

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since the first heart transplantation (HTx) in Korea was performed in 1992, HTxs have improved survival of end-stage heart failure patients.1)2)3) The Korean Organ Transplant Registry (KOTRY) was created to provide current data regarding recipient, donor, and transplant characteristics as well as post-transplant outcomes. The KOTRY was founded by the Korean Society of Transplant and Korea Center for Disease Control in 2014, and was the first nationwide organ transplant registry in Korea. This second Korean Heart Transplant Registry biannual report is based on KOTRY data submitted on 400 HTxs in adult recipients from March 2014 to December 2017.
METHODS
Data collection
Data are submitted to the KOTRY by medical centers nationwide. As described in the first report of the Korean Heart Transplant Registry,4) HTx patients from 4 nationally representative medical centers were consecutively enrolled upon transplant and followed. The study was reviewed and approved by the Institutional Review Board of each transplantation center. Detailed information regarding collected data and definition of comorbidities are described in the first report of the Korean Heart Transplant Registry.4) After transplant, follow-up visits were recorded at 1, 6, and 12 months, and annually thereafter. Among the 400 patients, 4 did not finish follow-up. Consequently, data from 400 HTxs were available from March 2014 to December 2017. Summary data are provided for the entire cohort of patients along with additional analyses focused on trends of the more recent cohort who received a transplant from January 2016 to December 2017, compared to the previous cohort who received a transplant from March 2014 to December 2015.
Statistical analysis
Continuous variables are recorded as mean±standard deviation and categorical variables are reported as frequency and percentages. Baseline recipient/donor characteristics and clinical outcomes of HTxs were compared according to transplant year. One-way analysis of variance was used for continuous variables and χ2 test for categorical variables. One-year and intermediate-term survival analysis was performed using Kaplan-Meier analysis. Univariate and multivariate Cox regression analyses were performed to determine independent variables for post-transplant mortality at 6 months and 2 years after HTx. A 2-sided p value<0.05 was accepted as indicating statistical significance. All data were analyzed using SPSS version 22.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
HTx donor and recipient demographics and characteristics
Transplant volume
A total of 400 HTxs were performed at 4 centers from March 2014 to December 2017. Since the first report of the KOTRY HTx report, 216 HTxs were performed through December 2017 (2016, n=106 and 2017, n=110) (Supplementary Figure 1). The total number of HTxs nationwide from April 2014 to December 2017 was 575, and this registry captured an estimated 70% of HTxs. The number of HTxs per year was steady over the 4-year period.
Donor demographics
Donor demographics are presented in Table 1. From the KOTRY registry, 72% of donors were male, and female donor-to-male recipient transplantation occurred slightly more often in 2017 (20%) than in previous years (2014–2015, 14% and 2016, 12%). Donor diabetes mellitus and hypertension were rare but rose slightly. The leading cause of donor death was intracranial hemorrhage (43% in 2016, 51% in 2017, and 49% in the overall cohort). Donor age is addressed in detail in section 6.
Table 1
Donor and recipient characteristics

Data are shown as mean±standard deviation or number.
ACC = aortic cross-clamp; BMI = body mass index; CPB = cardiopulmonary bypass; Cr = creatinine; ECMO = extracorporeal membrane oxygenation; HLA = human leukocyte antigen; IABP = intraaortic balloon pump; LVAD = left ventricular assisting device; PRA = panel reactive antibodies; RVSP = right ventricular systolic pressure; HTx = heart transplantation.
*p<0.05 compare to 2014–2015; †p<0.05 compared to 2016; ‡p<0.05 compared to 2017.
Recipient demographics and characteristics
As shown in Table 1, cardiomyopathy was the leading underlying heart disease diagnosis, and the proportions of coronary artery disease and valvular heart disease increased over time. Use of mechanical circulatory support to bridge patients to transplant increased over time (Supplementary Figure 2), predominantly with extracorporeal membrane oxygenation (ECMO) devices. The proportion of ECMO therapy to bridge patients increased steeply from 2016 to 2017 compared to previous years. The proportion of patients who were on mechanical ventilators also increased over time. These changes over time suggest a tendency to transplant higher risk patients.
Survival
For the 400 HTxs between March 2014 to December 2017, 1-year survival was 90%. Kaplan-Meier survival curves showed similar survival rates over time, although survival rates were slightly lower in 2016 (Supplementary Figure 3). One-year and long-term survival rates showed different trends according to heart disease diagnosis, although the differences were statistically insignificant (Figure 1). Patients who underwent HTx as a retransplant showed the lowest 1-year survival, while patients who underwent transplant due to cardiomyopathy and congenital heart disease showed the highest 1-year survival (Figure 1A). In patients who survived the first year after transplant, survival reached a plateau, except in those who received transplants for coronary artery disease (Figure 1B). Long-term survival remained the worst in those who underwent retransplant and best in those who underwent transplant for cardiomyopathy and congenital heart disease.
Figure 1
Kaplan-Meier (A) 1-year survival, and (B) long-term survival by diagnosis (cardiomyopathy, coronary artery disease, congenital diagnosis, retransplant, and valvular heart disease).

One-year survival was significantly lower in patients with pre-transplant ECMO (79%) compared to no pre-transplant mechanical support (93%) (Figure 2A). Pre-transplant mechanical device support other than ECMO included intraaortic balloon pump and left ventricular assisting device (LVAD) and was associated with a lower 1-year survival rate (85.7%) compared to those without any pre-transplant mechanical device support, but the trend did not reach statistical significance, most likely due to the small number of patients. Long-term survival was worst in patients with pre-transplant ECMO (78%) compared to others (patients with mechanical device support other than ECMO, 86% and no pre-transplant mechanical device support, 92%). Pre-transplant ECMO remained associated with a significantly worse prognosis after HTx. Supplementary Figure 4 shows 1-year and intermediate term survival outcomes with respect to pre-transplant support. Pre-transplant ECMO with ventilator care had the worst outcomes compared to patients with pre-transplant ECMO without a ventilator or those without ECMO or a ventilator. Supplementary Figure 5 shows cause of death by time of death after transplant. Infection was the most common reason for mortality after the first month and first year.
Figure 2
Kaplan-Meier analysis by pre-transplant durable mechanical circulatory support use (transplant March 2014–December 2017). LVAD vs. ECMO vs. NO LVAD/ECMO, inotropes vs. no inotropes. Comparison of (A) 1-year survival and (B) intermediate-term survival by pre-transplant durable mechanical circulatory support use.
ECMO = extracorporeal membrane oxygenation; LVAD = left ventricular assisting device.

Immunosuppression and rejection
Induction immunosuppression
A total of 359 patients were treated with immunosuppressive induction treatment (2 were treated with anti-thymocyte antibodies, and the rest with the interleukin-2 receptor antagonist basiliximab).
Maintenance immunosuppression
Immunosuppression at discharge by times is described in Supplementary Figure 6. Tacrolimus was continuously used as the preferable calcineurin inhibitor at discharge (Supplementary Figure 6A), while the use of cyclosporine decreased over time. Mycophenolate mofetil (MMF) was consistently the preferred cell cycle inhibitor, and there was constant usage of the mammalian target of rapamycin inhibitor everolimus (sirolimus was not used). Steroid use slightly, but significantly, declined over time at discharge.
Similar trends were observed in the usage of immunosuppressive agents at 1-year follow-up. Tacrolimus was the most frequently used calcineurin inhibitor, and only a few patients were taking cyclosporine over time (n=18, 10% at 2014–2015 and n=5, 5% at 2016). Usage of MMF (84% at 2014–2015 vs. 91% at 2016) and everolimus (33% at 2014–2015 and 34% at 2016) was stable, while steroid use decreased over time (82% at 2014–2015 and 72% at 2016).
Rejection
The incidence of rejection between discharge and 1-year follow-up slightly decreased over time (Supplementary Table 1). The incidence of treated rejection also decreased over time. Intermediate survival rates in patients with no rejection and treated/untreated rejection did not differ (Supplementary Figure 7). Most diagnosed rejection was based on a pathologic diagnosis from a protocol biopsy (pathologic rejection grades were acquired in 205 patients: incidence of grade 1R was 182, 46%; 2R was 22, 6%; and 3R was 1, 0.5%).
Post-transplant morbidity
The most common post-transplant morbidities are shown in Supplementary Table 2. The most common morbidity was hypertension, followed by diabetes. Cardiac allograft vasculopathy was diagnosed in 5.8% of patients within 1 year after HTx.
Multivariate analyses
To determine independent contributors to mortality and morbidity, we performed multivariate proportional hazard regression analyses for transplants that took place from 2014 to 2017, using donor and recipient pre-transplant and recipient post-transplant characteristics as independent variables. Variables associated with risk of 6-month and 2-year mortality are reported in Supplementary Table 3.
When analyzing 6-month mortality, only pre-transplant data were considered. In univariate analyses, previous history of HTx, recipient pre-transplant dialysis, pre-transplant ECMO treatment vs. non-mechanical device support and pre-transplant recipient ventilator support were significantly associated with 6-month mortality. In the multivariate analysis, previous HTx history and recipient history of dialysis remained independently associated with 6-month mortality. For 2-year mortality, post-comorbidities were considered. In univariate analyses, recipient age, pre-transplant ECMO, post-transplant renal replacement therapy, post-ECMO, post-transplant dialysis, and post-transplant tuberculosis were significant predictors. In the multivariate analysis, recipient age, pre-transplant ECMO, post-transplant dialysis, and post-transplant tuberculosis were independently associated with 2-year mortality. Post-transplant tuberculosis may have contributed to 2-year mortality due to the significant interactions between tuberculosis medication and immunosuppressive agents. Also, high mortality rates of tuberculosis in solid organ transplant patients because of difficulty in treating tuberculosis due to length of therapy may have been reflected in this data.5)
2018 report focus: age
Heart failure care has improved due to medications and circulatory supporting devices. As society ages, the number of older potential recipients is increasing, and introduction of LVAD use has implications for transplant recipient age. With issues of recipient demand/donor supply dilemma and formal or informal alternate lists with marginal donors, more and more centers are also accepting older donors.
Age and HTx demographics and characteristics
Supplementary Figures 8 and 9 depict the age distribution of donors and recipients according to transplant year. The mean recipient age did not differ significantly between years. The age group of 40–59 was the largest, and a small number of recipients older than 70 years did undergo HTx (3.3% in 2014–2015, 4% in 2016, and 1% in 2017). In contrast, donor age increased significantly over the 4-year period (Table 1). In 2014–2015, the proportion of donors aged ≤39 and 40–59 was similar (46.2% and 53.8%, respectively). In 2016 and 2017, the proportion of donors aged 40–59 surpassed 60% (64.2% and 61.8%, respectively) (Supplementary Figure 9). In 2017, 2% of donors were in the age group of 60–69.
Table 2 describes the clinical features of recipients according to different recipient age groups. Mean donor age increased as recipient age increased, and the donor-recipient age difference was larger with the increasing age of recipients. Male recipients predominated in all age groups. As shown in Supplementary Figure 10, the diagnosis of underlying heart disease varied significantly according to age group. Cardiomyopathy remained the major cause for HTx in all age groups, but was most prevalent in the age ≥70 (82%) group, followed by the age ≤39 group. Coronary artery disease was the second most common cause of underlying heart disease, except in the age ≤39 group.
Table 2
Donor and recipient characteristics by recipient age group (transplant March 2014–December 2017)

Older age recipients showed higher pre-transplant creatinine levels and right ventricular systolic pressure. One-year mortality did not differ among age groups, but intermediate-term survival (mean follow-up duration: 26.5±15.4 months) was significantly worse in recipients ≥70 years old compared to the other groups (Figure 3).
Figure 3
Kaplan-Meier survival by recipient age (transplant March 2014–May 2018).
Comparison of (A) 1-year survival and (B) intermediate-term survival according to recipient age.

Use of induction and maintenance immunosuppression did not differ among age groups. Supplementary Figure 11 describes the percentage of recipients experiencing rejection between transplant discharge and 1-year follow-up based on the type of immunosuppression maintenance according to recipient age, and tacrolimus was favored over cyclosporine in all age groups. MMF was maintained in over 80% of patients in all age groups, while everolimus was consistently maintained in one third of patients in all age groups (data not shown). The percentage of rejection or proportion of treated rejection did not differ according to age group. Although the figure shows more events of rejection in tacrolimus group when compared to cyclosporine group, when other variables (age, recipient/donor gender, and number of human leukocyte antigen mismatch) were considered, type of immunosuppression (tacrolimus based vs. cyclosporine based) was not a significant factor of rejection event between transplant discharge and 1-year follow up. Post-transplant comorbidities did not differ significantly among the different age groups (Table 3). Supplementary Figure 12 shows immunosuppression maintenance at 1-year follow up by year, which did not differ significantly.
Table 3
Post-transplant comorbidities at the 1-year follow-up visit

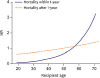
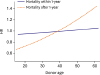
Donor and recipient age and recipient survival
Figures 4 and 5 show hazard ratios for conditional mortality within and after 1-year post-HTx by recipient and donor age groups. The effect of recipient age was more pronounced in short-term mortality (mortality within 1-year post-HTx) (Figure 4), while the effect of donor age was more prominent for conditional mortality after 1-year post-HTx (Figure 5).
DISCUSSION
This second biannual report based on KOTRY registry data detailed trends regarding donor and recipient characteristics, post-transplant comorbidities and outcomes. We also focused on age in relationship to pre and post-transplant characteristics and outcomes. Since the initial report of the KOTRY registry was published, some distinct trends in HTx were noted despite the short-term follow-up duration. First, usage of mechanical support devices before transplant has significantly increased. Significantly more patients are on ECMO and ventilators in recent years compared to 2014–2015, indicating that more patients are getting transplanted when they are severely ill, most likely due to organ shortages. Second, in terms of age, the mean donor age increased significantly in the most recent year compared to 2014–2015, while the mean recipient age was unchanged.
The number of patients bridged with ECMO before HTx has increased in recent years. Both short- and intermediate-term survival was worse in pre-transplant ECMO-supported patients compared to those without pre-transplant ECMO. Further, patients with ECMO and ventilator support before transplant did far worse than those with pre-transplant ECMO without a ventilator. Previous data from the United Network of Organ Sharing thoracic registry reported post-transplant survival in patients who were bridged with ECMO to be 73% at 3 months and 67% at 3 years.6) Corresponding survival rates from the KOTRY registry were 85% at 3 months and 77% at 3 years. The current standard treatments for bridging to transplant before HTx in the United States include durable ventricular assisting devices that yield better survival rates than ECMO.3) Durable ventricular assisting devices are still not affordable for most patients in Korea, and so very few (n=5, 1%) had a ventricular assisting device as a bridge to transplant in the KOTRY data. This is a unique and distinct characteristic of current HTx practice in Korea compared to other countries where the use of ECMO as a direct bridge to transplantation in adults is very infrequent; the most recent International Society for Heart and Lung Transplant (ISHLT) registry reported that 1% of cases used ECMO as a bridge to transplant.7) Relatively better survival in patients who were bridged with ECMO in the KOTRY data compared to other studies may result from a recent pre-emptive ECMO strategy, where patients undergo ECMO insertion electively rather than in an emergent setting. However, pre-transplant ECMO was still significantly associated with worse early and long-term survival outcomes in the KOTRY data. Unlike a durable ventricle assisting device, which allows patients to maintain a functional status, patients on ECMO support are immobilized in intensive care units with invasive monitoring and exposed to complications related to the ECMO and intensive care unit environment. Due to a shortage of organs and unaffordable durable ventricular supporting devices, more patients were bridged with ECMO before HTx. The major concern for the current practice in Korea includes poor post-transplant survival by preferentially allocating hearts to ECMO-supported patients.
We focused on age in this second official KOTRY HTx report. With the development of mechanical devices to bridge to HTx and the increasing prevalence of heart failure among the elderly, the number of potential HTx candidates of advanced age is increasing. With organ shortages, age is an important issue for recipient and donor selection. The ISHLT guideline was modified in 2016 to address issues of HTx in patients with advanced age.8) Previous studies have consistently reported comparable long-term survival outcome in patients with advanced age,9)10)11) and so the class IIb recommendation accommodated consideration of patients older than 70 years for HTx after careful selection.8) According to the 30th report from ISHLT, the proportion of recipients with age ≥70 in the 2006–2012 era was 1.3%. From the KOTRY data covering 2014–2017, the proportion of recipients age ≥70 who underwent HTx rose slightly to 2.8% (n=11).12)
The majority of HTxs in recipients of advanced age (≥65) are performed in North America, and reports from high volume centers in North America show comparable long-term survival rates in recipients of advanced age (10-year survival for age ≥70, 60–69 years, ≤60 years was 51.7%, 47.7%, and 57.1%, respectively).13) In contrast, the 30th ISHLT report showed worse survival with increasing recipient age.12) Despite conflicting results, the current consensus is that age older than 70 years alone should not be an exclusion criterion for HTx. According to single center data reporting favorable outcome following HTx in patients older than 70, the age group of ≥70 had less comorbidities compared to transplant recipients in their 60s, suggesting that a stringent selection process is important for favorable outcomes in patients of advanced age. The KOTRY data analyzed according to year revealed that the proportion of HTx recipients age ≥70 has recently declined (n=6, 3% in 2014–2015; n=4, 4% in 2016; and n=1, 1% in 2017). This trend reflects the current practice of thorough patient selection in advanced age patients as HTx candidates in Korea. Newly emerged alternative treatment choices, such as LVADs for destination therapy, may also have contributed to this trend.
Due to the relatively short follow-up duration, no differences in post-transplant comorbidities or causes of death among different age groups were noted in the KOTRY data, although previous studies suggest that post-transplant comorbidities and causes of death differ according to recipient age. In ISHLT data, death from graft failure, including coronary allograft vasculopathy and acute rejection, decreased with increasing age, while death related to multiple organ failure, infection and non-lymphoma malignancy increased.8) Declining immuno-competency with aging is known to potentially lower rejection rates due to lower generation of new T and B lymphocytes, which also contributes to increasing comorbidities associated with cancer and infection.14)15) Different immuno-competency with aging raises questions about whether post-transplant screening and management for rejection or comorbidities should differ according to age group, yet data remain insufficient to answer these questions.
Clearly, donor age increased in Korea from 2014 to 2017, over a relatively short period of time. Previous data from ISHLT also describe the same trends of increasing donor age.8) The median donor age in the KOTRY registry was 42, which was similar to the donor age in Europe (median age of 43), and older than that in North America (median age of 29). Increasing demand for donor organs has inevitably expanded the donor pool to include so-called marginal donors. A previous retrospective study analyzing outcome of 228 HTxs suggested that having a marginal donor (>50 years) did not affect 1,3, or 5 year mortality if associated with a short ischemic time, however, patients with older donors presented with more frequent coronary allograft vasculopathy.16) The increasing incidence of coronary allograft vasculopathy with increasing donor age might be explained by age-related endothelial dysfunction and age correlated increases in the incidence of pre-existing coronary artery disease of donor hearts.17) Data from the 30th report from ISHLT showed that increasing donor age was associated with worse survival, particularly with donors aged ≥60. Although younger donor age was accepted as an important prognostic factor for favorable long-term outcome after HTx, it remains worthwhile to consider accepting marginal donors, because the survival of patients who receive a transplant from a selected marginal donor might still be better than for those who were not transplanted at all.16) Consequently, there is increasing acceptance for marginal donors with careful selection, such as short ischemic time, and this trend was reflected in the KOTRY data.
In conclusions, KOTRY, the nationwide organ transplantation database supported by the Korean government, was established in an effort to provide evidence for a national organ transplant policy. Using KOTRY data, this report provided a comprehensive analysis of current transplantation data in Korea. Over 4 years, with increasing organ shortages, centers were more willing to accept older age donors, and more patients received transplants under ECMO care. Increasing age was a strong independent factor for intermediate long-term survival, but post-transplant comorbidities did not differ among age groups, possibly due to the relatively short-term follow-up period. Further study with longer follow-up duration is needed to better understand age-related post-transplant prognosis.
 XML Download
XML Download