

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In healthy subjects, the heart rate (HR) falls rapidly after cessation of exercise as the parasympathetic tone is enhanced and catecholamine level drops, whereas the heart rate recovery (HRR) after exercise in patients with impaired parasympathetic nervous systems, such as heart failure1) or ischemic heart disease,2) shows a marked attenuation of this drop.1)
Arterial stiffness is increased in hypertension,3) but it can be also observed in pre-hypertensive patients.4) Pulse wave velocity (PWV) is considered the gold standard method for estimation of arterial stiffness.5) The carotid arterial stiffness index (CSI) is another well-known parameter of arterial stiffness that can be used directly and non-invasively to measure the elastic property of the arterial wall.6)7)8)
Several experimental studies have demonstrated that atherosclerosis reduces baroreceptor sensitivity,9)10)11) which contributes to impairments in the parasympathetic nervous system.12) However, clinical evidence has been scarce as to whether the degree of autonomic modulation is related to arterial stiffness and a blunted vasoactive response following exercise, even in prehypertensive patients with an early atherosclerotic stage. Therefore, we investigated whether impaired vagal activity as demonstrated by slow HRR after symptom-limited treadmill exercise was associated with increased arterial stiffness, as assessed by PWV and CSI at rest, and a blunted vasoactive response following exercise, as assessed by CSI after exercise in normotensive patients without overt atherosclerosis.
METHODS
Study population
A total of 162 consecutively normotensive patients without overt atherosclerosis who underwent treadmill stress echocardiography (TSE) between June 2013 and April 2014 at one cardiology center (Kyung Hee University Hospital at Gangdong, Seoul, Korea) with typical or atypical chest pain or dyspnea and electrocardiographic abnormalities was screened. Patients also underwent brachial-ankle PWV (baPWV) measurements at rest and ultrasonographic examination of their carotid arteries at rest and after exercise. Among these 162 patients, eight demonstrated significant coronary artery disease and were excluded from this study. The remaining 154 patients were ultimately enrolled. Patients who met the following criteria were also excluded: younger than 20 years of age; past medical history of hypertension; previously documented coronary artery disease; non-sinus rhythm, such as atrial fibrillation; valvular heart disease greater than moderate grade; left ventricular ejection fraction less than 50%; systemic diseases, including chronic obstructive pulmonary disease, renal failure, and hepatic failure; suspicious peripheral artery disease with clinical symptoms; ankle brachial index less than 0.9; and overt atherosclerosis with carotid plaque ≥ 1.5 mm. All patients provided written informed consent before undergoing TSE. This study was approved by the hospital ethics committee (KHNMC IRB 2013-01-114).
BaPWV
BaPWV (VaSera VS-1000, Fukuda Denshi Co., Tokyo, Japan) was performed before TSE according to the manufacturer's recommendation. Patients were examined in the supine position. Four pressure waveforms from blood pressure (BP) cuffs that were wrapped around both arms and ankles and connected to a plethysmographic sensor and an amorphous sensor were stored for 10 seconds. Phonogram, BP, and HR were also simultaneously recorded. BaPWV was calculated by measuring the time for the pulse wave to travel between the brachial and posterior tibial arteries. The mean value of the right-sided and left-sided baPWVs was used for this analysis. All measurements were performed by experienced operators who were blinded to patient information.
TSE and ultrasonographic examination of the carotid arteries
Symptom-limited treadmill exercise was carried out according to the standard Bruce protocol.13) After cessation of exercise, patients were moved to the left decubitus position for an assessment of wall motion abnormalities. BP and HR were measured before exercise, at the end of each stage, and at 1 min after exercise. The target HR was calculated as 220 – age. HRR was defined as the difference between HR just before termination of exercise (peak HR) and HR at 1 minute after exercise.
CSIs were measured before exercise (CSI at rest) and within 5 minutes after exercise (CSI after exercise) on both common carotid arteries using high resolution B-mode ultrasound (iE33 Ultrasound with Linear Array Transducer, Philips, San Jose, CA, USA) in the supine position. Systolic and diastolic carotid luminal diameters were measured on the longitudinal carotid arterial image as the maximal and minimal carotid diameters during the cardiac cycle (Figure 1). Systolic and diastolic BPs were simultaneously measured using cuff sphygmomanometry of the brachial artery (Tango, SunTech Medical, Morrisville, NC, USA) during the ultrasound measurements. CSI was calculated as the ratio of the natural logarithm of (systolic BP/diastolic BP)/[(systolic carotid arterial diameter - diastolic carotid arterial diameter)/diastolic carotid arterial diameter] (Figure 1). The mean value of the right-sided and left-sided CSIs was used for this analysis. TSE and ultrasonographic examination of the carotid arteries were performed by one experienced operator who was blinded to all patient data to exclude inter-observer variability.

Statistical analysis
Statistical analyses were performed using SPSS for Windows, version 13.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as the mean ± standard deviation. Categorical variables were expressed as group percentage. Pearson's correlation was utilized to demonstrate the correlations between indices of arterial stiffness and HRR. Simple and multiple regressions analyses to assess the relationships between indices of arterial stiffness and HRR were performed. The intra-observer variability for values of CSI at rest on Bland-Altman analysis was tested in 10 patients, and the coefficient of variability was 3.9%.14) Statistical significance was considered at a p value less than 0.05.
RESULTS
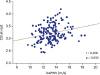
Baseline clinical characteristics, variables of the treadmill stress test, and arterial stiffness indices of the study population are described in Table 1. Table 2 shows univariate regression analyses between HRR and clinical variables. Slow HRR was correlated with patients who were aging, tended to be male (t-test, male: female = 41 ± 11 beats/min: 37 ± 11 beats/min, p = 0.024), and had diabetes (t-test, non-diabetes: diabetes = 40 ± 11 beats/min: 33 ± 12 beats/min, p = 0.008), higher resting and peak systolic BP, higher resting HR, lower peak HR, lower metabolic equivalents, increased baPWV, and increased CSIs at rest and after exercise. HRR had moderate correlation to baPWV (r = −0.331, p < 0.001) and CSI after exercise (r = −0.334, p < 0.001) and a weak correlation to CSI at rest (r = −0.269, p = 0.001) (Figure 2). No relationships were found between HRR and baseline laboratory findings, such as cholesterol, triglycerides, and high- and low-density lipoprotein cholesterol (data not shown). HRR was inversely associated with baPWV and CSI after exercise after adjusting for established cardiovascular risk factors of age, sex, body mass index, diabetes, and current smoking but was not associated with CSI at rest (Table 3, Model 1). HRR was also associated with CSI after exercise after adjusting for model 1 + resting systolic BP and metabolic equivalent of tasks but was not associated with baPWV or CSI at rest (Table 3, Model 2). BaPWV had a weak correlation with CSI at rest (r = 0.250, p = 0.002, Figure 3). CSI after exercise had positive correlation with baPWV (r = 0.363, p < 0.001) and CSI at rest (r = 0.514, p < 0.001) (Figure 4).
Table 1
Clinical characteristics and variables associated with the treadmill stress test and arterial stiffness indices of the study population

Table 2
Univariate analysis of associated variables for HRR

baPWV: brachial-ankle pulse wave velocity, β: unstandardized coefficients, BMI: body mass index, CSI: carotid arterial stiffness index, DBP: diastolic blood pressure, HR: heart rate, HRR: heart rate recovery, MET: metabolic equivalent of tasks, SBP: systolic blood pressure, SE: standardized error, Stβ: standardized coefficients.
Figure 2
Scatter plots describing the correlations of HRR with baPWV (left panel) and CSI at rest (middle panel) and after exercise (right panel). baPWV: brachial ankle pulse wave velocity, CSI: carotid arterial stiffness index, HRR: heart rate recovery.

Table 3
Associations of HRR with atherosclerotic markers after adjusting for confounding variables: multivariate linear analyses
baPWV: brachial-ankle pulse wave velocity, β: unstandardized coefficients, CSI: carotid arterial stiffness index, HRR: heart rate recovery, SE: standardized error, Stβ: standardized coefficients.
*Adjusting for established cardiovascular risks including age, sex, body mass index, diabetes, current smoking; †adjusting for model 1 + resting systolic blood pressure, and metabolic equivalent of tasks.

DISCUSSION
This study demonstrated that HRR was closely and inversely associated with CSI after exercise but not CSI at rest. HRR was also weakly associated with baPWV. Several authors have previously reported that carotid atherosclerosis may alter the elastic properties of the arterial wall to collagen fibers and impair the vasoactive paracrine functions of the endothelium such as secretion of nitric oxide, and prostaglandin, thus may decrease the distensibility of the carotid sinus and baroreflex sensitivity.6)9)15)16)17) Decreased baroreflex sensitivity contributes to the decrease in parasympathetic activity and increase in sympathetic activity that accompany the development and progression of cardiovascular disease.18) Indeed, Nasr et al.19) demonstrated that decreased baroreflex sensitivity was associated with carotid atherosclerosis. Chao et al.15) reported that baroreflex sensitivity was closely associated with HR variability, a typical parameter for estimating autonomic function. Similarly, Jae et al.20) demonstrated that HRR, which is another marker to estimate autonomic function,1)2) was impaired in patients with carotid atherosclerosis with stenosis > 25% and/or intima-media thickness > 1.2 mm. However, this association between HRR and carotid atherosclerosis might be clearly observed after overt atherosclerotic change. Indeed, HRR was not associated with CSI at rest in our study, which only enrolled patients with a low atherosclerotic burden of carotid plaque < 1.5 mm (average carotid intima-media thickness = 0.6 ± 0.1 mm). Meanwhile, HRR was weakly associated with baPWV when established cardiovascular risks were adjusted. However, the association between the two factors was not significant when systolic BP or metabolic equivalent of tasks were included as confounding factors. We surmise that this is because measurement of baPWV is pressure-dependent.5) Therefore, autonomic activity following exercise might not be closely associated with atherosclerotic change apart from established cardiovascular risks, at least in the early atherosclerotic stage.
Several studies have consistently shown that repetitive aerobic exercise training improved arterial stiffness.21)22)23) On the contrary, the immediate impact of aerobic exercise on arterial stiffness might be complex and controversial according to the anatomic site at which the arterial stiffness was assessed, the timing of the measurement post-exercise, the intensity of the exercise, and characteristics of the patients.21)24) Seo et al.25) demonstrated that arterial stiffness measured by baPWV was decreased after maximal treadmill exercise. However, Liu et al.21) demonstrated that immediate carotid stiffness was increased after acute exercise training of moderate intensity, but the difference before and after exercise tended to decrease according to repetitive exercise training. Mutter et al.24) insisted that stiffness on the central and upper body peripheral arterial segments deteriorated for a short duration after exercise and then improved, while stiffness on the lower arterial segments decreased regardless of the post-exercise timing of the measurement. Some researchers suggested that the decrease in arterial stiffness after acute exercise is due to increased release of shear stress-induced nitric oxide or other vasoactive agents.26)27) However, Sugawara et al.28) demonstrated that immediate vasodilation after low intensity exercise was not associated with increased production of nitric oxide. Boutouyrie et al.29) also insisted that autonomic activity to modulate sympathetic tone during exercise might be a mechanism of decreased arterial stiffness after acute exercise. The results of this study do not allow us to confirm which hypothesis is right. However, the close association between HRR and CSI after exercise may exist because CSIs after exercise are modulated by autonomic activity as well as vascular endothelial function.
In this study, the correlation between baPWV and CSI at rest was weak. BaPWV is an atherosclerotic marker to indirectly assess arterial stiffness in regional muscular components as well as the aortic, brachial, femoral and tibial arteries.30) On the other hand, CSI is a direct stiffness marker limited to the carotid artery. The arteries of the entire body are not homogeneously affected in the progression of atherosclerosis. In general, the carotid artery becomes stiffer than the femoral or radial arteries in association with aging and high BP.31)32) This study suggested that baPWV might be a more useful marker to estimate association with autonomic function derived by HRR than CSI at rest.
CSI at rest was not associated with HRR but was highly associated with CSI after exercise, even after adjusting for established cardiovascular risks and HRR (data not shown; Stβ = 0.412, p < 0.001). It might be suggested because the two markers measured arterial stiffness on the same anatomic site.
This study had some limitations. First, we measured brachial BP instead of central BP to calculate CSI. The BP measurement may have been overestimated because peripheral arterial pulse pressure is amplified compared with central arterial pulse pressure.5) However, some previous studies have demonstrated that a stiffness index using peripheral BP had a very good correlation with indices using central BP33)34) and also was clinically useful.35) A second limitation is that we measured baPWV, but we did not measure carotid-femoral PWV (cfPWV) which has been traditionally used to evaluate aortic stiffness. Although the value of baPWV is higher than that of cfPWV because of the inclusion of the stiffness of the peripheral muscular artery,30) baPWV is known to have good correlation with cfPWV36) and aortic PWV measured by an invasive method.37) In addition, baPWV is easier to measure, so it has better intra- and inter-observer reproducibilities than cfPWV.38) Finally, because this was a cross-sectional study, we could not determine causation between arterial stiffness and HRR.
CONCLUSIONS
Sympathovagal imbalance indicated by slow HRR after exercise was associated with increased arterial stiffness in normotensive patients without overt atherosclerosis. Furthermore, the close association between HRR and exercise-induced carotid arterial stiffness might have been observed because autonomic function following exercise as well as vascular endothelial function determine carotid arterial vasomotion after exercise.
 XML Download
XML Download