

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Obesity is related to a variety of metabolic disorders, such as type 2 diabetes mellitus, hypertension, hyperlipidemia, obstructive sleep apnea, and non-alcoholic fatty liver disease, and even malignancies like colon and breast cancer. The prevalence of obesity is increasing worldwide, and this increasing trend has also been observed in Asian countries. According to the Korea National Health and Nutritional Examination Survey (KNHANES) in 2016, the prevalence of obesity [body mass index (BMI) ≥25]1 in Korea has increased to 42.3% for males and 26.4% for females.2 Studies on nonsurgical treatment options for obesity rarely extend beyond 12 months. Bariatric surgical procedures are known to achieve substantial weight loss and provide major secondary health benefits. Due to its ease, safety, and adjustability, laparoscopic adjustable gastric band (AGB) has been one of the most popular bariatric procedures, and unlike Roux-en-Y gastric bypass (RYGBP) and sleeve gastrectomy (SG), it does not alter GI tract anatomy. However, slippage, infection, and migration (erosion) of the band system remain common chronic problems and are major causes of band removal. In the longer term, we have witnessed disturbance of food passage and proximal dilatation above bands in patients without complication. The higher than expected rates of complications and reoperation have resulted in a loss of favor of AGB. In a recent study conducted by the American College of Surgeons' National Surgical Quality Improvement Program (NSQIP), RYGBP, AGB, and SG accounted for 58.4, 28.8, and 9.3% of procedures in 2010 but for 37.6, 3.1, and 58.2% in 2014, respectively.3 Results regarding the long-term incidence of AGB explantation are contradictory. The majority have reported that about 50% of AGBs are explanted in the long-term (>10 years),45678910 whereas O'Brien, et al.11 reported that only 5.6% of bands were explanted in a 10-year follow-up study of 714 patients and that the need for revision decreased as the technique evolved, with a 40% revision rate for proximal gastric enlargements during the first 10 years and a revision rate of only 6.4% during the last 5 years. In the present study, we investigated the incidences, types, and causes of AGB explantation over 10 years of clinical practice. In addition, we evaluated morbidities associated with explantation by different surgical techniques.
MATERIALS AND METHODS
This retrospective review was conducted using prospectively maintained data of patients that underwent AGB implantation and explantation by one surgeon (S.M.K.) at a single tertiary center. Guidelines issued by the Asian Consensus Meeting on Metabolic Surgery (2008, Trivandrum, India) regarding BMI restriction for AGB implantation were followed in all cases (http://www.acmoms.com/acmom_2008.html). Operations were performed using the following bands: LAP-BAND® (Allergan, Irvine, CA, USA) with different modifications (9.75/10.0, AP series), Swedish adjustable gastric band® (Obtech Medical, Baar, Switzerland), and Midband™ (MIDBAND, Medical Innovation Development, Villeurbanne, France). The AGB procedure was performed as described previously.1213 In brief, port positions included a 15-mm umbilical port for a camera and two 5-mm ports (one in each subcostal area) for instruments. A Nathanson liver retractor (Cook Medical, Queensland, Australia) was inserted through a 5-mm skin incision in the subxiphoid location and curved upward to retract the left hepatic lobe. In all cases, a pars flaccida dissection technique was used, whereby entry into the lesser sac was avoided by placing the band suprabursally around gastric vessels and fat instead of close to the gastric wall. Two or three gastrogastric 2-0 Ethibond sutures (Ethicon Inc., Somerville, NJ, USA) were inserted, and tubing was exteriorized and fixed to the port, which was sutured in place on anterior abdominal fascia.
The band was not inflated at band placement completion and left deflated for 4–6 weeks, when it was incrementally inflated over 3–4 sessions under radioscopic control in a radiology suite. Subsequently, depending on body weight changes, food portion sizes, and hunger, small volume adjustments were performed without barium swallow (usually, 0.1–0.3 mL saline was added or removed). A barium swallow test or gastroscopy was performed whenever there was clinical suspicion of a complication, such as slippage or erosion (incapacitating vomiting, reflux, epigastric pain). Upper GI barium swallow findings were classified as previously described,14 Gastroscopic findings of reflux esophagitis were classified using the modified Los Angeles classification system.15 Degree of band migration was classified based on gastroscopy findings as described below by Nocca, et al.16 We assigned patients that required (or requested) AGB explantation to one of three groups based on clinical judgment.
- Slippage (SL): the SL group consisted of patients diagnosed to have acute or chronic slippage with an abnormal phi angle by upper GI barium swallow study not corrected by completely deflating the band.
- Band Erosion (BE): the BE group consisted of patients with moderate to severe symptoms attributable to intragastric band migration by endoscopy or infection of the band system by abdominal CT.
- Intolerance (IT): the IT group consisted of patients exhibiting functional or psychologic intolerance. Functional intolerance was defined as partial or total food intolerance.
Usually these patients had moderate to severe esophagitis (LA grade ≥B) by gastroscopy or pouch/esophageal dilatation by upper GI without definite evidence of slippage or erosion. Psychologic intolerance was defined when proper band adjustment was not possible because the patient was concerned that they could not tolerate band tightening. These patients often requested AGB explantation for fear of future complications but had no sign or symptom of esophagitis, and radiologic studies revealed normal pouch/esophagus morphology without evidence of slippage or band erosion. Patients that underwent band to band revision, that is, removal and immediate replacement, were not included in the present study, because we considered the latter patients, maintaining their weight loss with in situ band, were different from the patients having AGB explanation.
When the extragastric approach for AGB explantation was performed in the BE group, three steps were performed to ensure safe closure of gastric perforation after explantation,17 as follows: 1) primary repair using absorbable suture materials, for which an interrupted suture was used to close the defect; 2) omental plugging involving fashioning of segmented vascularized omentum and its gentle insertion through the tunnel leading into the stomach that is usually left after band extraction and fixing in place by placing multiple sutures through a relatively healthy gastric wall; 3) drainage catheter insertion involving subphrenic Jackson-Pratt (JP) drain insertion through a left subcostal incision. Transgastric AGB explantation was performed via short gastrotomy and intragastric division of the eroded AGB with laparoscopic scissors. Gastrotomy was doubly closed with 2-0 Vicryls. A JP drain was also inserted onto the repaired gastrotomy. Endoscopic removal was performed for Nocca grade II, III BE patients under conscious sedation in an endoscopy suite. A gastric band cutter device (GBC; AMI, GmbH, Götzis, Switzerland) was used for the removal. Port and remaining tubes were removed under local anesthesia. In SL and IT groups, we simply cut and removed AGB after minimal capsular dissection around the band. Perioperative complications recorded after AGB explantation were graded using the Clavien–Dindo classification of surgical complications.18
Data were gathered from hospital medical records, postoperative visit findings, telephone interviews or e-mail responses, and in-office evaluations performed by the authors. Annual incidences and patterns of AGB implantation and explantation were analyzed. Demographic and anthropometric data, duration of having an AGB in situ, operative times, hospital stays, operative approaches, and morbidities in the SL, BE, and IT groups were compared. We also evaluated complications of BE with respect to surgical approach. Data were analyzed using SPSS ver. 11.5 (SPSS Inc., Chicago, IL, USA). Continuous variables are presented as mean±standard deviation and compared using one-way ANOVA test for independent samples. Categorical variables are described using frequency distributions and presented as frequencies (%). Categorical variables were compared using Pearson's Chi-squared or Fisher's exact test as appropriate. All tests were two-tailed, and statistical significance was accepted for p<0.05. The study was approved beforehand by the institutional review boards of Gachon University College of Medicine (GCIRB 2018-388).
RESULTS
Incidences and patterns of AGB explantation (n=99)
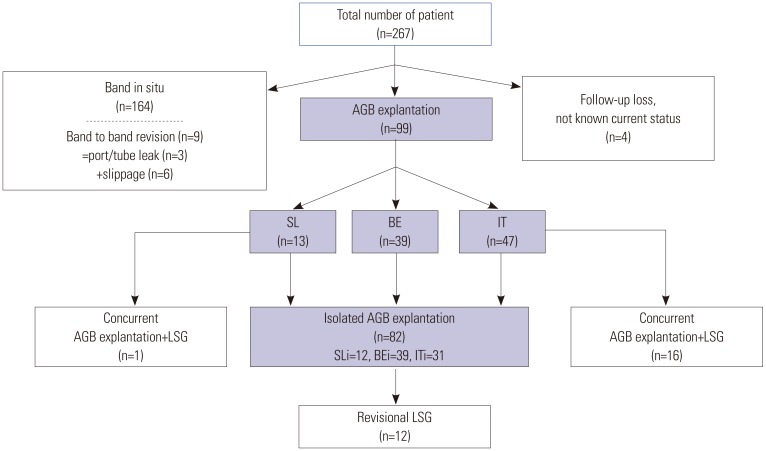
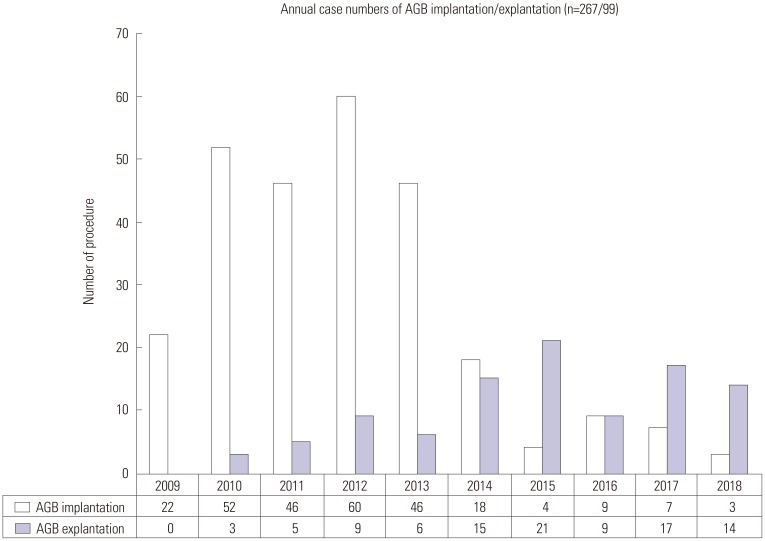
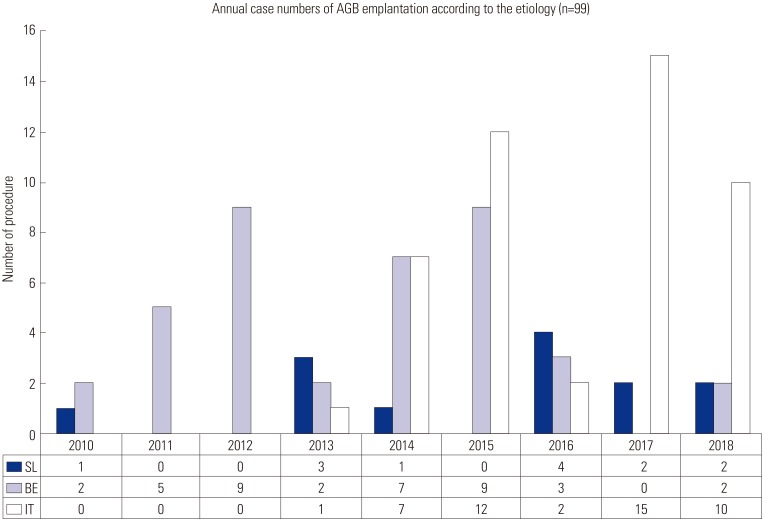
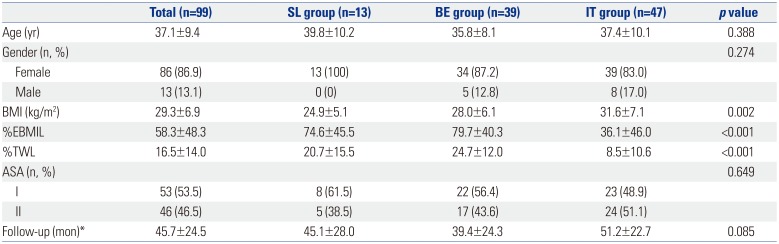
Between January 2009 and October 2018, 267 patients underwent primary AGB implantation at Gachon University Gil Medical Center, and of these 267 patients, 99 (37.1%) underwent AGB explantation. Four (1.6%) patients were lost to follow up, and their statuses were unknown at the time of writing. 164 (61.4%) patients had a band in situ. Band to band revision was performed in 9 of these 164 patients (three cases of AGB change due to system leaks and six cases of AGB explantation/immediate replacement due to acute or chronic slippage) (Fig. 1). Numbers of primary AGB implantation peaked in 2012 and then began to decline. Numbers of patients that underwent AGB explantation or conversion increased annually over the 10-year study period, and in 2015, the number of AGB explantation procedures started to exceed the number of implantations (Fig. 2). Mean band times in situ (months) in the SL, BE, and IT groups were 45.1±28.0, 39.4±24.3, and 51.2±22.7, respectively. AGB explantation occurred earlier in the BE group than in the other two groups, and AGB explantation of the IT group occurred later than in the other two groups, although it was not statistically significant (p=0.085) (Table 1, Fig. 3).
Demographic and anthropometric data of patients that underwent AGB explantation according to primary indication (n=99)
For 99 patients that underwent AGB explantation, 13 (13.1%), 39 (39.4), and 47 (47.5%) were assigned to the SL, BE, and IT groups, respectively. Mean ages of patients in these groups were 39.8±10.2, 35.8±8.1, and 37.4±10.1, respectively (p=0.388), and numbers (%) of females were 13 (100%), 34 (87.2%), and 39 (83.0%), respectively (p=0.274). Mean BMIs (kg/m2) at AGB removal in the SL, BE, and IT groups were 24.9±5.1, 28.0±6.1, and 31.6±7.1 (p=0.002); mean %EBMIL values were 74.6±45.5, 79.7±40.3, and 36.1±46.0, respectively (p<0.001); mean %TWL values were 20.7±15.5, 24.7±12.0, and 8.5±10.6, respectively (p<0.001), and numbers (%) of the American Society of Anesthesiologists physical status classification system class II patients were 5 (38.5%), 17 (43.6%), and 24 (51.1%), respectively (p=0.649) (Table 1).
Perioperative data of patients that underwent isolated AGB explantation (n=82)
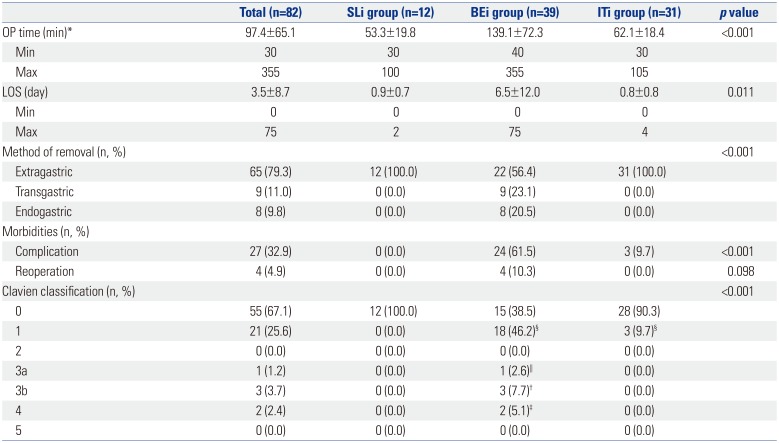
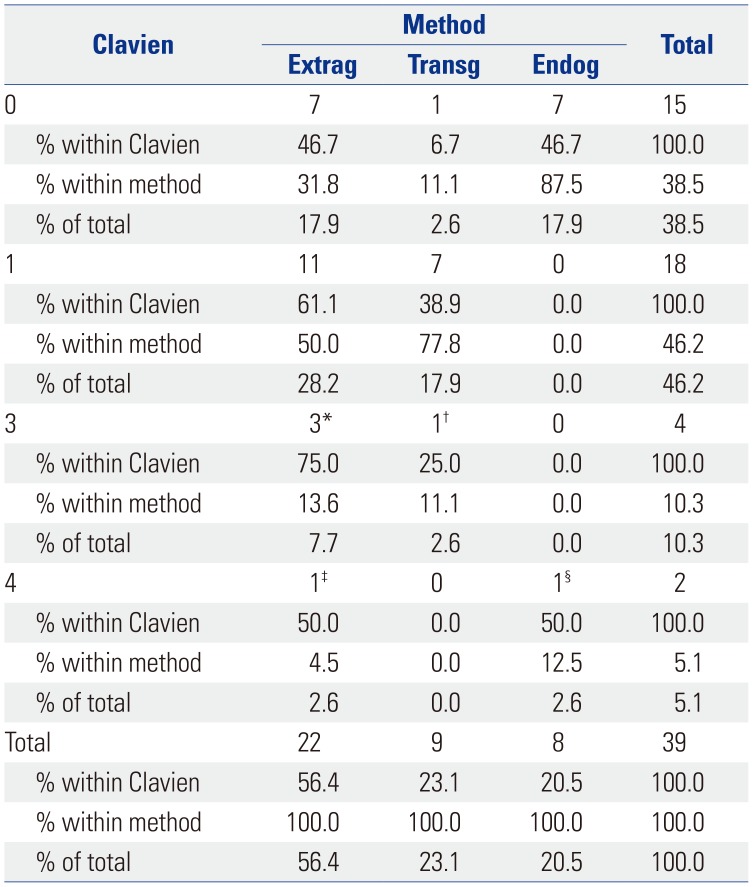
Isolated AGB explantation was performed for slippage (SLi, n=12), band erosion (BEi, n=39), or intolerance (ITi, n=31). Mean operative times required for explantation (min) in these groups were 53.3±19.8, 139.1±72.3, and 62.1±18.4, respectively (p<0.001), and mean postoperative hospital stays were 0.9±0.7, 6.5±12.0, and 0.8±0.8 days, respectively (p=0.011). In SLi and ITi groups, explantation was performed in all patients using the extragastric approach. In the BEi group (n=39), an extragastric approach was used in 22 (56.4%) patients, a transgastric approach in 9 (23.1%), and an endoscopic approach in 8 (20.5%) (p<0.001). The numbers (%) of patients that experienced a surgical complication (Clavien-Dindo class ≥1) immediately after AGB explantation in the SLi, BEi, and ITi groups were 0 (0.0%), 24 (61.5%), and 3 (9.7%), respectively (p<0.001). In the BEi group, four patients (4/39, 10.3%) underwent reoperation after AGB explantation, two underwent re-laparoscopy for an intra-abdominal abscess, one patient underwent laparotomy for a huge intra-abdominal abscess, and one underwent laparotomy for intragastric bleeding after endoscopic AGB removal. For 2 patients, percutaneous drainage (PCD) insertion was required to drain an intra-abdominal abscess (Tables 2 and 3).
DISCUSSION
Using a database at a single academic center, we examined the prevalences of AGB implantation and explantation by a single surgeon over a 10-year period. A steady increase in the popularity of AGB implantation was observed between 2009 and 2012, followed by a steady decline. In addition, we found that the number of AGB explantations increased annually from 2010, and that in 2015, the number of explantations exceeded that of implantations.
AGB is still advertised as “being designed for long-term use and to be reversed or removed if desired.” However, during our initial 10 years of experience, we found that 37.1% of bands had to be removed for slippage, erosion, or finally intolerance. Given that the number of AGB implantations is dramatically decreasing, but the number of explantations is increasing, it seems likely that the number of explantations will far exceed the number implantations in the near future. These findings and trends demonstrate AGB should no longer be considered adequate for long-term use. Furthermore, none of our 47 patients of band intolerance desired AGB explantation, but band removal was necessary due to incapacitating symptoms associated with band adjustment and suboptimal weight loss. As far as reversibility is concerned, AGB explantation is not without risks. In particular, we found explantation of an eroded gastric band to be associated with longer postoperative hospital stay (6.5±12.0 days), a high serious morbidity rate (Clavien 3a, 3b in 10.3%), and a high percentage of intensive care unit admissions (Clavien 4 in 5.1%). Other studies have similarly shown that AGB revision or explantation procedures are associated with higher rates of morbidity than primary AGB implantation.192021 In the present study, the incidence of severe morbidities associated with AGB explantation was higher than in other similar studies, which we believe was because half of the serious complications encountered in the present study occurred during the initial period (2010–2011), when our experience with eroded AGB explantation was not sufficient.17
We observed that AGB implantation peaked in 2012 and that this was followed by a dramatic decline over subsequent years. The reason for this decline is likely to be multifactorial and to include the introduction and increasing use of SG for the treatment of morbid obesity22 and the late complications (e.g., slippage, erosion, and intolerance) associated with AGB. Furthermore, the death of a celebrity after AGB surgery was well publicized in 2013 and 2014 in our country, and up until that time, the incidence of AGB implantation was far greater than that of SG or gastric bypass. Overall, the better outcomes achieved by SG in terms of weight loss and morbidity have contributed to its popularity and accelerated the decline in AGB surgery over recent years. Today, SG is the dominant procedure (43.6%) in our country, followed by gastric bypass surgery (13.5%).23
Slippage and erosion are typical major long-term complications of AGB and require band explantation.10 However, in the present study, the most common indication for band explantation was band intolerance (47.5%, 47/99), which was followed by band erosion (39.4%, 39/99) and slippage (13.1%, 11/99). Our practice started in 2009, and thus, it post-dated the era of perigastric AGB implantation, which is known to be associated with a high band slippage rate.24 Furthermore, we do not recommend AGB removal in all cases of band slippage: we have adopted a protocol of complete band deflation, followed by gradual inflation or removal and immediate replacement.14 During the early study period, band erosion was the main reason for AGB removal (Fig. 3), although subsequent improvements in surgical techniques and postoperative care probably changed this situation. However, in the present study, this observation lacked significance due to the low number of BE patients. The mean times for maintaining the band in situ in the SL, BE, and IT groups were 45.1±28.0, 39.4±24.3, and 51.2±22.7 months, respectively. Furthermore, AGB removal in the IT group tended to occur later than in the other two groups (p=0.085). This means that even if AGB patients “overcome” slippage or erosion in the short-term, many are still at risk of developing intolerance in the long-term. Based on these results, the number of patients with band intolerance will increase with follow-up duration. Lastly, due to the increased popularity of SG, many patient with band intolerance request AGB removal with concurrent SG. In fact, around a third of patients (16/47) in the intolerance group underwent concurrent surgery (Fig. 1), mainly during the period 2014–2018. Thus, had it not been for the higher efficacy and increased popularity of other surgical techniques like SG, many patients in our IT group would maintain their bands in situ with conservative management.
In the present study, severe complications after band explantation happened mainly in the BE group (Table 2). In retrospect, we admit that this phenomenon was related to inexperience and the method used to remove eroded AGBs. The fibrous capsule around an eroded band is actually ‘unhealthy’ phlegmonous tissue. Thus, after band removal, closure of the remaining gastric perforation is difficult, and repaired gastrostomies are more prone to leakage and breakdown. In this regard, transgastric removal, which is a laparoscopic gastrostomy with intraluminal division and eroded band removal, appears a more relevant procedure.25 In our study, the majority of mild complications (Clavien 1) were due to a postoperative spiking fever of a duration of 2–3 days (Table 2). In our experience, postoperative fever after eroded gastric band removal is common, and is probably due to minor leakage through the repaired gastrotomy or contamination of the operative field during infected band removal. Although antipyretic/antibiotic-based conservative treatment is sufficient in these patients, we encountered five cases of intra-abdominal abscess requiring further procedures (two PCD insertions and three reoperations for wash out and drainage). Recent reports indicate endoscopic removal of the eroded band is feasible. Ten of our patients underwent endoscopic removal, which was successful in 7 patients, which is in-line with success rates reported in other series.26272829 In one of the other 3 patients, contrary to endoscopic findings, band migration was not sufficient for removal, and therefore, we could not hook the band with wire. In another, the procedure was abandoned because after hooking the band, the wire broke instead of the band. Both of these patients underwent laparoscopic removal. In the remaining patient, after successful endoscopic removal, reoperation was performed for delayed intragastric bleeding. Our experiences of a small number of patients caution that endoscopic removal should be tried only for Nocca stage III patients with a band (including band buckle) exhibiting near total intragastric migration. After successful endoscopic removal, patients should be monitored overnight for possible delayed bleeding. Notably, during the migration of an eroded band, small branches of the left gastric artery can also be eroded, and these represent potential sources of massive bleeding after band removal, because the band can act as a tamponade. A case of this type was reported during the laparoscopic removal of an eroded band.30
Our study has several limitations that deserve mention. First, it is limited by its retrospective nature, by a relatively small cohort, with by a follow-up of <10 years. It has been suggested in more long-term studies that the earlier reported high frequencies of late adverse events have reduced markedly.1131 However, we believe that this study is the first and largest study from an academic center dealing with AGB in Korea. Second, we included patients that underwent AGB implantation during our learning period, which may have adversely affected incidences of severe complications. However, one of our aims was to present with transparency our experiences of 10 years of clinical practice with AGB. Lastly, unlike the definitions of slippage or erosion, the definition of intolerance was rather arbitrary. Although we defined intolerance as a sum of functional and psychologic intolerance as determined by an upper GI swallow study and gastroscopy, patients were very heterogenous in terms of amount of weight loss, food tolerance, amount of saline within the band, symptoms of esophagitis, and morphologies of distal esophagus or pouch superior to bands. Similar phenomena have been discussed in the literature.3233 However, from the clinical point of view, intolerance can be safely defined as “a non-slippage and non-erosion long complication of AGB.” Based on our clinical experience, many patients having intolerance (unlike slippage) have symptoms with inflated band. However, for fear of gaining weight, they are prone to refuse too much deflation or later removal.
In conclusion, during 10 years of clinical practice, 37.1% of our patients underwent AGB explantation. The most common indication for band explantation was band intolerance, and this was followed by band erosion and slippage. Intra-abdominal abscess and intragastric bleeding were rare, but serious complications encountered after eroded gastric band removal. Although the results of our study do not discourage AGB use, potential candidates should be informed of the long-term high risk of the need for band explantation and its associated morbidities.
 XML Download
XML Download