

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
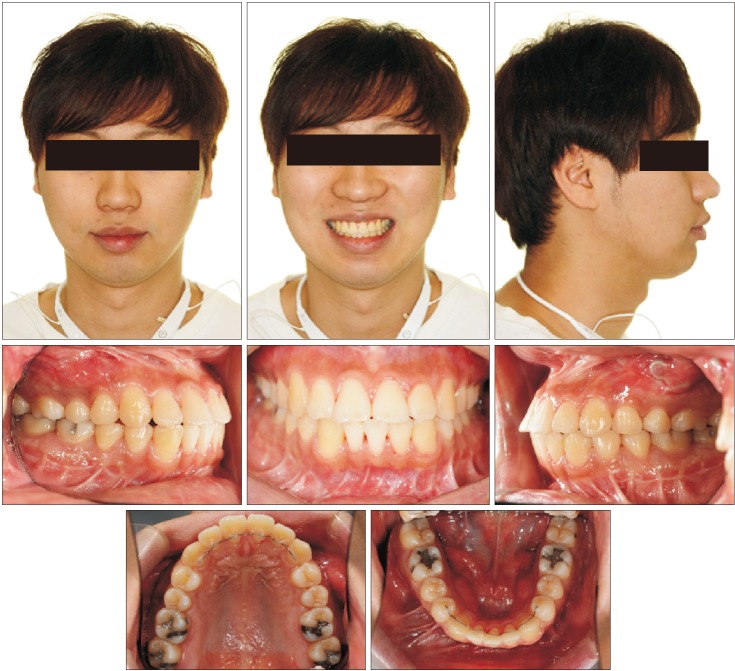
DIAGNOSIS AND ETIOLOGY

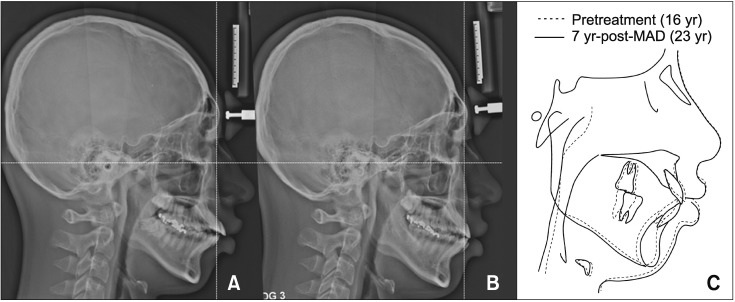 | Figure 3Lateral cephalograms. A, Pretreatment. B, After 7 years of wearing the mandibular advancement device (MAD). C, Superimposition of A and B.
|
Table 2
Comparison of the lateral cephalometric measurements of craniofacial, dentoalveolar, and pharyngeal airway parameters among the four observation time points
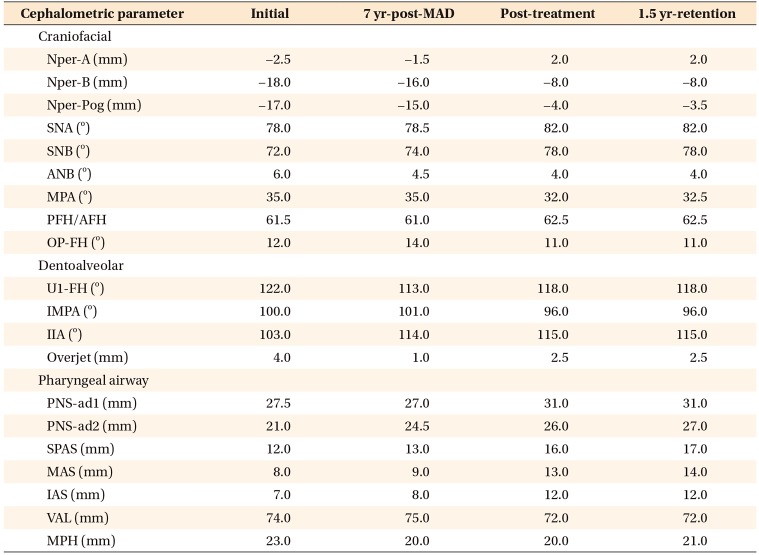
MAD, Mandibular advancement device; Nper-A, perpendicular distance between A point and nasion perpendicular line; Nper-B, perpendicular distance between B point and nasion perpendicular line; Nper-Pog, perpendicular distance between pogonion and nasion perpendicular line; SNA, angle between lines sella-nasion and nasion-point A; SNB, angle between lines sella-nasion and nasion-point B; ANB, angle between lines point A-nasion and nasion-point B; mandibular plane angle (MPA), angle between lines gonial-menton and Frankfort horizontal line; posterior facial height/anterior facial height (PFH/AFH), ratio between linear distance from sella to gonion and from nasion to menton; OP-FH, angle formed by the lines between occlusal plane and Frankfort horizontal line; U1-FH, angle formed by the lines between long axis of upper incisor and Frankfort horizontal line; incisor mandibular plane angle (IMPA), angle formed by the lines between long axis of lower incisor and mandibular plane angle; inter incisor angle (IIA), angle formed by the lines between long axis of upper incisor and lower incisor; PNS-ad1, linear distance from posterior nasal spine to the point ad1 (ad1, intersection of the line PNSBasion and the posterior nasopharyngeal wall); PNS-ad2, linear distance from posterior nasal spine to the point ad2 (ad2, the intersection of the posterior nasopharyngeal wall and the midpoint on the line joining sella and basion); superior posterior airway space (SPAS), the thickness of the airway behind the soft palate along a line parallel to gonion-point B; middle airway space (MAS), the thickness of the airway along a line parallel to gonion-point B through the lowest point of soft palate; inferior airway space (IAS), the thickness of the airway along a line extended through gonion-point B; vertical airway length (VAL), the linear distance between posterior nasal spine to epiglottis base; mandibular plane to hyoid (MPH), linear distance along a perpendicular from hyoid bone to the mandibular plane.
![]()
TREATMENT OBJECTIVES
TREATMENT ALTERNATIVES
TREATMENT PROGRESS

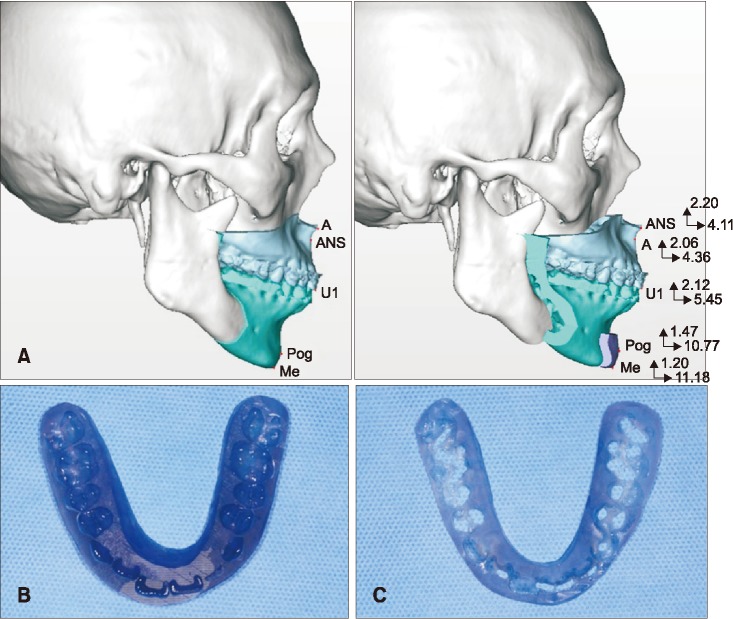 | Figure 6Computer-assisted three-dimensional (3D) planning of maxillomandibular advancement surgery with genioplasty using Simplant Pro software (Materialize Dental, Leuven, Belgium) (A), 3D printed intermediate wafer (B), and final wafer (C).A, Point A; ANS, anterior nasal spine; U1, upper central incisor; Pog, pogonion; Me, menton.
|
RESULTS
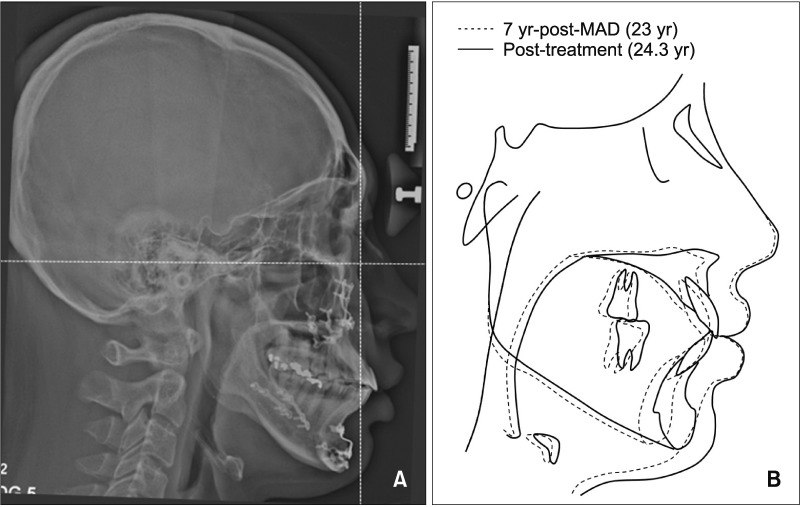 | Figure 7A, Lateral cephalograms taken at post-treatment. B, Superimposition of alignment after 7 years of wearing the mandibular advancement device (MAD) (7 yr-post-MAD) and post-treatment.
|


 XML Download
XML Download