

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Kyeong-Hyeon Park, M.D. , Joon-Woo Kim, M.D., Ph.D., Chang-Wug Oh, M.D., Ph.D.
, Joon-Woo Kim, M.D., Ph.D., Chang-Wug Oh, M.D., Ph.D.
, Joon-Woo Kim, M.D., Ph.D., Chang-Wug Oh, M.D., Ph.D.
Abstract
The incidence of malunion in the long bone with has been reduced because of the advancements in surgical technique. However, nonunion or malunion are still observed in mechanical axis deformation of the lower limb, resulting in the overload of cartilage and instability of the joint, requiring surgical correction. Preoperative planning for malunion is very important, and accurate evaluation of the deformity is essential. Herein, we describe the indications of corrective osteotomy, choice of patients, and various surgical methods for the treatment of malunion of the long bone.
Figures and Tables
 | Fig. 1(A) A 24-year-old male underwent plate fixation due to fracture of the tibia, but angulation and displacement remained. After 12 years of injury, the bone was united. (B) A slight shortening of the lower limb and medial deviation of the mechanical axis were checked, and traumatic osteoarthritis was found in the medial compartment of the left knee compared to the right knee (arrow).
|
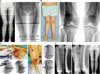 | Fig. 2(A) Valgus deformity was observed in the right distal femur as trauma at the growing age. The mechanical axis was deviated to the lateral side by more than moderately. The mechanical lateral distal femoral angle was 88 degrees on the left side and 80 degrees on the right side. (B) On weight-bearing radiographs, arthritic changes were noted in the lateral part of the knee (arrow), and the patient complained of pain during gait. (C) Osteotomy was performed through the lateral parapatellar approach. (D) The minimally invasive lateral plating was performed with a lateral open wedge osteotomy. (E) After a 3-year follow-up, the femoral alignment was recovered and the union was completed.
|
 | Fig. 3(A) After intramedullary nailing of the proximal tibial shaft fracture, non-union with anterior angulation was confirmed. The center of rotation of angulation was identified (arrow). (B) The angulation was corrected by exchanging the nailing with a blocking screw at the proximal fragment. Six months later, the bony alignment and union was achieved.
|
 | Fig. 4(A) In a 13-year-old male with valgus deformity due to osteochondroma, center of rotation of angulation was located at the distal tibia (arrow). We performed a medial close wedge osteotomy and restored the alignment by compressing the gap of osteotomy. The osteotomy site was fixed with minimally invasive plate osteosynthesis. (B) The anatomical alignment was recovered after operation. Six months later, bony union was completed.
|
 | Fig. 5(A) In a 58-year-old female, malunion with varus deformity after tibia shaft fracture was observed. The center of rotation of angulation was confirmed at the tibial shaft (arrow). (B) Percutaneous osteotomy was performed; an open wedge was made to an obtain angular correction, and minimally invasive plate fixation was performed. (C) After open wedge osteotomy, the alignment of the mechanical axis was restored. (D) One year postoperatively, bony union was achieved, and the mechanical axis was recovered similar to that of the contralateral side.
|
 | Fig. 6(A) A 67-year-old man, who was suspected to have growth plate injuries in childhood, was confirmed to have varus deformity in the left proximal tibia, and mechanical axis was shifted medially. (B) Because center of rotation of angulation was very close to the joint, fixing the plate was difficult and the correction angle was high; hence, acute correction was expected to be difficult. After attaching the Ilizarov external fixator, osteotomy was performed with the hinge placed outside the convexity (arrow). (C) A progressive distraction was performed to correct the varus deformity, and the external fixator was removed 5 months after sufficient bone maturation. (D) After about 10 months postoperatively, we confirm that the mechanical axis was more improved than before surgery.
|
 | Fig. 7(A) A 23-year-old man presented varus deformity after conservative treatment from a left femoral fracture at childhood. Mechanical axis was slightly shifted to the medial side compared with the right side. (B) Physical examination showed that the position of the left foot was rotated inward, and a computed tomography scan confirmed an increased femoral internal rotation. (C) The metal pin was inserted parallel to the anterior femur and then percutaneously osteotomized. After that, the pins fixed in parallel were rotated to correct the desired degree of rotational alignment, and intramedullary nail was inserted. (D) After the correction, the mechanical axis was passed to the center of the knee and the operation was completed. The position of the foot was similar on both sides. (E) On postoperative radiographs, it was confirmed that varus deformity was corrected, and the osteotomy site showed minimal incision. (F) One year later, osteotomy was well united, angulation and rotational deformity were corrected, and the mechanical axis was restored.
|
References
1. Milner SA, Davis TR, Muir KR, Greenwood DC, Doherty M. Long-term outcome after tibial shaft fracture: is malunion important? J Bone Joint Surg Am. 2002; 84-A:971–980.
2. Paley D, Herzenberg JE, Tetsworth K, McKie J, Bhave A. Deformity planning for frontal and sagittal plane corrective osteotomies. Orthop Clin North Am. 1994; 25:425–465.

3. Lustig S, Khiami F, Boyer P, et al. Post-traumatic knee osteoarthritis treated by osteotomy only. Orthop Traumatol Surg Res. 2010; 96:856–860.
4. Russell GV, Graves ML, Archdeacon MT, Barei DP, Brien GA Jr, Porter SE. The clamshell osteotomy: a new technique to correct complex diaphyseal malunions. J Bone Joint Surg Am. 2009; 91:314–324.
5. Borrelli J Jr, Leduc S, Gregush R, Ricci WM. Tricortical bone grafts for treatment of malaligned tibias and fibulas. Clin Orthop Relat Res. 2009; 467:1056–1063.
6. Sangeorzan BJ, Sangeorzan BP, Hansen ST Jr, Judd RP. Mathematically directed single-cut osteotomy for correction of tibial malunion. J Orthop Trauma. 1989; 3:267–275.
7. Oh CW, Kim SJ, Park SK, et al. Hemicallotasis for correction of varus deformity of the proximal tibia using a unilateral external fixator. J Orthop Sci. 2011; 16:44–50.
8. Seybold D, Gessmann J, Ozokyay L, Muhr G, Graf M. The Taylor Spatial Frame. Correction of posttraumatic deformities of the tibia and hindfoot. Unfallchirurg. 2008; 111:985–986. 988–995.
9. Park KH, Kim JW, Kim HJ, et al. Corrective osteotomy of the distal femur with fixator assistance: a novel technique of minimally invasive osteosynthesis. J Orthop Sci. 2017; 22:474–480.
10. Koyonos L, Slenker N, Cohen S. Complications in brief: osteotomy for lower extremity malalignment. Clin Orthop Relat Res. 2012; 470:3630–3636.
 XML Download
XML Download