

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Drug-induced parkinsonism (DIP) presents with symptoms, such as rigidity, postural instability, and gait disturbance, which also occur in idiopathic Parkinson disease (IPD). Most cases of DIP can be cured by discontinuing the offending drugs, whereas IPD becomes exacerbated over time. However, some DIP patients do not recover completely after discontinuation of the offending drugs.12 Approximately 20–22% of IPD patients are ultimately diagnosed with DIP.34 Furthermore, patients taking offending drugs have a 1.9–3.2 times higher possibility of developing Parkinson disease than those who do not.56 Therefore, to cure DIP and to decrease the risk of IPD, it is very important for doctors to differentiate whether a patient presenting with Parkinsonism is a case of DIP. In patients with DIP, it is necessary to identify which offending drugs the patient uses and to reduce the usage of those drugs to the greatest extent possible.
The most commonly used offending drugs have changed over time. In the past, DIP was commonly reported to be caused by antipsychotics, while today, the common offending drugs are atypical neuroleptics, benzamide derivatives (metoclopramide, levosulpiride, and clebopride), and calcium channel-blocking agents (flunarizine and cinnarizine).789 There are some differences among countries in the utilization of offending drugs. Some benzamide derivatives, such as levosulpiride, clebopride, and itopride, are not approved for use in the United States or United Kingdom,1011 although they are prescribed to many people in Korea.12
To reduce the occurrence of DIP, the epidemiological characteristics of DIP should be clearly understood. However, little research has investigated the current status of DIP and the use of offending drugs. The aim of this study was to estimate the prevalence of DIP through an analysis of the Korean National Health Insurance Claims (KNHIC) database. Trends in the utilization of offending drugs were investigated in this study as well.
MATERIALS AND METHODS
Data source
This study used the KNHIC database, which contains data from all hospitals and clinics concerning the health care services that they provide to their patients. This cumulative database includes individual data from the entire Korean population, with information on age, sex, diagnosis according to International Classification of Disease and Related Health Problems 10th revision (ICD-10) codes, date of diagnosis, medication adherence, insurance type, institutional characteristics of the healthcare provider, and the requested medical care costs. We obtained the data related to DIP patients in the KNHIC database from the National Health Insurance Service (NHIS).
Study population and offending drugs
We defined DIP patients as people who were aged 40–100 years old and had a diagnosis code for DIP (ICD-10: G21.1) as a principal diagnosis in 2009–2015. Those who were registered as having IPD (extra benefit code: V124) and who died in the year of diagnosis were excluded. Patients were classified according to whether they had used offending drugs before or after DIP diagnosis. The former group comprised DIP patients who were prescribed an offending drug for at least 28 days over the course of 1 year before the DIP diagnosis, and the latter group comprised DIP patients who were prescribed an offending drug for at least 28 days over the course of 6 months after the DIP diagnosis.13 This study used the list of offending drugs reported in a previous study913 that have been approved by the Korean Ministry of Food and Drug Safety. The previous study classified the offending drugs depending on the potential risk levels of DIP. The list of drugs that may cause DIP is provided in Supplementary Table 1 (only online). The high-risk group contains dopamine D2 receptor antagonists (haloperidol, pimozide, amisulpride, levomepromazine, promazine, sulpiride, risperidone, olanzapine, aripiprazole, and ziprasidone), dopamine depleters (tetrabenazine), and calcium channel antagonists (P-channel: flunarizine). The intermediate-risk group includes atypical antipsychotics (ziprasidone), antiemetic and gastrointestinal motility agents (metoclopramide, levosulpiride, clebopride, and itopride), calcium channel antagonists (L-channel: verapamil and diltiazem), and others (lithium and valproate). The low-risk group includes selective serotonin reuptake inhibitors (fluoxetine and sertraline), monoamine oxidase inhibitors (moclobemide), and others (amiodarone, procaine, and cyclosporin).914 We analyzed the proportion of offending drugs used before and after the DIP diagnosis in 2015 and the frequency of utilization of the offending drugs, focusing on the top five most frequently prescribed drugs by age.
Statistical analysis
The annual prevalence of DIP from 2009 to 2015 was calculated using age- and sex-standardized methods based on data regarding the population distribution issued by the Korea National Statistical Office in 2015. Trends in prevalence were estimated using the compound annual growth rate (CAGR) and Cochran-Armitage test (CAT) for DIP over 6 years. The CAGR was used to explore growth in a more precise, annualized manner. The CAGR was estimated with the formula [(ending value/beginning value)(1/no. of years)]−1.15 A null hypothesis in the CAT is the hypothesis of no trend, which would indicate an equal binomial proportion for all levels of the explanatory variable.16 Statistical significance was evaluated by applying two-tailed tests, and p values <0.05 were considered to indicate statistical significance. All statistical analyses were performed using version 9.4 (SAS institute, Cary, NC, USA)
RESULTS
Prevalence of DIP in 2009–2015
The total number of DIP cases was 859 in 2009, and it increased to 1840 in 2015. Of the DIP patients recorded in 2015, offending drugs had been used by 1285 (69.83%). The remaining DIP patients may have taken an offending drug for fewer than 28 days over the course of 1 year before DIP diagnosis. Genetic differences may also have been a relevant factor, as a previous study reported that not all patients using dopamine receptor blocking agents experience Parkinsonism, suggesting that genetic factors may affect the occurrence of DIP.7 The annual prevalences of DIP, standardizing the population by age and sex to 2015 values, were 4.09 per 100000 in 2009 and 7.02 in 2015. The prevalence of DIP was highest in 2015. The CAGR increased by 9.42%, and this increasing trend was statistically significant. Table 1 shows the annual prevalence rates of DIP per 100000 people according to sex. The annual prevalence of DIP among females was 1.98 times higher than that among males. The CAGR increased more in men (8.68%) than in women (9.82%). Between 2009 and 2015, the prevalence was highest in individuals aged 70–79 years and was lowest in those aged 40–59 years. In the former group, CAGRs were 14.6 per 100000 people in 2009 and 24.0 in 2015. However, for the latter group, they were 0.6 in 2009 and 1.5 in 2015. The CAGR increased in every age group (Fig. 1).
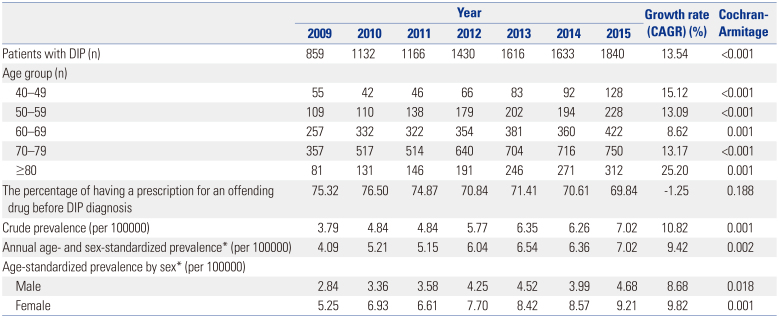
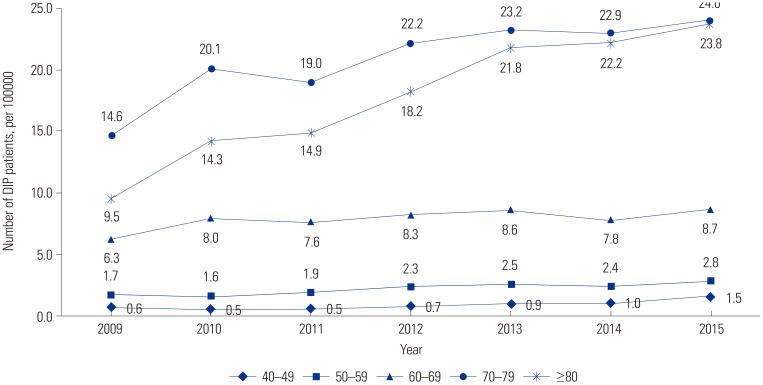
Table 1
Prevalence of Drug-Induced Parkinsonism
![]()
Utilization of offending drugs
Offending drugs used before DIP diagnosis
Offending drugs were identified by classifying DIP patients who were prescribed an offending drug for at least 28 days over the course of 1 year prior to the index date (1285 people). The index date was defined as the date of the first diagnosis of DIP. The offending drugs that DIP patients were most commonly prescribed were antiemetic and gastrointestinal motility agents (68.40%), followed by atypical antipsychotics (38.21%) and typical antipsychotics (23.66%) (Table 2). We then investigated the utilization of causative drugs among those who had been prescribed an offending drug for at least 28 days.
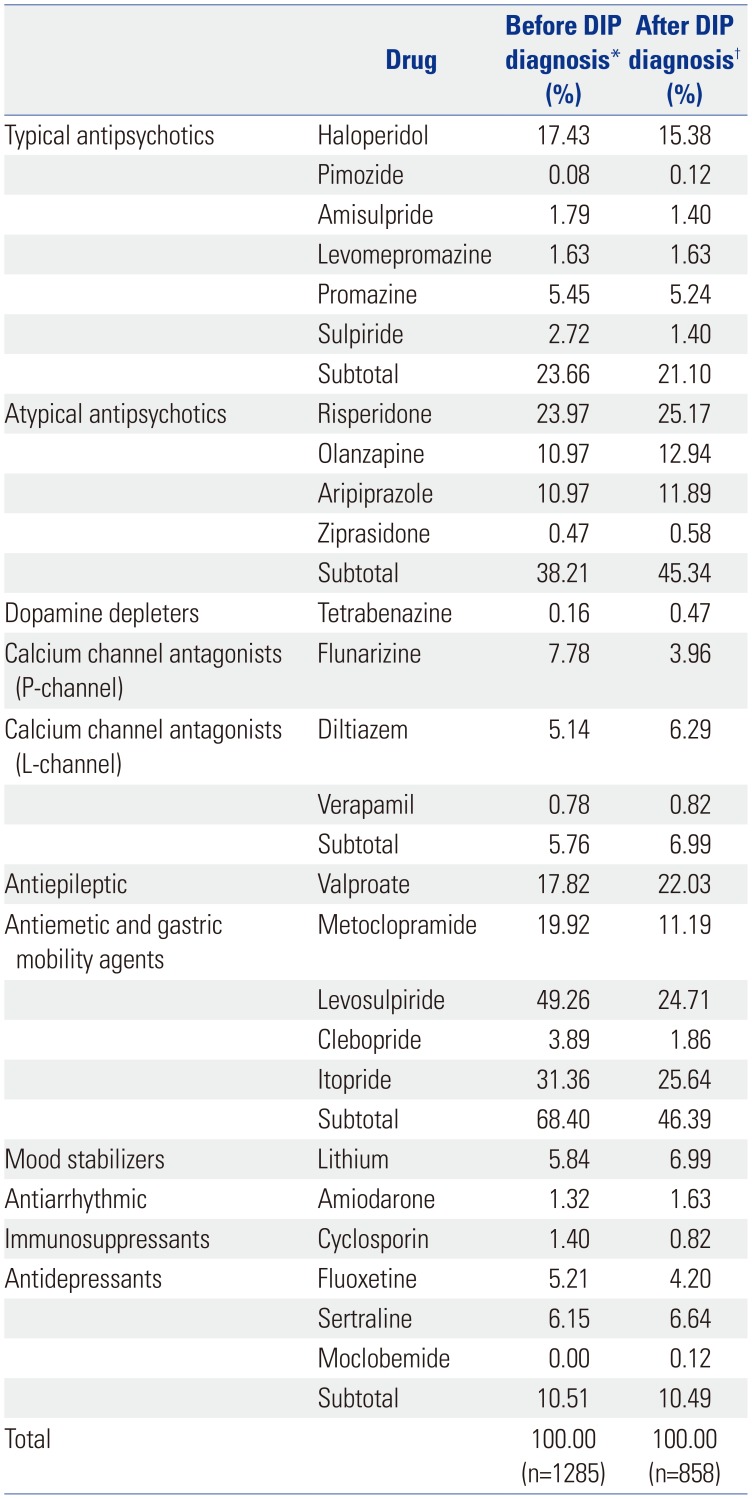
Table 2
Utilization of Offending Drugs before and after DIP Diagnosis in 2015
DIP, drug-induced parkinsonism.
*Before DIP diagnosis (%): 1) Numerator: DIP patients who were prescribed the offending drug. 2) Denominator: DIP patients who were prescribed an offending drug for at least 28 days over the course of 1 year before DIP diagnosis; †After DIP diagnosis (%): 1) Numerator: DIP patients who were prescribed the offending drug. 2) Denominator: DIP patients who were prescribed an offending drug for at least 28 days over the course of 6 months after DIP diagnosis.
![]()
We identified the five most frequently used offending drugs. In 2009, the most common offending drug was levosulpiride (68.62%), followed by itopride (30.76%), risperidone (15.30%), metoclopramide (43.43%), and valproate (12.98%). In 2015, levosulpiride (49.26%) was still the most frequently prescribed offending drug, followed by itopride (31.36%), risperidone (23.97%), metoclopramide (19.92%), and valproate (17.82%). The offending drugs most commonly used by individuals ≤59 years of age and those ≥60 years of age were risperidone and levosulpiride, respectively. Notable differences were found by age group. Individuals 59 years of age or younger used antipsychotic drugs more frequently, whereas those aged 60 years or over were more likely to be prescribed antiemetic and gastric mobility agents.
Among the antiemetic and gastrointestinal motility agents, levosulpiride showed a clear trend for decreasing utilization in all age groups. The CAGR of levosulpiride utilization decreased by 5.38% (p<0.001). Metoclopramide utilization decreased by a mean annual average of over 10% (p<0.001). Meanwhile, the CAGRs for risperidone and valproate utilization increased by 7.77% (p=0.019) and 5.42% ((p=0.208), respectively (Table 3).
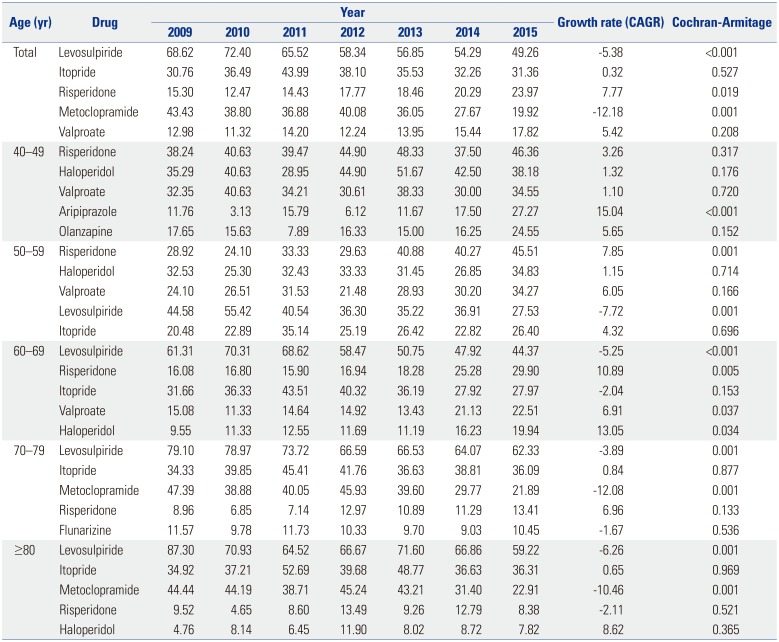
Table 3
The Five Offending Drugs Most Commonly Used before DIP Diagnosis (%)
![]()
Offending drugs used after DIP diagnosis
The use of offending drugs after the DIP diagnosis was defined by identifying patients who were prescribed an offending drug for at least 28 days over the course of 6 months after being diagnosed with DIP. In 2009, the rate was 41.61%, and it increased by an average of 0.69% each year. The over-70 group showed a decrease in the utilization of offending drugs after being diagnosed with DIP. However, the age group of 40–49 showed a remarkable average annual increase of 6.45% (p<0.001). In 2015, the age group of 40–49 had the highest rate of continuing prescriptions (82.03%), and this trend was seen in all age groups (Table 4).
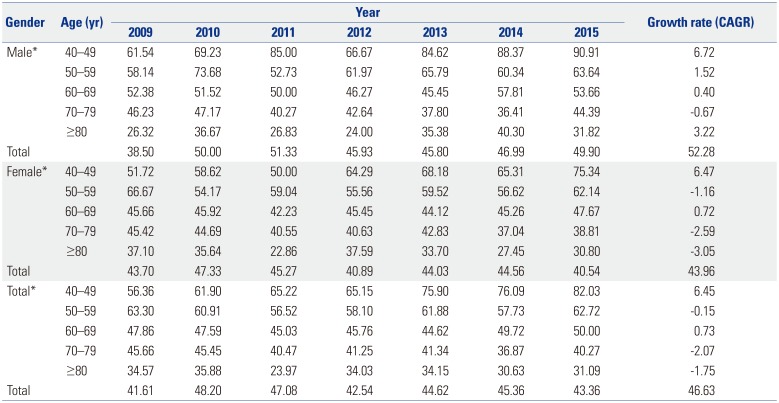
Table 4
Prescription of Offending Drugs within 6 Months after DIP Diagnosis
![]()
We investigated the types of offending drugs that were prescribed for at least 28 days over the course of 6 months after the index date, and the results were similar to those obtained for offending drug prescriptions before the index date. DIP patients who were prescribed antiemetic and gastrointestinal motility agents accounted for the highest percentage of the entire group (25.64%), followed by those who were prescribed atypical antipsychotics (24.7%) and antiepileptic (15.38%).
In 2015 the most commonly prescribed offending drug was levosulpiride (25.64%), followed by itopride (25.17%), risperidone (24.71%), metoclopramide (22.03%), and valproate (15.38%). Levosulpiride was the most widely used drug in all age groups, although its mean annual growth rate decreased by 4.28% ((p=0.009). In contrast, the rate of itopride utilization consistently increased. The CAGR of itopride, which is also an antiemetic and gastrointestinal motility agent, plunged by 12.65% ((p=0.004). Physicians might consider itopride to be a less-risky alternative to levosulpiride (Table 5).
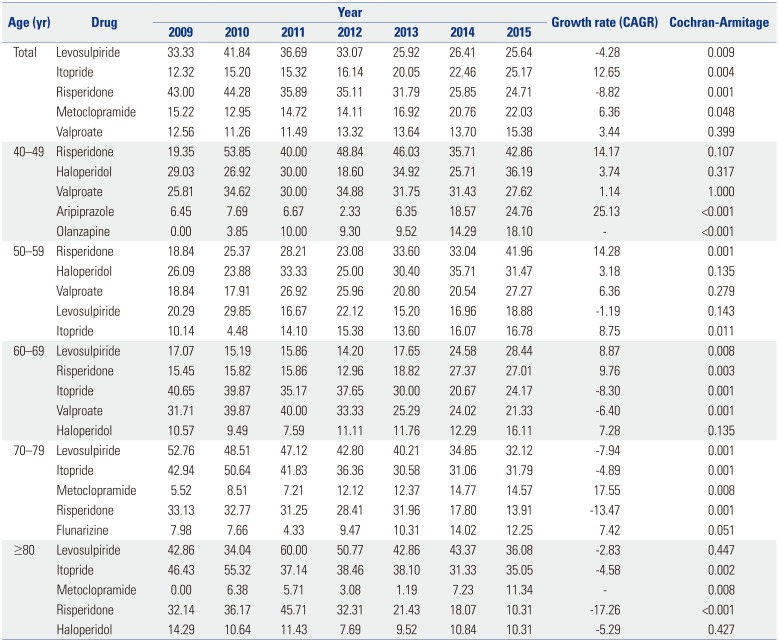
Table 5
The Five Offending Drugs Most Commonly Used after DIP Diagnosis (%)
![]()
Additionally, the rate of risperidone utilization consistently decreased by an average of 8.82% (p<0.05) each year. The rate of valproate utilization consistently increased, and its mean annual growth rate showed an increase of 3.44% ((p=0.400). Physicians might have switched to prescribing other drugs as less-risky alternatives to risperidone, with the exception of cases in which risperidone is essential for the treatment plan and it is impossible to change the prescription.
DISCUSSION
This study analyzed the prevalence of DIP from 2009 to 2015 using the NHIS database. DIP is generally characterized by the absence of symptoms of Parkinsonism before the use of an offending drug and by resolution of the symptoms within 6 months of the withdrawal of that drug.17 To calculate DIP prevalence using a nationwide large-scale database, which is distinct from using patients' medical records, an operational definition of DIP is needed. In this study, when a doctor used a DIP diagnostic code as the principal diagnosis, that patient was defined as having DIP. The problem with this definition is that many patients with DIP may be misdiagnosed with IPD because the clinical features of these two conditions are indistinguishable.7 In addition, because the NHIS database is a medical utilization record, this does not include people who did not visit medical institutions. As a result, the actual number of DIP patients could have been underestimated.
According to the results of this study, there were 7.02 DIP patients per 100000 people aged 40–100 years in 2015. Among those aged 70–79, there were 24.0 patients per 100000 in 2015. Few previous studies have investigated the prevalence of DIP using nationwide administrative data. In one study in Brazil, a prevalence of DIP of 2.7% was estimated using a communitybased survey.16 In three regions of Spain, a prevalence of 0.49% was calculated using the door-to-door method among older adults.3418 However, it is difficult to compare these results, since the definition of patients and research methods used were different in each study.
Our study found that DIP was more common in women than in men in all age groups. Female has consistently been reported as a risk factor for DIP.819 The underlying mechanisms are unknown, and genetic, endocrine, social, and cultural differences may contribute to the higher prevalence of DIP in women. In general, old age is known to be a risk factor for DIP,3 which this study confirmed using large-scale nationwide data. The increasing risk of DIP with age reflects the frequent use of dopamine-blocking agents in recent years for the control of mental disorders with agitation, confusion, delirium, and anxiety.17
There are no clinical criteria for how long offending drugs must be used to cause DIP symptoms. However, since the length of treatment is a risk factor for DIP, we investigated the types of offending drugs used by DIP patients who had been prescribed them for at least 28 days during the 1-year period prior to the index date.
Antiemetic and gastric mobility agents, particularly levosulpiride, were the offending drugs most commonly used by DIP patients. Atypical antipsychotics were the next most frequently used type. Antiemetic and gastric mobility agents, such as levosulpiride, clebopride, and itopride, are not approved in the United States or United Kingdom.
Remarkably, between 2009 and 2015, the usage of levosulpiride drastically decreased while the usage of itopride increased slightly. This downward trend in levosulpiride utilization may have been due to studies reporting the occurrence of DIP caused by levosulpiride,20212223 which may reflect differences in the ability of levosulpiride and itopride to penetrate the central nervous system.
With respect to therapeutic class, both levosulpiride and itopride are benzamide derivatives, although they have slightly different mechanisms. According to a previous study, levosulpiride has a high affinity (Ki: 27–134 nM) for dopamine 2 receptor antagonism and targets selective dopamine presynaptic auto-receptors in the central nervous system.24 In contrast, itopride has the same effect in terms of dopamine 2 receptor antagonism, but little effect on the central nervous system.25 Similarly to other reported results,26 the time trend of DIP prevalence in all age groups decreased over this recent 7-year period, which may have been related to changes in the usage of prokinetics, including levosulpiride and itopride. Although their CAGRs clearly decreased, these drugs are still frequently and readily prescribed in Korea. Although prokinetics have a low potency for dopamine receptor blocking, they can cause DIP and have also been shown to be associated with cognitive dysfunction.22
Over 40% of patients continued to use offending drugs after being diagnosed with DIP. In particular, the age group of 40–49 received the most atypical antipsychotic prescriptions for treatment, whereas the age group of 70–79 took the most antiemetic and gastric mobility agents. We believe that physicians regularly prescribe these drugs to treat patients younger than 60 years old. Doctors commonly prescribed benzamide derivatives, such as levosulpiride, itopride, and metoclopramide, in the over-60 group after DIP diagnosis. It is need that physicians pay more attention to prescription patterns in patients who are older than 60.
To prevent and cure DIP, doctors need to reduce the utilization of offending drugs and to find less-risky substitutes. Checking a patient's medication history after the onset of Parkinsonism is also important. In particular, in older adult patients who are at high risk for both DIP and IPD, the long-term use of offending drugs should be considered more carefully and, if necessary, be limited. Additionally, it is necessary to emphasize the need for continuous education on offending drugs.
This is the first representative study to estimate the prevalence of DIP and to identify the usage patterns of offending drugs among the Korean population. Despite these contributions, our study has several limitations. First, we used prescription claims data, so we could not identify whether patients actually took the prescribed medicines. Second, the diagnosis of DIP was determined in this study using an operational definition. Since some doctors may not have recognized DIP in their patients, some patients might have not been included in this study.
 XML Download
XML Download