

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Diffuse long coronary artery lesions consist of approximately 20% of all percutaneous coronary intervention (PCI) and represent a therapeutic challenge, as these often require implantation of multiple stents which have been associated with poor clinical outcomes including increased risk of stent thrombosis and restenosis.1)2) However, the evolution of coronary stent technology including newer antiproliferative drugs, thinner and flexible stent architecture, and more biocompatible polymer with improved elution dynamics might provide a better clinical outcome in patients with diffuse long lesions.
In a current issue, Park et al.3) investigated the efficacy and safety of the Resolute™ zotarolimus-eluting stent (R-ZES; Medtronic Inc., Santa Rosa, CA, USA) in patients with diffuse long coronary lesions ≥25 mm from a prospective, relatively large-scale and real-world registry. Current analysis showed the incidence of major adverse cardiac events (MACE, the composite of cardiac death, non-fatal myocardial infarction, and clinically-driven target vessel revascularization) and definite stent thrombosis at 1 year were 3.0% and 0.3% respectively. In subgroups analysis, multiple overlapping stents implantation is significantly associated with high rates of MACE compared with single stent implantation (7.1% vs. 1.5%, respectively, p<0.001).
R-ZES uses a cobalt chromium platform with a continuous sinusoidal design to further enhance the flexibility and deliverability in the complex lesion. A BioLink™ durable polymer is adapted to allow a slower drug elution and provide good biocompatibility. The RESOLUTE all-comers trial comparing R-ZES with everolimus-eluting stent (EES) demonstrated similar safety and efficacy for the R-ZES and EES through 4-year follow-up.4) In addition, there were comparable clinical outcomes between R-ZES and EES in patients with very long (>30 mm) coronary artery stenosis.5)
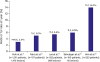
Traditionally, lesion and stent length have been known as an important predictor of in-stent restenosis or adverse events, especially for bare-metal stent from the early stage of coronary intervention. Concern over high doses of the anti-proliferative drug, overlapping stent layer and extensive vascular injury were associated with higher rates of restenosis and very late stent thrombosis. However, the impact of lesion length on clinical outcomes could be different in the bare-metal stent and drug-eluting stent (DES), especially second-generation.6) Although Park et al.'s study3) is not a randomized or comparative study, the clinical result of R-ZES for diffuse long coronary lesions is comparable to those in previous studies (Figure 1).5)7)8)9) Thus, PCI with R-ZES appears to be safe and effective in Korean patients with diffuse long coronary artery disease.
However, there is a significant increase of MACE rate (7.1% vs. 1.5%, p<0.001) in multiple overlapping stenting (13.8% of the study group) than in single stenting (86.2% of the study group) for long coronary lesions in this study.3) Overlapping stents are a potential source of neointimal hyperplasia due to the physical double layer of stent struts. A short gap can be inadvertently lapsed out between multiple stents, which increases the risk of restenosis and stent thrombosis. Compared to the current study, LONG Native Coronary Lesions With Drug-Eluting Stent-IV (LONG-DES IV) trial9) showed higher target lesion failure rate (14%) of R-ZES at 1-year follow-up which may be derived more implantation of multiple stents (52.8%, more than 2 stents) and longer length of stents used (45.9±17.1 mm) than those in the current study (implantation of multiple stents, 13.8%, mean stent length, 28.27±6.97 mm, respectively).3)
Therefore, implantation of the second-generation DES is a reasonable strategy in diffuse long coronary lesions which can be covered by a single long stent. However, in case of very long coronary lesions which cannot be covered by single long stent and need for multiple overlapping stents, MACE rate is still high3)9) and further investigations for better angiographic and clinical outcome are needed. Regarding this topic, IVUS-guided optimal implantation strategy reduced MACE rate than in angiography-guided implantation, mainly derived by the reduction of ischemia-driven target lesion revascularization, in diffuse long lesions.10)
Taken together, the implantation of the second-generation DES such as R-ZES in diffuse long coronary lesions is the optimal strategy in real clinical practice. In very long coronary lesions, avoidance of overlapping stents, use of IVUS may improve clinical outcome. Still, we have a long way to go in very long coronary artery lesions.
 XML Download
XML Download