

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Hip fractures are commonly seen in the elderly population and are increasing in number with the aging of the population. Currently, intramedullary (IM) devices are widely used for unstable intertrochanteric fractures due to their biomechanical properties which permit early loading, especially in patients with unstable fractures.1) Gamma 3 nail (Gamma 3 locking nail system; Stryker, Kalamazoo, MI, USA) is the latest nail in proximal femoral nail system using conventional lag screw. These implants, however, are not free of complications. Commonly reported complications include stress-derived femoral shaft fractures, hip screw cutout from the head/neck fragment, and varus deformity and fracture collapse.2) Less commonly reported complications include femoral head rotation, lateral back out of the implant, and lateral soft-tissue penetration.3) This article presents a case of medial intrapelvic penetration of the lag screw of the Gamma 3 nail with a comprehensive review of the literature regarding this rare complication.
Case Reports
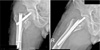
The patient, a 72-year-old man, presented at Busan Veterans Hospital with severe hip pain after a fall. Plain radiography demonstrated an unstable trochanteric fracture (Orthopaedic Trauma Association Type 31-A2.3) of the right femur (Fig. 1). Three days after the initial injury, a closed reduction and internal fixation with Gamma 3 nail (120 degree, 10×170 mm) were performed. The alignment was shown to be within the permissible range in the anteroposterior and lateral radiograph taken using the C-arm fluoroscopy during the surgery, hence the IM nails were inserted. However, due to the inadequate reaming of the trochanteric area, fracture gap widening was identified during the insertion the IM nail. Lag screws were inserted and then distal locking screw were inserted. It was confirmed that the tip apex distances (TADs) were above 25 mm and the locations of the lag screws were on the cleveland zone4) IV in the C-arm fluoroscopy image. However, changing the TADs or the positions of the lag screws were not attempted and the surgery was finished by fixing them in position using set screws (Fig. 2). Although the patient was not allowed to ambulate due to high risk of loss reduction of the fracture, follow-up radiographs at 2 weeks after surgery showed varus displacement and rotation of proximal fragment. The reoperation was not performed at this time because the patient refused revisional surgery (Fig. 3). Weight bearing was prohibited and outpatient clinic visits for routine image follow-ups were advised. The patient was relocated to a hospital near patient's home. Two months after the operation, the patient visited our hospital again. The patient was uncooperative to the recommended visits every two weeks after surgery for image follow-ups. He presented with moderate to severe pain in the right hip without any trauma. After discharge, the patient was committed to being on a wheel chair and the pain was increasing in severity. Shortly after, there was swelling on the lateral side of the hip joint. Radiographs showed perforation of the lag screw into the pelvis through the femoral head and acetabulum (Fig. 4). A computed tomography (CT) scan was performed, and it showed the lag screw lying in the posterior pelvis. The lag screw was located in the proximal portion of the iliopsoas muscle layer. However, no injuries to the major vessels including the common iliac artery, external and internal iliac artery were suspected (Fig. 5). Due to artifact from the screw, we could not elicit accurate details with regard to the proximity of the major pelvic vessels. Angio CT with enhancement for accurate status checkup of lag screw, major vessels and major intrapelvic organs was not performed accordingly to the plan. There were no neurological abnormalities in the physical examination on the lower extremities. We planned to remove the lag screw and IM nail, and perform a total hip arthroplasty. A general surgeon and a vascular surgeon were standing by in the operation room, in case of suspected injury to a vessel or an organ during surgery. The surgery was performed under the general anesthesia with the patient lying in lateral decubitus position for the modified Hardinge approach. The femoral head was eliminated after dislocating the hip joint. A bone deficit was found, which was suspected to have occurred due to a cut-out of a lag screw on the postero-superior region of the femur. The lag screw was embedded postero-superiorly from the center of the acetabulum and near the edge of the acetabulum. About 3 centimeters of the distal portion of the lag screw was exposed. The lag screw was eliminated without much resistance and there were no sign of bleeding or unstable vital signs immediately after. However, while using a electrocautery to eliminate surrounding soft tissue, such as the acetabulum's labrum, the patient's blood pressure dropped abruptly and the patient was deceased. The exact cause of death is unknown since the autopsy was not performed. However, the proximal portion of the lag screw was located in the retroperitoneal area, and the lag screw was located close to the common iliac artery, resulting in adhesion of the surrounding soft tissues; massive bleeding due to vessel injury during the screw remove was presumed to be the cause of death.
Discussion
Several studies have demonstrated a good outcome with few complications after treatment using Gamma nail; however these implants are not free of complications.23) Although cut out of the lag screw or penetration of the femoral head is the key element for intrapelvic migration of gamma nail lag screw,5) the latter complication is considered to be extremely rare.
Werner-Tutschku et al.6) was the first to describe the phenomenon of medial migration regarding the Proximal Femur Nail (PFN, PFN-a; Synthes, Oberdorf, Switzerland). He described it as opposed migration of the lag screw in lateral direction and of the antirotational screw to the opposite. He termed this phenomenon as “Z-effect”.6) So far, this type of dislocation has only been described in 2 screw fixation devices (i.e., PFN). In single screw devices, a few cases of medial intrapelvic migration of the lag screw of a gamma nail have been reported in the English literature.578) Flint et al.5) summarized the proposed risk factors for femoral head and acetabulum penetration and medial migration of lag screws in five categories: i) intraoperative surgeon-related factors; damage of femoral head by over-reaming, malposition of lag screw, ii) intraoperative fracture-related factors; lateral buttress deficiency, unstable medial cortex, malreduction in varus position, osteoporotic bone, distraction of fracture site due to non weight bearing restrictions, iii) implant-related factors; nail/lag screw dysfunction, set screw dysfunction, nail toggling, iv) technical mistakes; too great TAD, superior/anterior placement of lag screw in the femoral head, inadequate lag screw length, v) postoperative factors; fall, additional trauma, abnormal forces to hip articulation.
Only two cases of intrapelvic migration of the lag screw of Gamma 3 nail which is one of the latest proximal femoral nail systems using conventional lag screw were reported.8) The exact etiology of this condition remains unknown due to its uniqueness. Iatrogenic damage of the femoral head during reaming, screw placement in improper position on the femoral head, early loading, subjecting the implant to excessive torsional forces, direct trauma that produces a defect in the screw-nail slot interface, the misplacement of the set screw in the proximal nail extremity, and the choice of a too short or too long cephalic screw have been associated with this unusual complication.578) However, this case is about a pelvic migration of a lag screw that occurred from using the Gamma 3, which is a new thread design and has strong resistance against cut-outs. Horas and Ernst9) reported intrapelvic migration of the Gamma lag screw after treating an unstable pathologic pertrochanteric fracture in a 69-year-old patient. They were unable to place the set screw due to the path being blocked by the polymethylmethacrylate that had been injected to help stabilize the fracture. Four months postoperatively, intrapelvic migration of lag screw was identified on radiographs. The authors recommended using the set screw to prevent medial migration of the lag screw. However, in the present case, all the steps of the surgical technique were properly executed, and set screw was used. There were no evidence that the misplacement of the set screw in the proximal nail have been associated with this unusual complication in surgical procedure. There is a possibility of set screw migration when a force exceeding the set screw stability is applied, due to external force or reduction failure followed by malrotation or varus collapse. Rebuzzi et al.10) showed that out of a total of 981 IM hip fracture fixations, with a ‘risky’ screw position in 21 of these cases, 9 lag screws cut out, with 3 penetrating the acetabulum. This shows that medial migration is relatively common when the screw position is deemed to be risky (43%).10)
The present patient had an unstable intertrochanteric hip fracture with the discontinuity of the medial cortex. We theorized that lag screw cut-out through the femoral head with varus collapse of the fracture due to poor fracture reduction and inappropriate yet eccentric lag screw position in femoral head, there was toggling of the nail with the lag screw which led to the medial migration of the lag screw with repeated axial loading. The authors assume that the fracture was incomplete reduction and the lag screw was inserted at an inappropriate position of the femoral head, resulting in lag screw cut-out after all. Due to the cephalic screw being too short, stable fixation within the femoral head was not achieved and enabled movement, further penetration of the femoral head and eventual migration into the pelvis are aggravated due to poor bone quality.
We emphasize if patient has a less than ideal fixation of an unstable extracapsular hip fracture, then they should be monitored carefully for evidence of medial screw migration. The authors believe if the pelvic penetration is predicted by the medial migration of the lag screw as shown in the presented case, the revision operation should be performed immediately, since the femoral intertrochanteric fracture which has poor fracture reduction status and inadequate lag screw position. When the screw migrates into the pelvis, the status of major vessels and intrapelvic organs related with lag screw should have been performed with abdomenpelvic CT with enhancement. Tauber and Resch described a case of intra-abdominal lag screw migration of approximately 5 cm, treated by implant removal and replacement by revision-THA.6) In their case, however, a massive retroperitoneal abscess under the iliopsoas fascia, with extension to the left periarticular hip region, was found 12 weeks after revision surgery and required multiple reoperations. Therefore, we recommend a precise examination such as abdominal and pelvic CT with enhancement to check for injury in vessels due to lag screw, or injury in intrapelvic organs precedently, and then the operation should be performed with both vascular and orthopedic input due to the close proximity of the major pelvis vessels.




 XML Download
XML Download