pacemaker-years after first pacemaker implantation and 12.12/1,000 pacemaker-years after pacemaker replacement.16)
The substantially elevated risk of infection after CIED replacements and other repeated procedures observed in the present study has been reported previously.9)10)11)19) The increased risk of infection after repeated procedures argues strongly that industry should improve CIED batteries and that physicians should increase device longevity by appropriately programming CIED parameters. Furthermore, the increased risk of infection after repeated procedures should be considered in the decision-making process when handling device recalls,20) which are a common reason for premature repeated procedures. In each patient, the benefits of replacing the hardware should be balanced with the increased risk of device infection.
At first glance, the higher risk of infection after repeated procedures (most often simple CIED replacements) is unexpected, as these procedures most often involve only a minor surgical revision and are short-lasting compared with first implantations. It is generally recognized, however, that revision surgery is an important risk factor for the infection of an implanted prosthesis or device.21) Our findings could likely be explained by the fact that CIED pockets can be colonized by bacteria, even in the absence of any initial clinical signs of infection.22) In combination with the limited immunological response of the fibrous and poorly vascularized CIED pocket that is opened during replacement or revision procedures,23) the rapid formation of a microbial biofilm24) by either latent or perioperative inoculation of pathogens may be favored, thereby allowing pocket infection.
Beside CIED replacement, we also found that diabetes and hypertension were important risk factors. Prior studies have suggested that male sex, younger age, diabetes, underlying heart disease, implantation during the earliest part of the study period, and absence of antibiotics were associated with an increased risk of CIED infection.10)11)15)16)17) This study did not evaluated other potentially important procedure-related factors including the size of the implanting center, the complexity of the procedure, and the number of leads.
There are few published data on the current cost of managing CIED infection. Moreover, these analyses do not reflect the current patient population receiving CIED therapy. In US Medicare patients, the standardized adjusted incremental and total admission costs with infection were $14,360 to $16,498 and $28,676 to $53,349, respectively, depending on CIED type.25)
Although it is important to reduce admission costs associated with CIED infection, preventing infections or reducing the severity of infections through early detection would have a significant impact on both mortality and cost associated with these infections.
The present study is a retrospective analysis, and thus bears the inherent limitations of such studies. First, infections identified using KCD codes for cardiac or vascular device infection, or cardinal manifestations of infection, in the setting of a CIED implantation, were presumed to be CIED infections. We took an approach similar to Voigt et al.6)26) that incorporates multiple distinct code-based criteria to increase the sensitivity of the search. Because the rate of lead extraction is relatively low in Korea, we could not identify CIED infection using lead extraction. Moreover, we could not distinguish between major and minor infections. Second, we were not able to distinguish whether removal of the pacemaker system was due to infection arising from a device pocket infection or from a bloodstream infection of the intravascular portion of the system. However, data suggest an overlap between these two events.27)28) Third, although heterogeneous baselines imply potential interactions between replacement and diabetes mellitus and/or heart failure, this possibility was not investigated. Fourth, in this study, data from 2014 to 2016 were extracted and utilized for drawing results. Hence, these results may not properly capture current rates of CIED implantation (and related infection rates) if CIED is growing perhaps fast. Finally, the recent methods of lead extraction, such as lasers or mechanical sheaths were not available. Therefore, this study may underestimate the incremental admission cost with infection. Despite these limitations, we believe these data provide useful insights into mortality and cost associated with infection of CIED as they are being used in current practice.
In conclusion, the rate of CIED infection in Korea was 1.95 per 100 person-years with average cost of US$ 16,584. The most important risk factor was generator replacement. This result suggests that generator replacement should be performed cautiously to avoid CIED infection. Further research to reduce the incidence of CIED infection during generator replacement is warranted.
 XML Download
XML Download