

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Various diseases associated with the biliary system, including extrahepatic biliary duct obstruction (EHBO) due to stones, tumors, pancreatitis, inflammation, mucocele, perforation, and rarely avulsion of the bile duct, can induce vague clinical signs and result in nonspecific laboratory results [1234].
Ultrasonography is the most commonly used technique for investigating the biliary tract in animals, but ultrasonographic images are influenced by intraluminal gas, food remnants in the intestine, depth of structure, and lesions related to adjacent organs. In cases with ascites and bile peritonitis induced by bile duct perforation or avulsion, it is difficult to localize the exact site of lesions in ultrasonography [56].
Availability of computed tomography (CT) is increasing in veterinary medicine. CT can be used to evaluate both gallbladder and bile ducts, particularly on pre- and post-contrast CT images. A dilated bile duct is one of the common findings of EHBO. However, bile duct dilation is not a pathognomonic finding for EHBO diagnosis, and it can be encountered in asymptomatic dogs in practice [7]. Conversely, bile congestion can occur even without evidence of gallbladder and bile duct dilation in some dogs with jaundice [7]. Therefore, not just bile duct dilation but bile duct patency needs to be evaluated for diagnosing EHBO.
Indirect CT cholangiography is invasive and uses biliary-specific contrast agents for imaging the biliary tract [8]. However, in patients with biliary obstruction, hepatocellular disease, and others, hepatic concentrations of the contrast agent can be insufficient to visualize the biliary system clearly because the contrast agents are absorbed by hepatocytes and excreted through the bile duct into the intestines [9]. Therefore, indirect CT cholangiography has little diagnostic value for differentiating between hepatic and post-hepatic jaundice. Ultrasound contrast agent (SonoVue) has been percutaneously injected into the gallbladder to assess the patency of the common bile duct by observing the microbubbles from the duodenal papilla in dogs [9]. This procedure required simultaneous scanning of the gallbladder for contrast injection and the duodenum for microbubbles and used two ultrasound machines. Ultrasonographic evaluation of the microbubbles could be interrupted by various artifacts related to food in the duodenum. Endoscopic retrograde cholangiopancreatography (ERCP) provides excellent delineation of ductal structure with high spatial resolution [7101112]. ERCP has been applied to healthy dogs and dogs with chronic gastrointestinal problems [71213]. However, the success rate of ERCP is influenced by the experience of the investigator and the size of the dog [131415]. Moreover, ERCP can cause complications including pancreatitis, bleeding, perforations, and infections which can lead to 6.85% mortality and morbidity rates in patients undergoing ERCP [13]. Thus, even in humans, CT transhepatic cholangiography is now used for accessing the biliary tree in cases where ERCP is unsuccessful or for anatomic evaluation of complications.
Transhepatic cholecystography is a radiographic contrast technique in which the biliary tract is examined after direct injection of an iodinated contrast agent into the gallbladder with ultrasound, fluoroscopy, or peritoneoscopy guidance [3161718]. This technique allows the assessment of the biliary tract by direct detailed visualization of the gallbladder and bile duct and has high sensitivity and specificity for diagnosing biliary obstruction [34161718]. However, transhepatic cholecystography has not been widely used in practice because it is invasive and can lead to complications such as bile peritonitis, gallbladder rupture, or hepatic hemorrhage. In addition, it can be difficult to evaluate the structure of the biliary tract using this method because of bile tract summation on radiographs [318]. Most of those risks are similar for CT transhepatic cholangiography, but CT allows tomographic imaging and reconstruction. This study was performed with the hypothesis that CT transhepatic cholecystography can detect the biliary tract without summation of bile tracts, and can be used to evaluate tract structure and patency. The purpose of this study was to investigate the feasibility of CT transhepatic cholecystography and to optimize the use of this technique in dogs.
MATERIALS AND METHODS
Animals
In this crossover study design, 8 intact male, purpose-bred beagles (3–5 years old), weighing 9–11 kg, were used. All dogs were clinically healthy based on systemic arterial blood pressure, physical examination, complete blood count, serum biochemistry, and abdominal radiography and ultrasound results. Dogs were cared for in accordance with the Laboratory Animal Research Center Guide for Care and Use, and the experimental protocol was approved by the Institutional Animal Care and Use Committee at Chonnam National University (CNU IA-YB-R-2017-09).
CT cholecystography
After food deprivation for 12–18 h, general anesthesia was induced by intravenous injection of a combination of 0.03 mg/kg of medetomidine hydrochloride (Domitor; Orion Corp., Finland) and 1.5 mg/kg of zolazepam hydrochloride–tiletamine hydrochloride (Zoletil; Virbac, France), and maintained with isoflurane (Terrell; Piramal Critical Care, USA). After placing the dog in the sternal recumbency position on the CT table, pre-contrast CT scanning was performed using a 16-row multidetector CT scanner (Somatom Emotion; Siemens Medical Systems, Germany) with a setting of 16 rows × 0.5-mm collimation, helical pitch of 0.8, rotation duration of 600 msec, 1 mm slice thickness, tube voltage of 130 kV, and tube current of 120 effective mA. Then, without changing the position of the dog, transhepatic cholangiography was performed by one examiner (KDE). Under ultrasonography (ProSound Alpha 7; Hitachi-Aloka, Japan), a 22-gauge catheter (Angiocath Plus; Becton Dickinson Infusion Therapy Systems Inc, Singapore) was percutaneously passed into the gallbladder through a subcostal or intercostal approach depending on the need to provide a proper window of the gallbladder each time. The catheter was connected to a 3-way stopcock and as much bile juice was aspirated from the gallbladder as possible. Then, the iodinated contrast medium, iohexol (Omnipaque 300; GE Healthcare, Norway), was slowly injected into the gallbladder over 60 sec through the 3-way stopcock. Transhepatic cholecystography was performed in dogs with maintenance of spontaneous breathing. Post-contrast CT scanning was performed at 3, 10, and 30 min after injection of the contrast medium into the gallbladder using the same protocol as that for pre-contrast CT scanning. All CT images of the pre-contrast and CT cholangiography were reconstructed into 1 mm increments with an 0.8 pitch. In each dog, CT cholecystography was conducted four times at a minimum of one-week intervals using four different contrast formulas; 8 mL and 16 mL of total contrast medium volumes and 1:1 and 1:3 dilution ratios between iohexol and saline. During or after the procedure, the dog was treated or considered removed from the experiment if the dog exhibited depression, abdominal discomfort, restless, or pain. After each CT cholecystography, the dog was given an intravenous injection of 2 mg/kg tramadol (Tamadol; Dongkwang Pham, Korea) and 20 mg/kg cefazolin (Cefozol; Hankook Korus Pharm, Korea) for 3 days. Complications related to cholecystography were monitored based on clinical signs such as abdominal pain, vomiting, anorexia, and depression and on complete blood count results. Ultrasonography for bile leakage or rupture of the gall bladder, peritonitis, hemorrhage, and others was conducted at 1 week after cholangiography by one examiner (KDE).
CT cholecystography images evaluation
In all post-contrast series of CT scans, 2-dimensional (2D) or 3-dimensional (3D) reconstructions of the biliary tract were created using curvilinear planar reconstruction (CPR), maximum intensity projection (MIP), shaded surface display (SSD), and volume rendering technique (VRT). CT images were transferred to a workstation (Infinitt PACS; Infinitt Healthcare, Korea) and blind assessment of each CT image set was performed by two examiners (KDE, PSJ), separately.
For qualitative evaluations, filling of the gallbladder, visibility of the biliary tract, and the quality of CT images including artifacts were assessed (Table 1). Contrast medium in the lumen of the duodenum was evaluated based on the absence or presence of contrast medium and used to assess bile duct patency. Distinction of the gallbladder and cystic duct and distinction of the common bile duct and duodenum were evaluated based on whether the cystic duct or common bile duct could be identified separately from the gallbladder or from the duodenum. The distinction of these two bile ducts was evaluated to assess sufficient filling of the biliary system with contrast medium. For quantitative evaluations, the volume of the gallbladder, and diameters of the cystic duct and common bile duct were measured. Regions of interest were drawn over the gallbladder in each transverse CT image by setting the threshold between 400 and 2000 Hounsfield units. The volume of the gallbladder was measured by using CT volume measuring software (Somatom Emotion; Siemens Medical Systems, USA). The diameter of the cystic duct was measured as the widest short axis of the cystic duct, perpendicular to the bile duct wall, at the junction of the bile duct and gallbladder (Fig. 1). The diameter of the common bile duct was measured at the duodenal papilla region where the region of the duodenal-common bile duct was observed after finding the maximal diameter of the common bile duct by using paddle-wheel reconstruction.
Table 1
Qualitative analysis of CT cholangiography evaluation factors

![]()
 | Fig. 1Quantitative measurement of the volume of the gallbladder and diameter of the bile duct in a dog with 16 mL of 1:3 diluted contrast formula. (A) On transverse CT images, a region of interest (dashed curve) was drawn over the gallbladder and the volume of the gallbladder was measured using CT volume measuring software with a threshold setting between 400 and 2000 Hounsfield units. (B) Diameter of the cystic duct was measured as the widest short axis of the cystic duct (arrow), perpendicular to the bile duct wall, at the junction of the bile duct and gallbladder. (C) The maximal diameter (arrow) of the common bile duct was measured at the duodenal papilla region (arrowhead) using paddle-wheel reconstruction.CT, computed tomography.
|
Statistical analysis
Differences in quantitative and qualitative evaluation factors were investigated by performing repeated measures analysis of variance (ANOVA). The p values less than or equal to 0.05 were considered significant. Analysis of reproducibility between reviewers was performed by using an intra-class correlation coefficient test. All statistical tests were performed with SPSS statistical software for Windows (Release 23.0; standard version; SPSS Inc., USA).
RESULTS
A total of 32 sets of CT cholecystography images were obtained from the 8 beagles with four contrast formulas. Both 2D- and 3D-reconstructed CT images using CPR, MIP, SSD, and VRT were obtained for each CT image set. CT cholecystography was performed reliably under ultrasound-guidance. Mild bile leakage was observed in 10 CT image sets obtained at 3 min after transhepatic cholangiography; however, no associated clinical signs nor changes in complete blood count were observed in any dog.
CT cholangiography was evaluated according to the contrast formula that was used and the time of CT acquisition (Tables 2 and 3). The volume and dilution ratio of the contrast agent significantly affected the filling of the gallbladder (p = 0.034) and the quality of CT images and artifacts (p = 0.02). It also influenced the absence or presence of contrast medium in the lumen of the duodenum (p = 0.018), distinction of common bile duct and duodenum (p = 0.03), and the volume of the gallbladder (p = 0.005). However, CT cholecystography features did not significantly differ according to the time of acquisition, except for the diameters of the cystic duct (Fig. 2).
Table 2
Qualitative assessment of evaluation factor scores for CT transhepatic cholangiography using different volumes and dilution ratios of the contrast agent, as well as different CT scan times in 8 normal Beagle dogs
Data are expressed as mean ± standard deviation of the score.
CT, computed tomography; GB, gallbladder; CD, cystic duct; CBD, common bile duct.
![]()
Table 3
Quantitative evaluation of CT transhepatic cholangiography using different volumes and dilution ratios of the contrast agent and different CT scan timing in 8 normal Beagles
Data were expressed as mean ± standard deviation.
CT, computed tomography; GB, gallbladder; CD, cystic duct; CBD, common bile duct.
![]()
 | Fig. 2Reconstructed shaded surface display computed tomography images after transhepatic cholangiography using 16 mL volume and 1:1 dilution ratio of contrast medium in a dog. There were no significant differences in opacification between the gallbladder and common bile duct according to scan time; at 3 min (A), 10 min (B), and 30 min (C). Long arrow = cystic duct, thick long arrow = extrahepatic duct, short arrow = intrahepatic bile duct. Left side of the image is the right side of the dog.
|
Compared to the 8 mL volume of the contrast agent, the evaluation factors including volume of gallbladder (p = 0.021), diameters of cystic (p = 0.035) and common bile ducts (p = 0.026), filling of gallbladder (p = 0.021), visibility of biliary tract (p = 0.046), and distinction of common bile duct and duodenum (p = 0.045) were significantly greater when the contrast agent volume was 16 mL, regardless of scan time or contrast dilution ratio. The gallbladder and biliary tract appeared larger and were well visualized when the contrast agent volume was 16 mL (Fig. 3).
 | Fig. 3Reformatted shaded surface display computed tomography images after transhepatic cholangiography with 1:3 dilution ratio and 8 mL (A) or 16 mL (B) of contrast volume in the same dog. The gallbladder and bile ducts are well visualized with 16 mL of contrast medium. Left side of the image is the right side of the dog.
|
Significant differences were identified in the quality of CT images and artifacts at all scan times and contrast volumes (p = 0.01) between the different contrast medium dilution ratios. When the dilution ratio of the contrast medium was 1:1, beam-hardening artifacts deteriorated the CT image quality; thus, the 1:3 dilution ratio was deemed optimal for achieving acceptable CT images (Fig. 4).
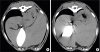 | Fig. 4Transverse computed tomography image after transhepatic cholangiography with 8 mL contrast volume and 1:3 (A) or 1:1 (B) dilution ratios in the same dog. Dark streaks induced by beam hardening artifact are observed in the image using a 1:1 dilution ratio. Left side of the image is the right side of the dog.
|
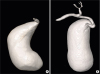
In comparison to transverse CT scan images, CPR could assess the biliary tract intuitively with one image by its ability to reconstruct the bile duct linearly in all dogs and using a 16-mL contrast volume (Fig. 5). MIP reconstructions helped to visualize the biliary tract and provided a sharp contrast to surrounding structures. SSD provided a realistic-looking 3D view of the surface of the biliary structure of interest. VRT facilitated, not only assessment of the anatomical biliary structure, but also evaluation of the anatomic relationship between the biliary system and the surrounding organs.
 | Fig. 5Reconstructed computed tomography transhepatic cholangiography images. (A) The entire biliary duct from the cystic duct to the orifice to the duodenum (arrow) is clearly visualized on a curvilinear planar reconstruction image. (B) On a maximum intensity projection, enhanced gallbladder and bile duct are differentiated from the liver in detail and the lumen of the bile duct is well visualized at the extremities. (C) Outlining of the gallbladder and bile duct are shown on a shaded surface display. However, the internal structure is not delineated. (D) On volume rendering, the three-dimensional relationship between the biliary system and adjacent organs is clearly defined. Left side of the image is the right side of the dog.
|
With regards to inter-observer agreement, there was an excellent, statistically significant agreement between the examiners (KDE, PSJ) for all evaluation factors except one for which the agreement was considered good (Table 4).
Table 4
Inter-observer correlation coefficients for evaluation factor scores provided by two examiners

Data between 0.61 to 0.79, and greater than 0.9 are indicative of good, and excellent reliability, respectively, based on 95% confidence intervals.
GB, gallbladder; CT, computed tomography; CD, cystic duct; CBD, common bile duct.
![]()
DISCUSSION
The feasibility of CT transhepatic cholecystography in dogs was evaluated in this study. The approach provided detailed cross-sectional, reconstruction, and 3D images of the gallbladder, cystic duct, and common bile duct. These structures could be distinguished from the liver parenchyma, adjacent vessels, duodenal lumen, and pancreas. Comprehensive visualization of the anatomic relationship between the biliary system and adjacent structures was improved by using the 3D reformatted CT transhepatic cholangiography images. The 16 mL contrast medium volume and the 1:3 dilution ratio of contrast medium and saline provided optimal quality images of CT transhepatic cholangiography. CT image acquisition timing was not a significant parameter for evaluating the biliary system via CT transhepatic cholecystography.
In CT transhepatic cholecystography, the lumen of the bile duct can be observed distinctly due to the homogeneous filling by the contrast agent. The diameter of the common bile duct was consistently measured as approximately 3.36 mm at the duodenal papilla. After linear reconstruction of the bile duct by CPR, the patency of the biliary tract range to the orifice of the bile duct could be clearly evaluated. The distinction between the gallbladder and cystic duct and between the common bile duct and duodenum could be visualized, especially via paddle-wheel reconstruction. MIP allowed for easy evaluation of the biliary lumen and tributaries and also the relationship between the contrast-filled structures and the densities of other surrounding structures. Thus, MIP is used in cases of stenosis and choledocholithiasis in humans [192021]. SSD provided a realistic 3D image of the surface of the biliary structure while obscuring intraluminal structures. SSD is suitable for intuitively outlining the gallbladder and bile duct [4192022]. VRT provided the 3D anatomic relationship between the biliary system and adjacent structures. In human study, VRT allows for overall assessment of patients with biliary obstruction by depicting the biliary tree, vessels, and adjacent organs such as the liver, pancreas, and duodenum, which cannot be clarified with conventional cholangiography or even in some cases that underwent endoscopic retrograde cholangiography (ERCP) [81523].
The volume and dilution ratio of the contrast agent and the scan time of CT transhepatic cholecystography were investigated in this study because the protocol for transhepatic cholecystography has not been established, even in radiographic studies. The gallbladder can accommodate a volume of approximately 1 mL/kg of body weight [24]. The volume of contrast agent was set at 8 mL and 16 mL after considering the mean weight of dogs used in this study, which was about 10 kg. Sufficient filling of the gallbladder and the entire biliary tract could be achieved using 16 mL of contrast agent when evaluated based on volume of the gallbladder, and diameters of the cystic and common bile duct. In addition, the common bile duct was more distinctly identified from the duodenum using this volume. A diluted contrast agent was used during cholecystography in this study to reduce artifacts associated with high-density contrast agents in order to improve image quality. A dilution ratio of 1:3 provided better CT transhepatic cholecystography imagery compared to that from a 1:1 ratio with minimal artifact presence. Contrary to indirect CT cholangiography, which requires about 30 to 60 min to provide optimal CT images after metabolizing oral contrast agent in the liver [8], in this study, the gallbladder and bile duct were effectively filled with contrast agent immediately after direct injection into the gallbladder. The degree of filling of the gallbladder and bile duct was not significantly changed according to CT scan time, although there was some difference in the degree of filling of the biliary tract in each dog. Gallbladder distensibility, the resistance of the sphincter of Oddi, and the volume of the bile duct in the gallbladder can induce individual differences in dogs [18].
Similar to radiographic cholecystography, in CT transhepatic cholecystography bile leakage can occur after direct contrast injection. Bile leakage was reported in about 10% of human patients in a radiographic cholecystography study [2]. In the present study, about 30% of all CT transhepatic cholecystography episodes showed bile leakage; however, leakage-related clinical signs were not detected in any dog. The resolution of CT transhepatic cholecystography is higher than that of radiography; thus subclinical bile leakage can be detected [23].
In the present study, only two volumes of contrast agent, 8 mL and 16 mL, were compared in order to establish a protocol for CT transhepatic cholecystography and only healthy dogs of the same breed were used. Despite those limitations, this study investigated the effects of volume and dilution ratio of the contrast agent, as well as CT scan time, on CT transhepatic cholecystography results. The clinical usefulness of this method was confirmed by the results of the comprehensive evaluation.
In conclusion, ultrasound-guided CT transhepatic cholecystography was effectively and safely used to examine the gallbladder and bile duct in dogs, and various reconstruction techniques employed in this study improved the anatomic elucidation of the biliary system. A total volume of 16 mL of contrast agent with a 1:3 contrast medium dilution ratio was optimal for visualizing the gallbladder and biliary tract with minimal artifact development. Although percutaneous CT cholecystography is not the first choice among diagnostic tools for patients with biliary disease, it is considered a useful diagnostic imaging method for identifying obstructions in the biliary tree, determining patency of the duct, and differentiating surgical candidates from medically treatable cases in dogs with jaundice.
 XML Download
XML Download