

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sexual dysfunction refers to the difficulty that occurs during any stage of sexual response cycle that prevents an individual or a couple from experiencing satisfaction from normal sexual activity. Female sexual dysfunction (FSD) is a relatively common disorder with a prevalence of 30–50%.1 During the menopausal transition, the risk of FSD increases, and the reported prevalence of sexual dysfunction in postmenopausal women ranges from 68–86% in various studies.2 In Korea, the frequency of FSD also increases with age, with the reported prevalence in middle-age women (≥40 years old) being 55–65%.345 The etiology of FSD can be multifactorial, and it can also be affected by various surgical or medical conditions. Gynecologic, physiologic, or pathologic conditions known to be associated with sexual dysfunction are pregnancy and delivery, menopause, infertility, pelvic floor dysfunction, urinary incontinence, gynecological cancer, and uterine leiomyoma.6789
Uterine leiomyoma is also a common problem in gynecologic patients, with a lifetime prevalence estimated to be 25–50%. Previous studies have shown impaired sexual function in the presence of uterine leiomyoma among premenopausal women.910 In the study by Ertunc, et al.,10 uterine leiomyoma was associated with sexual dysfunction, including impaired satisfaction and dyspareunia, and myomectomy was associated with improved sexual function.
However, there is a paucity of information regarding the effect of uterine leiomyoma on sexual dysfunction according to menopausal status. This is an important issue, considering that more women are reaching menopause with uterine leiomyoma rather than undergoing hysterectomy, as conservative treatment is the mainstay in the management of leiomyoma, and menopause itself can affect FSD.11 Additionally, it is well known that sexual dysfunction can result in lower quality of women's life.12
The objective of this study was to determine the relationship between uterine leiomyoma and sexual dysfunction according to menopausal status. To address this issue, we determined the relationship between uterine leiomyoma and sexual dysfunction in premenopausal and postmenopausal women.
Go to : 
MATERIALS AND METHODS
Subjects
In this retrospective cohort study, the study population consisted of consecutive women who underwent gynecologic screening tests, including transvaginal ultrasound, and completed the questionnaires on female sexual function in the Center for Health Promotion and Optimal Aging at Seoul National University Hospital from January 2010 to December 2011. Subjects were excluded if they had a surgical history of hysterectomy. Women who were sexually inactive were also excluded, and sexual inactivity was defined as having sexual intercourse fewer than once per month. Since this study was a retrospective study based on medical records, informed consent was not obtained for this study, and the Institutional Review Board of Seoul National University Hospital approved the study (1102-041-351).
Assessment of patients
Two experienced gynecologists (S.M. Lee and S.M. Kim) performed gynecologic examination and transvaginal ultrasound with LOGIC E9 (GE Medical Systems Information Technologies, GE Healthcare, Milwaukee, WI, USA). Diagnosis of uterine leiomyoma was made by ultrasound finding, defined as a mass of 0.5 cm or larger.13
Questionnaire
All subjects answered questions regarding socio-demographic characteristics, and underwent detailed history taking and ultrasonography to determine both menopausal status and the presence or absence of uterine leiomyoma. Socio-demographic characteristics included previous medical or surgical history, academic career, alcohol consumption, smoking habits, and individual household income. For academic career, subjects were divided by their highest completed schooling level. Smoking or alcohol consumption was divided into the following three subgroups: current, former, or never. Menopause was defined as the cessation of menses for at least 12 months that was not caused by pregnancy, breastfeeding, or other medical conditions.
Female sexual function was determined by the Korean version of Female Sexual Function Index (FSFI).14 FSFI is a well-structured questionnaire with 19 items that assess sexual functioning or problems in six domains (desire, arousal, lubrication, orgasm, satisfaction, and pain) during the past 4 weeks. Scores of each domain range from 1 to 5 or 0 to 5, and the total score is obtained by the sum of the six domain scores multiplied by the domain factor (0.3–0.6). The total score of FSFI ranges from 2 to 36, and FSD is defined as a total score of FSFI ≤26.55.15
Data analysis
Proportions were compared with Fisher's exact test or chisquare test, and comparisons of continuous variables between groups were performed using either Mann-Whitney U test or Kruskal-Wallis test, as appropriate. Logistic regression was conducted for multivariate analysis. p-value <0.05 was considered to be significant. SPSS version 20 software (IBM Corp., Armonk, NY, USA) was utilized.
A prior sample size calculation was performed to determine how many postmenopausal women would be needed to detect a change from 72% to 88% in the frequency of FSD in cases with and without uterine leiomyoma. We estimated that the average frequency of FSD would be 80% in postmenopausal women, based on previous reports.23 Assuming an estimated ratio of 1:1 between those with and without uterine leiomyoma, we determined that we would require 220 postmenopausal women with 80% power and type 1 error of 5%, as well as 284 postmenopausal women with 90% power and type 1 error of 5%.
Go to :
RESULTS
During the study period, a total of 968 women were approached consecutively. Among these women, 841 (87%) completed the questionnaire and were ultimately enrolled in the analysis; 564 women were premenopausal, and 277 were postmenopausal. On transvaginal ultrasound, uterine leiomyoma was detected in 334 women (40%) overall; 40.1% (226/564) of premenopausal women and 39.0% (108/277) of postmenopausal women were affected.
Table 1 compares clinical characteristics according to the presence or absence of uterine leiomyoma in postmenopausal women. All parameters including mean age, body mass index, parity, frequency of diabetes, hypertension, hormone replacement therapy, smoking, alcohol consumption, and the level of education and income did not differ between the two groups.
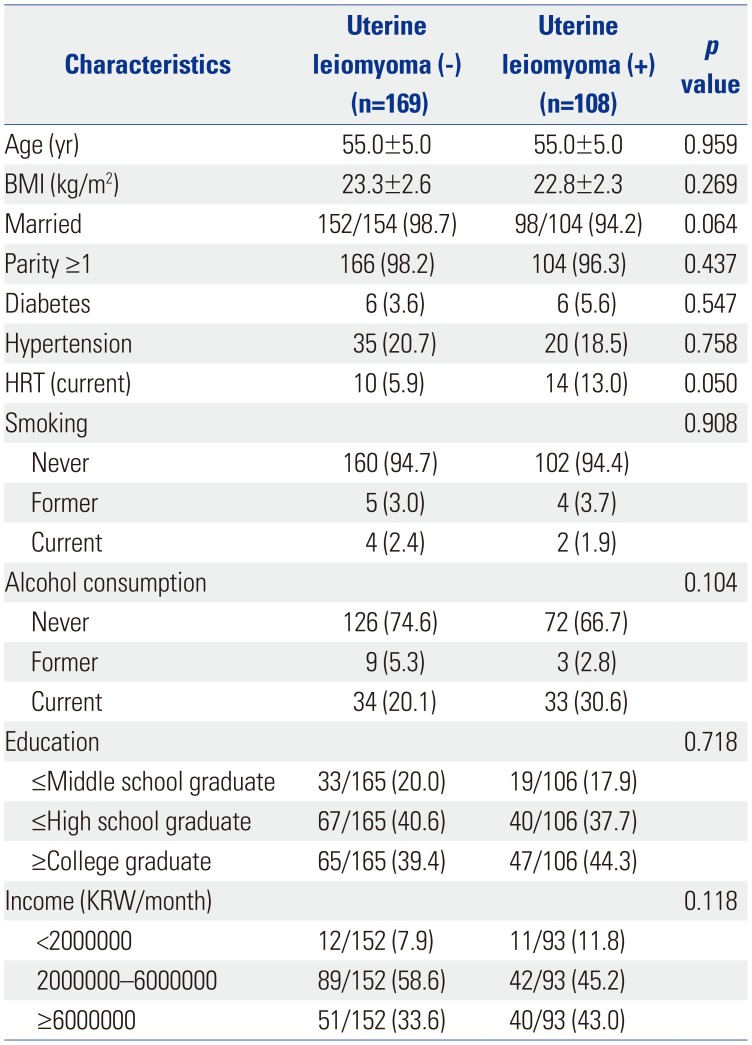
Table 1
Characteristics of Postmenopausal Women according to the Presence or Absence of Uterine Leiomyoma
![]()
Table 2 shows the characteristics of premenopausal women according to the presence or absence of uterine leiomyoma. Women with uterine leiomyoma had significantly higher mean age and body mass index and significant lower height compared to those without uterine leiomyoma.
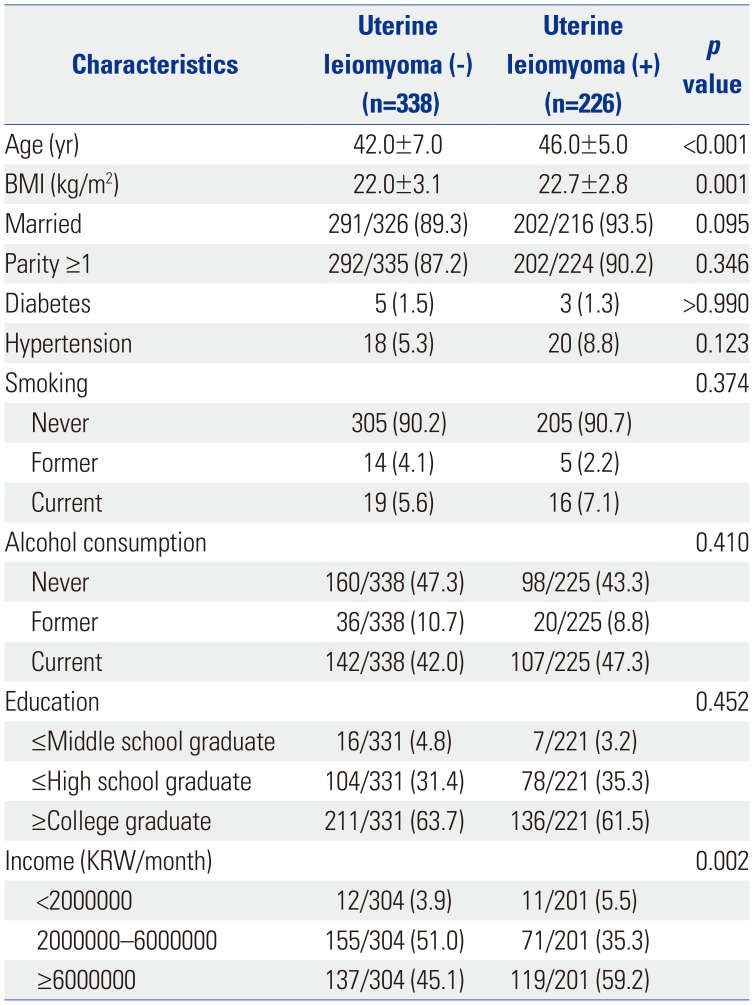
Table 2
Characteristics of Premenopausal Women according to the Presence or Absence of Uterine Leiomyoma
![]()
Table 3 demonstrates the relationship between FSD and uterine leiomyoma in postmenopausal women. Postmenopausal women with uterine leiomyoma had a lower frequency of FSD than those without uterine leiomyoma (frequency of FSD was 71.3% in women with leiomyoma vs. 86.4% in women without leiomyoma, p=0.003), and those women also had a lower frequency of sexual difficulties related to the desire, arousal, and lubrication domains. In addition, women with uterine leiomyoma had higher total FSFI scores, with higher scores in the desire, arousal, lubrication, orgasm, and satisfaction domains than those without uterine leiomyoma. The relationship between uterine leiomyoma and lower frequency of sexual dysfunction in postmenopausal women remained significant after adjustment for confounding variables (Table 4), which were chosen according to the differences between women with and without FSD in univariate analysis (p<0.2).
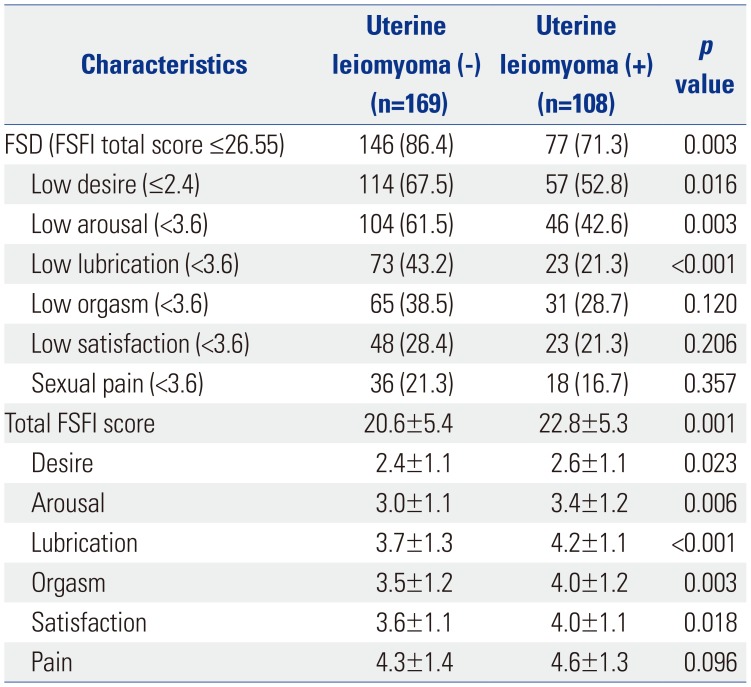
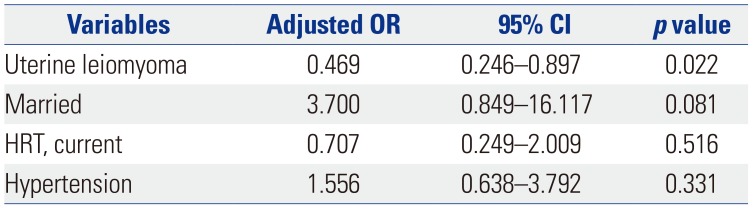
Table 3
Comparison of FSFI Scores in Postmenopausal Women according to the Presence or Absence of Uterine Leiomyoma
![]()
Table 4
Relationship of Significant Variables in Female Sexual Dysfunction in Postmenopausal Women by Multiple Logistic Regression Analysis
| Variables | Adjusted OR | 95% CI | p value |
|---|---|---|---|
| Uterine leiomyoma | 0.469 | 0.246–0.897 | 0.022 |
| Married | 3.700 | 0.849–16.117 | 0.081 |
| HRT, current | 0.707 | 0.249–2.009 | 0.516 |
| Hypertension | 1.556 | 0.638–3.792 | 0.331 |
![]()
In premenopausal group, the frequency of FSD and total FSFI score did not significantly differ according to the presence or absence of uterine leiomyoma (Table 5). However, women with uterine leiomyoma had a higher frequency of sexual difficulty in the satisfaction domain (11.9% vs. 6.2%, p=0.021) and lower mean pain score (5.3±0.9 vs. 5.1±1.0, p=0.046) than those without leiomyoma.
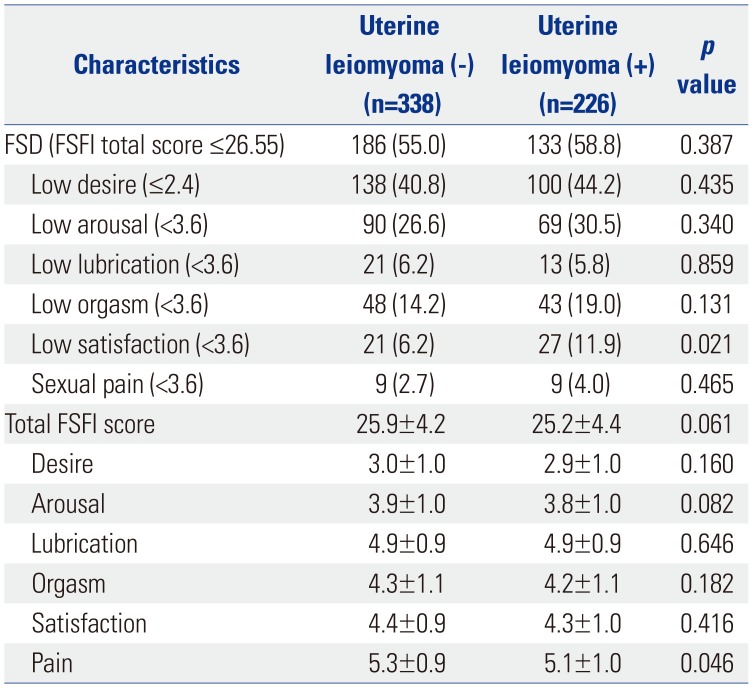
Table 5
Comparison of FSFI Scores in Premenopausal Women according to the Presence or Absence of Uterine Leiomyoma
![]()
Go to :
DISCUSSION
The principal finding of this study is that women with uterine leiomyoma had a lower frequency of FSD than those without uterine leiomyoma in postmenopausal group. This relationship between uterine leiomyoma and lower frequency of sexual dysfunction in postmenopausal women remained significant after adjustment for confounding variables.
Why is uterine leiomyoma associated with a reduced risk of FSD in postmenopausal women? The different concentrations of estrogen may play a role in this association between leiomyoma and FSD. Estrogen is important to sexual function, and decreasing estrogen levels are significantly associated with an increased prevalence of sexual dysfunction in postmenopausal women.16 Menopausal hormone therapy has been reported to improve sexual dysfunction in postmenopausal women,17 and dramatic decreases in estrogen among postmenopausal women is known to cause vulvovaginal atrophy, which can be the cause of dyspareunia.18 The association between uterine leiomyoma and estrogen has also been reported.19 The incidence of uterine leiomyoma is increased when women are exposed to high endogenous estrogen, which occurs with obesity or early menarche, whereas women with decreased estrogen exposure, which is associated with increased parity, have lower incidences of uterine leiomyoma.20 The prior use of hormone replacement therapy is associated with an increased risk of uterine leiomyoma in postmenopausal women.21 In the study by Randell, et al.,21 postmenopausal women with leiomyoma had higher bone mineral density and lower risk of fracture than those without leiomyoma, and the authors suggested that this may be due to higher estrogen levels leading to both higher bone mineral density and the growth of leiomyoma. According to these studies, it may be postulated that the presence of uterine leiomyoma indicates a relatively higher level of endogenous estrogen in postmenopausal women, which in turn result in reduced risk of FSD. In the current study, we did not measure the endogenous estrogen level in the study population, and this needs to be evaluated in further studies.
In the current study, we did not examine sex-related distress and partner factors that contribute to sexual function. Further studies may be needed to demonstrate the relationship between sex-related distress and uterine leiomyoma, and to adjust partner factors.
To the best of our knowledge, this is the first study to evaluate the relationship between FSD and uterine leiomyoma according to menopausal status, and we have demonstrated that the presence of uterine leiomyoma is associated with the risk of FSD in postmenopausal women.
Go to :
 XML Download
XML Download