

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Microdontia is a condition when the teeth are abnormally small. There are 3 types of microdontia: true generalized microdontia, relative generalized microdontia, and localized microdontia.1 True generalized microdontia can be classified when all the teeth are smaller than the normal size. It is very rare, and occurs in pituitary dwarfism, Fanconi's anemia, or a variety of syndromes. Relative generalized microdontia is when all the teeth are normal size but appear smaller relative to large jaws. Localized microdontia, which is more common than generalized microdontia, is when a single tooth is smaller than normal. The most frequently involved tooth is the maxillary lateral incisor, which may be shaped like an inverted cone. The frequency of peg-shaped maxillary permanent lateral incisors is around 1.8%, and they are more likely to occur in women than men.2 In most cases, microdontia is attributed to a genetic basis and tend to run in families,3 but it can also occur spontaneously.4 Microdontia is usually associated with hypodontia and may have retained deciduous teeth, missing deciduous teeth, or missing permanent teeth.5 In patients with microdontia, esthetics may be the main concern. Thus, the treatment strategies generally focus on the corrections of appearance and abnormal gaps between teeth without compromising function.
Modern restorative dentistry focuses on improving the esthetics and keeping the sound dental tissues as long as possible. Thus, in view of minimally invasive or even noninvasive approaches, current restorative dentistry move forward toward dental adhesive systems allowing for biomechanical functions.6 Minimally or noninvasive treatment modalities can be particularly indicated in young patients with immature, still developing dental tissues. The concept of selection criteria between direct and indirect restorations has been changed due to the introduction of minimally invasive treatments with adhesive techniques. Direct restorations may be advantageous when considering risk factors associated with tooth vitality, patient age, cost, and retrievability. However, indirect restorations still can be chosen in cases of high esthetic demand or large extent of involved teeth.7 Ceramic materials can provide desired esthetics while the principal limitation of ceramics is their brittleness.
Zirconia, which has esthetic potential and high strength, continues to play an important role in modern esthetic dentistry. As an alternative to porcelain-veneered zirconia, use of zirconia in monolithic fullcontour designs has gained wide popularity to eliminate the chipping problem. With high fracture resistance, monolithic zirconia enable to preserve as much dental tissues as possible allowing reduced prosthetic space.8 Due to its polycrystalline microstructure, the internal light scattering results in opaque appearance. Thus, zirconia has been continuously developed to enhance its translucency. By increasing yttria content up to 5 mol%, high translucent cubic-phase zirconia containing about 50% cubic phase was introduced. This new category of cubic-phase zirconia (5 mol% yttria partially stabilized zirconia, 5Y-PSZ) can offer improved translucency similar to9 or even higher than that of lithium disilicate glass-ceramic.10 On the contrary, other studies reported that cubic-phase zirconia has lower level of translucency than that of lithium disilicate and it can't take the place of enamel.1112 The high translucent cubic-phase zirconia is found to be more resistant to aging behavior than 3 mol% yttria-stabilized tetragonal zirconia polycrystalline (3Y-TZP).13 However, reduced mechanical strength is inevitably accompanied by a sacrifice in the transformation-toughening mechanism13 although cubic-phase zirconia has demonstrated superior mechanical properties than lithium disilicate glass-ceramic.12
A digital technology is gaining momentum in all aspects of dentistry, including digital imaging, guided surgery, digital impressions, and computer-aided design and computer-aided manufacturing (CAD/CAM) fabricated prostheses.14 With a digital workflow, clinical and laboratory steps can be reduced, and thus potential sources of manufacturing error would be minimized.15 Intraoral digital impressions can decrease chair time and increase productivity. It was reported that digital impression techniques would be a reliable alternative15 to or even more accurate than conventional techniques especially for short-span fixed dental prostheses (FDPs).1617
Considerations of the patient's long-term oral health and function, optimal selections of ceramic materials and esthetic designs depending on the individual clinical situations, and adequate tooth bonding techniques would be prerequisites for successful esthetic and functional outcomes in minimally invasive esthetic dentistry. This case report describes a digital workflow of a noninvasive esthetic treatment using cubic-phase zirconia for a patient with isolated microdontia. Human subject approval was obtained from the Ajou University Hospital Institutional Review Board (no. AJIRB-MEDEXP-18-370).
Case report
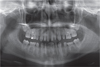
A 15-year-old female who had isolated microdontia in combination with spacing attended Ajou University Dental Hospital for esthetic treatment. She had a healthy general condition with no systemic disease or syndrome, no history of receiving radiation therapy or chemotherapy during tooth development. However, microdontia was running in her family. The clinical examination revealed smaller anterior and posterior teeth with spacing in maxilla and mandible, retained mandibular primary central incisors, and retained mandibular and maxillary deciduous second molars (Fig. 1). The radiographic examination showed agenesis of mandibular second premolars and second molars (Fig. 2). When she was presented with the option of an orthodontic treatment, she said that she did not want “braces”. Her chief esthetic interest was to correct shape and form of the maxillary anterior teeth and to close anterior space. The primary challenge was to establish a harmonious esthetic appearance without compromising function. An additional challenge was to prevent pulpal damage in young teeth with abundant blood supply and a larger pulp.
The teeth were cleaned with pumice to remove the pellicle. Digital impressions of maxillary, mandibular arches, and check bite were obtained using an intraoral scanner (i500, Medit, Seoul, Korea) following the manufacturer's protocol. The Standard Tessellation Language (STL) files exported from the software (Medit LINK, Medit, Seoul, Korea) were transferred to CAD/CAM software (Zirkonzahn Modellier, Zirkonzahn GmbH, Gais, Italy) for a digital wax-up. In consideration of the patient's age, a noninvasive approach to preserve sound dental tissues was planned. To re-create the shape of maxillary anterior teeth from canine to canine, to achieve a progressive emergence profile in the inter-proximal spaces, and to maintain the existing occlusal relationship, six 3/4 laminate veneers with incisal lingual wrap were designed. The gaps between maxillary anterior teeth were more than 1.0 mm, and thus high-translucent cubic-phase-containing zirconia (5Y-PSZ, Luxen Smile S2, DENTALMAX Co., Seoul, Korea) in a monolithic form was used to reduce the risk for unsupported veneer fracture.18
To optimize the esthetic appearance, the width of maxillary anterior teeth was designed trying to obtain 80% proportion when viewed from the front instead of “golden proportion” of 62% because the patient had short anterior teeth.19 In addition, the veneers were designed without creating black triangles in the gingival embrasures to make a more confident smile. With a veneer module in the CAD/CAM software, several parameters were adjusted: cement space, 10 µm; horizontal crown margin, 0.15 mm; minimum thickness, 0.3 mm (Fig. 3). The veneer thicknesses on the labial surfaces ranged from 0.360 mm to 1.142 mm, and the veneer thicknesses on the proximal surfaces ranged from 0.437 mm to 2.462 mm. The increases in incisal length of the veneers ranged from 0.359 mm to 1.499 mm (Fig. 4).
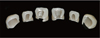
The computer numerical control (CNC) file created from the 3D modeling software was transferred to a milling machine (M5, Zirkonzahn GmbH, Gais, Italy). Six individual cubic-phase zirconia veneers were milled and subsequently sintered in a furnace (ZIRKONOFEN 600/V2, Zirkonzahn GmbH, Gais, Italy) at 1550℃ for 3 hours. Post-sintering staining and glazing were performed to produce final esthetic appearance (Fig. 5). The inner surfaces of the veneers were sandblasted using 50 µm aluminum oxide at a pressure of 0.5 bar.
The maxillary anterior teeth were cleaned using a slurry of pumice and washed thoroughly with water spray. Cementation was done using a dual polymerized resin composite cement (Panavia F 2.0 Light, Kuraray Noritake Dental Inc., Tokyo, Japan) which is a selfetching resin adhesive cement that contain 10-Methacryloyloxydecyl dihydrogen phosphate (MDP). The uncut enamel surfaces were acid etched to remove organic pellicle20 and then, ED primer II was applied to improve the bond strength to enamel according to the manufacturer's protocol. The veneers were seated properly and luted two at a time starting with the central incisors and continuing distally. At 6-month follow-up, neither loss of retention nor biologic complications were detected (Fig. 6A, 6B). The labial surfaces of the veneers were in harmony with the gingival profile without overcontouring (Fig. 6C). Even and stable occlusal contacts ensuring smooth anterior guidances were provided (Fig. 6D). Patient was very satisfied with the natural and esthetic appearance of the prostheses.
Discussion
A noninvasive esthetic restorative approach with a digital workflow is based on maximum preservation of dental tissue by avoiding the need to cut down tooth structures, providing high level of function and comfort to the patient. The definitive prostheses should be designed with respect to periodontal health, strength of the restoration with the limited thickness, and esthetic appearance.
High-translucent zirconia materials which increase cubic contents at the expense of mechanical properties can be selectively applied as a monolithic design in highly esthetic clinical cases. A resin-based adhesive system improves the fracture resistance of monolithic allceramic restorations compared with conventional cementation.21 Recent study reported that the fracture strength of 0.2 mm-thick adhesively bonded high translucent zirconia crowns exceeded maximum chewing forces of 900 N.22 Yan et al.23 investigated that 5Y-PSZ had higher flexural strength (593 MPa) than lithium disilicate glass-ceramic (488 MPa), while lithium disilicate exhibited higher load-bearing capacity (872 N) than 5Y-PSZ (715 N) when adhesively bonded to dentin. In their study, 5Y-PSZ exhibited only slightly lower translucency than that of lithium disilicate glass-ceramic. However, occlusal surface fractures dominated in the thick layers (d > 1 mm) of the monolithic glass-ceramic restorations.24 Therefore, for the clinical application in the esthetic zone with free-standing stress bearing area, high translucent cubic-phase zirconia would be more suitable. In this study, cubic-phase zirconia (5Y-PSZ) with flexural strength of 600 MPa based on the manufacturer's data report was used. Six veneers were fabricated with a horizontal marginal thickness of 0.15 mm and a mean labial thickness of 0.56 mm to avoid over-contoured restorations.
In this study, Panavia F 2.0 was used to cement veneers and the cement space was set at 10 µm. Panavia F 2.0 provided higher values of elastic modulus (7.3 GPa), bond strength to zirconia (40.7 MPa), flexural strength (78.9 MPa) than self-adhesive cements and lower value of water absorption (25.3 µg/mm3) than self-adhesive cements.25 Previous studies demonstrated that bonding strength of resin-based luting agent to cubic-phase zirconia could be increased by using an MDP-containing primer.2627 With respect to the cubicphase zirconia/Panavia/enamel trilayer system, a thin cement layer would be advantageous to enhance the load-bearing capacity due to the elastic mismatch among them; cubic-phase zirconia (200-210 GPa), Panavia (7.3 GPa), and enamel (~70 GPa).2328 In addition, reduced cement space can improve the marginal fit of CAD/CAM fabricated monolithic zirconia crowns.29 In this study, the veneer design included proximal surface and incisal extension. Thus, occlusal stresses, especially during protrusive movement, would be more widely distributed and provided the increased mechanical resistance to fracture.
Cubic-phase zirconia would behave in a different manner to air abrasion compared to 3Y-TZP because cubic zirconia do not undergo transformation toughening after airborne-particle abrasion. McLaren et al.30 reported that cubic-phase zirconia showed a significant decrease in flexural strength, although 3Y-TZP demonstrated no significant decrease or even an increase in strength after airborne-particle abrasion. The authors suggested different surface treatment modalities for cubic-phase zirconia; such as less abrasive particles, lower air pressure, 30 µm alumina coated in silica combined with a silane primer and MDP. In Inokoshi et al.'s study,31 alumina particle sandblasting did not significantly increase surface roughness of cubicphase zirconia although the sandblasted cubic-phase zirconia showed slightly higher roughness values. In this study, the cubic-phase zirconia veneers were sandblasted using 50 µm aluminum oxide particle under reduced pressure (0.5 bar).
In the present study, zirconia veneers were directly bonded to the intact tooth surfaces. The intimate contact and stress distribution within the veneers would affect long-term survival. Previous studies3233 compared the bond strengths of adhesive systems to unprepared and ground enamel surfaces. According to their studies, uncut enamel should be separately etched with phosphoric acid before the self-etching system was used. Accordingly, the intact enamel surface was acid etched before ED primer was applied to improve the bond strength to enamel for this patient.
Due to the improved translucency, superior periodontal stability, and ease of fabrication in CAD/CAM systems, cubic-phase zirconia could be one of the materials of choice in the esthetic zone as a noninvasive approach. The keys for obtaining long-term stability of noninvasive cubic-phase zirconia restorations would be utilizing an adhesive bonding system with high modulus to improve bonding efficiency and minimizing the cement thickness to enhance loadbearing property. Cubic-phase zirconia is mechanically weaker than 3Y-TZP and its elastic modulus is higher than that of lithium disilicate glass-ceramic (95 – 105 GPa),23 and thus clinical guidelines for predictable surface treatments and adhesive bonding systems should be further investigated.
Conclusion
High-translucent cubic-phase zirconia can be indicated for a conservative esthetic dental treatment modality. In this clinical report, cubic-phase zirconia veneers were fabricated by using a digital workflow to correct shape and form of the teeth and the healthy reaction of the supporting dental tissues could contribute to long-term esthetic success.




 XML Download
XML Download