

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pre-operative echocardiographic assessment of MV pathology has become of crucial importance with the transition from prosthetic mitral valve (MV) replacement to MV repair in the last decades. This has more recently been facilitated by development of newer echocardiographic techniques such as three-dimensional (3D) imaging1)2) and simultaneous biplane imaging.3)4)
Communication between the cardiologist and the surgeon is as important as the obtained echocardiographic information. Therefore, in 1983, Carpentier5) proposed a clearly defined, universal MV leaflet terminology. The normal MV is comprised of an anterior leaflet connected on either side through the anterolateral and posteromedial commissures to the posterior leaflet. The anterior leaflet occupies two-thirds of the valve area, whereas the posterior leaflet occupies only one-third, and the latter leaflet is connected to two-thirds of the annulus. The posterior leaflet consists of three scallops or segments: the lateral scallop is labeled P1, the middle scallop P2, and the medial scallop P3. Although the anterior leaflet is smooth without natural scallops, the leaflet parts opposing the corresponding posterior leaflet scallops are accordingly labeled A1, A2, and A3. Because the P2 scallop is relatively large, it may be divided into lateral and medial halves (P2L and P2M) or even divided into three parts: centro-lateral (P2CL), central (P2C), and centro-medial (P2CM). The two commissures are usually also composed of small scallops and may be designated as the lateral commissural scallop (CL) and medial commissural scallop (CM).6) The chordae arising from the anterolateral papillary muscle are attached to CL, A1, P1, A2L, and P2L, whereas those arising from the posteromedial papillary muscle are attached to CM, A3, P3, A2M, and P2M.
In addition to the leaflets and their scallops, the MV apparatus includes an annulus, chordae tendineae, papillary muscles, and the left ventricle (LV). Mitral regurgitation (MR) may develop when any part of the MV apparatus becomes abnormal. Carpentier5) described the pathophysiologic classification of the three types of MV pathology on the basis of a functional approach that were linked to specific repair techniques. Type I involves normal leaflet motion, type II is associated with increased leaflet motion, and type III is associated with restricted leaflet motion.
More recently, Shah and Raney7)8) proposed a modified echocardiographic classification of MR mechanisms to provide a more comprehensive and detailed assessment of MV disorders that is relevant to modern MV repair techniques. In this report, we give an overview of the Shah and Raney pathological MR classification (Table 1), with special attention to the added value of 3D-echocardiography. The focus is on trans-esophageal 3D imaging because, in our experience, 3D transthoracic imaging of the MV has limited accuracy even in the hands of experts.3)9)10)11)
Table 1
Echocardiography-based classification of mitral valve pathology

CLASSIFICATION OF MV PATHOLOGY
Type I: Normal leaflet motion
This type of pathology is the same as in the original Carpentier classification. The MV leaflets have normal excursion and subannular leaflet coaptation without a tenting or tethering appearance. Underlying pathologies for MR of this type are now sub-categorized as leaflet perforation (Type I-A), congenital cleft deformity (Type I-B), and pure annular dilatation without leaflet tethering (Type I-C).
MV leaflet perforation can be the result of trauma but is most commonly caused by localized infective tissue destruction. Other than primary MV endocarditis, aortic valve endocarditis can also directly extend toward the anterior MV leaflet via the anatomically shared fibrous trigones or be transmitted via the aortic valve regurgitation blood jet.12) Three-dimensional echocardiography provides added benefit to traditional two-dimensional (2D) imaging because of its ability to provide en-face visualization of the MV, allowing more precise anatomical localization and measurement of the size of the leaflet perforation, as seen in Figure 1.13)
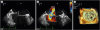
Figure 1
Mitral valve perforation in the medial part of the anterior leaflet, identified with 2D grayscale (A, see arrowhead), 2D color (B), and with 3D echo from the left atrial (surgical) view (C, see arrowhead).
A congenital cleft of the MV is most commonly seen in association with an atrioventricular canal defect, but an isolated cleft of the anterior or posterior MV leaflet has also been described.14) In this subtype, 3D echocardiography provides superior diagnostic accuracy and may improve surgical results.15)16) An MV cleft can be easily seen on the 3D image from both the atrial (Figure 2A) and ventricular (Figure 2B) aspects of the MV, whereas it is often extremely challenging to make the correct diagnosis with 2D echocardiography. It is important to differentiate true clefts from drop-outs (facilitated by use of color Doppler) and pseudo clefts from deep folds in myxomatous MV disease, particularly post-MV repair.
Figure 2
Three-dimensional echocardiographic surgical view of an anterior mitral valve leaflet cleft seen from the left atrial (surgical) view (A, see asterisk) and left ventricular view (B, see asterisk).

Mitral annulus dilatation is usually seen in combination with the later described types II and III MR.17) Pure or isolated mitral annulus dilatation in the absence of leaflet tethering or prolapse is mainly seen in patients with chronic atrial fibrillation but also in patients with heart failure with preserved LV function.18) The location of MV leaflet coaptation with respect to the annulus is normal, but the zone or surface of coaptation is reduced, resulting in central MR. The definition of annulus dilatation with 2D echocardiography is limited by lack of clear data regarding the best echocardiographic view in which it should be measured.19)20) The apical 4-chamber view is recommended in some instances,21) although it is well known that this view does not represent a consistent or reproducible axis of the mitral annulus.22)23)24) In contrast, 3D echocardiography provides an en-face view of the mitral annulus from which multi-planar reconstruction or modeling of the MV enables precise measurements not only of the major and minor axes, but also of the complete annular circumference (Figure 3).

Type II: Increased leaflet motion
This type is characterized by MV leaflets exhibiting excess excursion into the left atrium and is also the same as in the original Carpentier classification but now has three subtypes. In type II-A there is typically fibro-elastic deficiency with thin and friable chordae that lead to a prolapsing segment due to chordal elongation, eventually resulting in a flail leaflet prolapse due to chordal rupture (Figure 4A). Acute flail leaflet prolapse may also be the result of chordal rupture in acute endocarditis or (less often) papillary muscle rupture due to acute myocardial infarction (Figures 4B to 4E). The MR jet in this type is always eccentric: anteriorly directed in posterior MV leaflet prolapse and posteriorly directed in anterior MV leaflet prolapse. A late-systolic central jet may be seen in billowing leaflets due to chordal elongation (Type II-B, Figures 5A to 5C). In its extreme form, there is significantly increased diffuse redundant and thickened leaflet tissue due to myxoid infiltration and annulus dilatation with multiplecentral and eccentric regurgitant jets known as myxomatous Barlow's disease (Figures 5D and 5E). In patients with more severe chordal elongation, the regurgitant jets may occur earlier in systole. The combination of these two types results in a third subtype consisting of billowing leaflets with associated flail due to chordal rupture that also results in multiple jets (Type II-C).
Figure 4
Type II-A mitral valve prolapse due to fibro-elastic deficiency with chordal rupture (A, see arrowhead). Acute flail mitral valve leaflet prolapse due to antero-lateral papillary muscle rupture (B, see arrowhead) and postero-medial papillary muscle rupture (C: gray-scale, see arrowhead, D: color Doppler, E: 3D image, see arrowhead).

Figure 5
Type II-B billowing mitral valve leaflets due to chordal elongation seen with 2D transthoracic (A), 2D trans-esophageal (B), and 3D echocardiography (C: surgical view). Diffuse redundant and thickened leaflet tissue known as myxomatous Barlow's disease is seen with trans-esophageal echocardiography without (D: type II-B) and with chordal ruptures (E: type II-C).

Of note, the terms flail, prolapse, and billowing MV are often used differently, especially between cardiologists and surgeons. Billowing refers to passing of only the body of the MV leaflet above the mitral annular plane (Figures 5A to 5C), whereas prolapse means that the leaflet tips are also above the mitral annular plane. Prolapse, unlike billowing, is always associated with MR. A flail MV leaflet is an extreme form of prolapse associated with chordal rupture (Figure 4A) or extreme chordal elongation without rupture.
The presence, location, and extent of prolapse are of crucial importance in defining the likelihood of successful MV repair.25)26) Compared to 2D imaging, 3D echocardiography obviates the need to mentally reconstruct the MV in three dimensions from multiple 2D images to understand the underlying MV anatomy. The entire MV can be visualized in a single image, making it possible to examine both leaflets from the left atrial (surgical) perspective, which allows more definitive identification of the localization (Figure 6) and extent (Figure 7) of prolapse. This technique may also be less operator dependent because it does not require the finesse of probe manipulation to delineate MV pathology. Several studies have shown that time to diagnosis was considerably faster and diagnostic accuracy improved with 3D echocardiography, in particular for identification of P1 and P3 prolapse.6)
Figure 6
Mitral valve prolapse site identification with trans-esophageal commissural view 2D imaging (left column), color-imaging (middle column), and 3D imaging (right column). Seen are prolapses (asterisks and arrowheads) of the P1 (top row A-C), P2 (middle row D-F), and P3 (bottom row G-I) scallops.


Type III: Restricted MV leaflet motion
In the original Carpentier classification, type III was divided into two subtypes: IIIA with restricted opening and IIIB with restricted closure. Shah and Raney8) proposed division of this type into three subtypes.5)
Type III-A is characterized by systolic and diastolic restriction as seen in rheumatic and other inflammatory pathologies and is associated with commissural fusion, chordal shortening, and fibrosis. The leaflets are thickened and shortened, resulting in inadequate coaptation and regurgitation (Figures 8A and 8B). The main role for 3D echocardiography in this subtype is assessment of the MV area, and this has become the reference method of classifying MV stenosis (Figure 8C)27)28) because it facilitates imaging of the true narrowest opening of the MV orifice. Still, it should be recognized that this measurement is – as the 2D measurement – challenging in the presence of severe calcification. The use of a 3D Wilkins score may improve the traditional 2D Wilkins score for selection of patients suitable for MV plasty.29)30)
Figure 8
Mitral valve restriction seen with 2D trans-thoracic gray scale and color imaging in rheumatic disease with systolic and diastolic restriction (A, B, and C show the 3D surgical view with reduced valve opening) in dilated cardiomyopathy with symmetric systolic restriction (D and E) and ischemic cardiomyopathy (F and G) with asymmetric systolic restriction. In the bottom panel (H), 3D echocardiographic virtual models are seen from the commissure-to-commissure view. The 3D tenting area and tethering angle of segment P3 (arrow-line) may predict recurrent mitral regurgitation after annuloplasty. AC denotes anterior commissure and PC denotes posterior commissure. Reproduced with permission from Bouma et al.37)

In types III-B and III-C, there is systolic restriction with one or more tethered leaflets. Tethering on echocardiography is characterized by systolic displacement of one or more leaflets from the annular plane.31)32) The closure and position of mitral leaflets are determined by the balance between two forces acting on them: the closing forces generated by the LV systolic contraction, which effectively closes the valve, and the tethering forces, which restrain the leaflets to prevent leaflet prolapse. When tethering is increased by outward displacement of the papillary muscles and the closure forces are reduced by LV dysfunction, the equilibrium between these two forces is disrupted in favor of tethering forces, with displacement of the coaptation point of the leaflets in the ventricle.
Two tethering patterns have been described33) and in the new approach are classified as type III-B symmetric (Figures 8D and 8E) and type III-C asymmetric (Figures 8F and 8G) restriction. Systolic symmetric tethering with central MR is seen in dilated or chronic global ischemic cardiomyopathy with outward displacement of the papillary muscles and annulus dilatation with the point of coaptation remaining at the leaflet tips but displaced toward the apex with a reduction in coaptation zone.33) The severity of this type of MR is greatly related to dynamic changes in loading conditions seen in treatment with diuretics, afterload reducing agents, or general anesthesia (Figure 9).34) 3D echocardiography may quantify dynamic changes that occur in the mitral annular surface and its 3D longitudinal displacement and characterize the complex geometric relationship between the papillary muscles and the MV apparatus.35) Some have advocated measurement of the tenting pattern, especially regional 3D tethering of segment P3, as a predictor of long-term prognosis in patients with dilated cardiomyopathy36) or as a predictor of recurrent ischemic MR after undersized mitral ring annuloplasty.37)
Figure 9
Influence on the severity of trans-esophageal assessment of mitral regurgitation by peri-operative blood pressure changes (A) and general anesthesia (B: significant mitral regurgitation in the outpatient clinic, C: minimal mitral regurgitation under general anesthesia).

Asymmetric systolic restriction as seen in type III-C (Figures 8F and 8G) typically occurs in patients with a localized posterior wall motion abnormality and results in tethering of the corresponding leaflet, whereas the other normal leaflet overrides the point of coaptation without going above the annular plane. It is important to recognize that this latter leaflet is thus not prolapsing but only overriding a restricted opposite leaflet.
Type IV: Systolic anterior motion
Systolic anterior motion (SAM) of the MV may lead to significant MR and is seen in different circumstances. In general, the role of 3D echocardiography in recognition of SAM is minimal.
Type IV-A is seen in hypertrophic cardiomyopathy characterized by anteriorly displaced papillary muscles and elongated MV leaflets with a residual portion of the anterior MV leaflet extending beyond the point of coaptation.38) This portion is not constrained by the left atrial – ventricular pressure differences but freely moves with the flow in the LV outflow tract. In particular, in patients with a relatively short posterior MV leaflet, SAM causes an eccentric MR jet directed laterally and posteriorly (Figure 10A).
Figure 10
Mitral regurgitation due to systolic anterior motion (see arrowheads) in hypertrophic cardiomyopathy (A) and after mitral valve annuloplasty (B: gray-scale and C: color Doppler).

Type IV-B is seen after MV repair. Pathologic motion of the distal MV leaflet as described above may be simulated by a disproportionate reduction of the MV annulus compared to the size of post-repair MV leaflet tissue (Figures 10B and 10C).
Type IV-C is seen in a hypovolemic, hyperdynamic LV. Typically it is seen during dobutamine stress39) or with excess doses of inotropics in hypotensive states, paradoxically worsening hypotension.
Type V: Hybrid motion in co-existing pathologies
Hybrid pathologies include combinations of more than one pathology in a patient. Examples include intrinsic pathology with a superimposed infective endocarditis lesion and restrictive posterior leaflet pathology combined with anterior leaflet prolapse or SAM.
SPECIFIC ROLES OF 3D COLOR IMAGING IN ASSESSMENT OF MV PATHOLOGY
The main application of 3D color imaging for assessment of MV pathology is in assessment of paravalvular leakage after MV surgery.40) Evaluation of the extent and shape of the leaking orifice and the site of annulus detachment is critical in assessment of paravalvular leakage and may best be provided by the surgeon's en-face view of the prosthetic MV from the left atrium (Figure 11). In addition, color 3D imaging may facilitate the differentiation of 3D drop-out artifacts from true defects.41)
Figure 11
Three-dimensional echocardiography showing mitral ring dehiscence (A) and replacement with a mechanical prosthesis (B). The lower panel shows localization of smaller paravalvular leakage after implantation of a mechanical prosthesis by the origin of the 3D color Doppler jet (C, arrowhead), facilitating wire passage (D, arrowhead) and thus placement of a closure device.

CONCLUSION
Accurate description of the MR mechanism is crucial for determination of the need for and type of MV surgery. Addition of 3D echocardiography may be particularly helpful in identification of MV leaflet perforation, cleft, or prolapse and a more reproducible definition of MV annulus dilatation. The described modified classification by Shah and Raney provides a more comprehensive and detailed assessment of MV disorders. Further studies should investigate whether this modified classification has an impact on surgical techniques and outcome.
 XML Download
XML Download